Genderaspekte in der Substanzgebrauchsstörung - Universitätsspital Zürich Klinik für Konsiliarpsychiatrie & Psychosomatik ...
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Universitätsspital Zürich
Klinik für Konsiliarpsychiatrie & Psychosomatik
9.11.2020
- Virtuelles Seminar -
Genderaspekte in der
Substanzgebrauchsstörung
Zentrum für Public Health
Univ. Klinik für Psychiatrie & Psychotherapie
gabriele.fischer@meduniwien.ac.at
OP-CAT Kommission 3
Disclosure • Keine Interessenskonflikte bzgl. Inhaltes der Präsentation
Struktur
• Allgemeines
– Geschlechtsstereotypien
– Sexismus: „Führungsstil“
• Kosten durch psychiatr. Erkrankungen
• Psychiatrische Erkrankungen
– am Beispiel der Substanzgebrauchsstörung mit
• somatischen Konsequenzen
Geschlechtsstereotyp
Kreislauf sich selbst erfüllender Prophezeiung
Aufgrund der Geschlechterstereotype werden Erwartungen gebildet,
die sich in unterschiedlicher Weise an weibliche und männliche
Personen richtet.
• Aufgrund der Tendenz zur kognitiven Konsistenz („stimmiger“
Eindruck) werden ankommende Informationen der Zielperson in
verzerrter Form (abhängig von bestehenden Erwartungen)
aufgenommen, verarbeitet und behalten
• Es kommt zu einer erwartungskonformen kognitiven „Abbildung“
der Zielperson
• Dies beeinflusst das Handeln - wenn die Zielperson wünscht,
den Erwartungen zu entsprechen - wird von ihr auch das
erwartete Verhalten „produziert“
• Damit wird das Stereotyp bekräftigt und aufrecht erhalten.
Formen des Sexismus in der Epidemiologie I • Geschlechterinsensibilität - Geschlechterdifferenzen werden ignoriert und Befunde nur an einem Geschlecht erhoben (z.B. Ätiolog. Befunde) • Geschlechterdichotomie - Unterschiede werden überbetont, Definition anhand von Stereotypen - Abweichung = krank (z.b: MMPI) • Familialismus - Familie wird als Einheit genommen ohne auf unterschiedlichen Aufgaben der einzelnen Mitglieder einzugehen (z.b. weibl. Mitglieder übernehmen Pflege)
Formen des Sexismus in der Epidemiologie II • Überverallgemeinerung - Aussagen werden formuliert, die aufgrund der Forschungslage aber nur für ein Geschlecht bekannt sind (z.b.: Medikamentenwirkung wird auf alle übertragen, obwohl nur bei einem Geschlecht geprüft) • Doppelter Bewertungsmaßstab (z.b: aggressives Verhalten wird bei Jungen als sozial angemessen gesehen, bei Mädchen deviant) • Geschlechtsverklärung - Überhöhung empirischer Geschlechts- Merkmale zu normativer Forderung (z.b. weil das eine Geschlecht so ist, wird die Sollforderung für das andere erhoben - emotionale Expressivität der Frau wird zum Maßstab der emotion. Ausdrucksfähigkeit beim Mann)

“Stolze Frauen gelten als aggressiv,
Männer als dynamisch & zielstrebig”
Brosi et al., 2016, Journal of Applied Psychology
Wissenschaftliche Studie um die Wirkung von Stolz zu untersuchen
• 400 Studierenden wurden Bilder von jungen ♀ und ♂, die ein begehrtes Stipendium gewonnen
haben gezeigt
Ø Eine Hälfte der Abgebildeten gab sich stolz, indem sie die Hände in die Hüften stemmten und
triumphal von oben herab schauten.
Ø Der andere Teil freute sich lediglich.
• Zusätzlich wurden sie mit einem kurzen Text als stolz („sehr stolz“) oder freudig („ein breites
Lächeln“) beschrieben.
• Die Studenten schätzten dann mit einem Fragebogen ein, ob die Personen auf den Fotos
selbstbewusst, warmherzig oder rücksichtslos waren und wie sie vermutlich Mitarbeiter führen
würden.
Ergebnisse
• Sowohl ♂ als auch ♀, die stolz waren, galten als selbstbewusst & kühl, sowie weniger empathisch
• Stolze ♀ & ♂ wurden eher als keine guten Chefs beschrieben
• Stolze ♀ wurden jedoch im Vergleich zu ♂ durchwegs negativer eingeschätzt:
à ♀ galten eher als aggressiv, ♂ eher als dynamisch & zielstrebig
• „Stolze“♀ näherten sich in ihren zugeschrieben Eigenschaften somit denen der ♂ an (♂ wurden
generell als tatkräftiger & forscher beschrieben; ♀ generell eher als mitmenschlicher und weniger
tatkräftig, insbesondere wenn sie lächelten)
Introduction
• Sex differences are of high scientific and societal interest because of
their prominence in behavior
• Sex differences in human behavior show adaptive complementarity
– Males have better motor and spatial abilities
– Females have superior memory and social cognition skills
• The brain can be analyzed on the whole as a large and complex
network known as the human connectome (vs. individual regions or
tracts in isolation) à capability to provide fundamental insights into
organization and integration of brain networks
• Aim of Study:
– Detailed analysis of sex differences in brain connectivity on a large sample
(♀521, ♂428) of healthy young individuals (8-22y.)1 using the diffusion-based
structural connectome of the brain
1 Young individuals were used since developmental trajectories of males and females separate at a
young age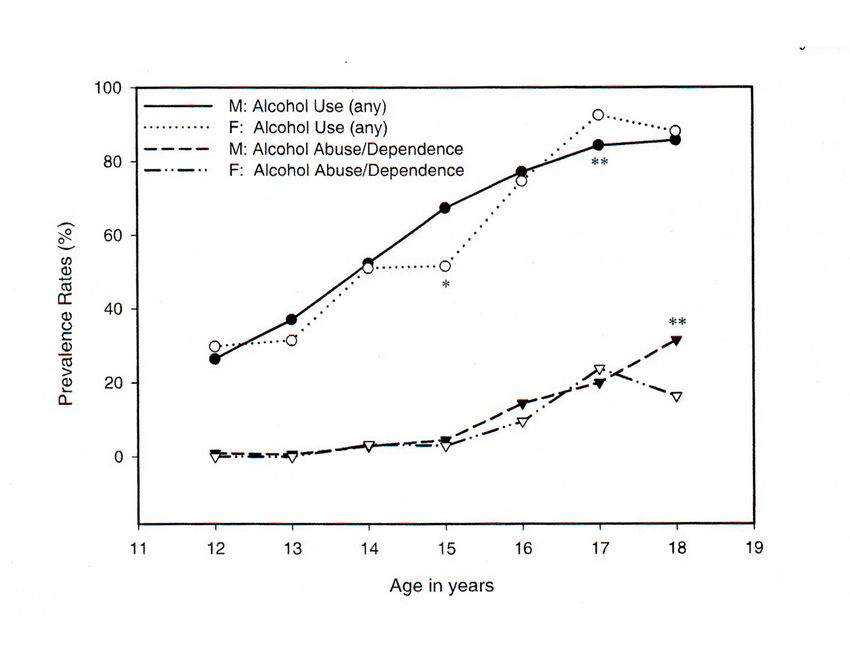
Method Schematic of the pipeline for creating the structural connectome (SC)
Results Fig. 3. Representative regions of the brain that have a higher participation coefficient (PC) at a significance level of P < 0.001. The regions have been projected onto the surface of thebrain for better visualization. Red indicates a higher PC in females, and blue indicates a higher PC in males (mainly localized to the cerebellum). Although multiple regions have higher PCs in females, the cerebellum has a higher PC in males. L, left; R, right.
Results
• Connection-based analysis:
♂ Male brains are structured to facilitate intrahemispheric cortical
connectivity, although the opposite was observed in the cerebellum
♀ In contrast, female brains displayed higher interhemispheric
connectivity
à These results were confirmed on all levels (global, lobar, regional)
♂ Greater within-hemispheric supratentorial connectivity combined
with greater cross-hemispheric cerebellar connectivity confers an
efficient system for coordinated action in males
♀ Greater interhemispheric connectivity in females facilitates
integration of the analytical and sequential reasoning modes of the
left hemisphere with the spatial, intuitive processing of information
of the right hemisphereWarum ist es sehr wichtig psychiatr. Erkrankungen zu gewichten ? • Kosten der psychiatrischen Erkrankung • Lebensqualität der psychiatrisch Kranken
Gesundheits- bzw. Krankheitskosten
Volkswirtschaftliche Belastungen durch
nicht-infektiöse Erkrankungen weltweit im
Zeitraum der Jahre 2011-2030 in Milliarden US 76 Mrd. €
Dollar 7,7% Produktivitätsverlust
8,5%
22 Mrd. € ambulante
15,6 16,3 Versorgung
18
18,8%
16 10 Mrd. €
Milliarden US Dollar
14 65% Spitalsversorgung
12
10 8,3 9 Mrd. €
8 4,8 Medikamente
6
4 1,7
2
0
et
es ge
n
g en e n
ge
n à Der Schwerpunkt der
n un ng n
ab
Di
kr
an
ku
kr
an
k
kr
an
k u
kr
an
ku
volkswirtschaftlichen Belastung
er er r Er
we
gs
Kr
e bs
lär
e E
sc
he liegt vorwiegend im
em ku hi
eA
t
dio
va
s
Ps
yc Produktivitäts-verlust (hier am
h r
i sc
ro
n Ka
Beispiel der Depression innerhalb
Ch
der EU)1
ICG Integrated Consulting Group (2012). Seelische Gesundheit in Österreich. Abrufbar unter
http://www.innenwelt.at/sites/default/files/ICG_Studie_Seelische%20Gesundheit%20in%20Österreich_Summary_2012_10
_08.pdf
1 Sobocki, Ekman, Agren, Runeson, Jönsson (2006). International Journal of Clinical Practice, 60(7), 791.798.Psychiatrische Erkrankungen – weitere
Faktoren und Kosten
Verordnungen Psychopharmaka:
2009: 1.973.660
2012: 2.168.815
à 66% Antidepressiva, 22% Beruhigungsmittel, 18% Antipsychotika
Daten: Hauptverband der Sozialversicherungsträger
Hauptursachen für Berufsunfähigkeitspensionen
50 45,7
43 44
45 42
40
40 37
33,1
35 Psychiatrische Krankheiten
30
24,4
Prozent
25 Krankheiten des
20 20 19
20
18 17 17,8 Bewegungsapparates
15 11,9 Herz-Kreislauf-Erkrankungen
10 10 9 10 10
10
8
5
0
2005 2006 2007 2008 2009 2010 2011Die Hauptursachen für DALYs
* DALYs = Maß für die weltweite Krankheitslast, ausgedrückt in der Zahl an
verlorenen Lebensjahren aufgrund von schlechter Gesundheit, Behinderung
oder frühzeitigem Tod
Bipolare Störungen
Ernährungsbed./endokrine Erkr. Bereich psychiatrischer Störungen im eigentlichen Sinne
Asthma
Somatische Krankheiten mit bedeutsamen klinisch-
psychologischen Interventionsmöglichkeiten
Migräne
Andere somatische Erkrankungen
Drogenmissbrauch/-abhängigkeit
Leberzirrhose
Selbst zugefügte Ve rletzungen
Brustkre bs
Darmkrebs
Diabetes m ellitus
Verkehrsunfälle
Entzündl. Gelenkerkrankung
Lungenkrebs
Chron. obstr. pulm. Erkr. (COPD)
Hörverlust
Alkoholmiss brauch/Abhängigkeit
Schlaganfall
De menze n
He rzinfarkt
Unipolare Depres sion
0 1 2 3 4 5 6 7 8
World Health Organization (2002). Global Burden of Disease Estimates. http://www.who.int/healthinfo/global_burden_
disease/en/index.html. (Zugegriff am 08. Jan. 2013)Gender-related differences in psychiatric and neurological
disease burden
DALY: disability-adjusted life-years; OCD: obsessive–compulsive disorder
Wittchen HU, et al. Eur Neuropsychopharmacol. 2011;21:655–79Sex and gender differences – do they
exist?
GENDER
SEX
Differences based on psychosocial
Differences based on biology
factors
Both sex and gender are influenced by:
Health-related Social factors
factors
Access to resources
Exposure to mental health
risks and underlying Status
comorbidity Income
Initiation – Diagnoses
& Employment
Treatment response Social position
Arpa S. EMCDDA 2017. Available at:
https://www.emcdda.europa.eu/system/files/attachments/6235/EuropeanResponsesGuide2017_BackgroundPaper-Women-
who-use-drugs.pdf [accessed Sep 2020]Heritability Estimates – genetische Belastung
Agrawal & Linskey, 2008
Additive genetics alcohol dependence 50-70%
nicotine dependence 50-75%
cannabis dependence 35-75%
cocaine dependence 35-80%
heroin dependence 40-60%Menschenrechtsverträge UN-Prinzipien
Kinderrechts- Internationale Konvention zum
Behindertenrechts-
konvention Schutz der Rechte aller
konvention (CRPD) Migranten und ihrer
(CRC) Familienangehörigen (CRMW)
Konvention zur
Internationales
Beseitigung jeder
Anti-Folter- Übereinkommen zur
Diskriminierung von
Konvention Beseitigung jeder Form von
Frauen (CEDAW)
(CAT) Rassendiskriminierung
(CERD)
Internationaler Pakt über wirtschaftliche, soziale und kulturelle
“Bill of Rechte (CESCR)
Rights” Internationaler Pakt über bürgerliche und politische Rechte
Allgemeine Erklärung der Menschenrechte
22 (UDHR)Pflicht des Einbezuges von Menschen mit
Behinderung: Art 4/3 CRPD
Bei der Ausarbeitung und Umsetzung von
Rechtsvorschriften und politischen Konzepten zur
Durchführung dieses Übereinkommens und bei
anderen Entscheidungsprozessen in Fragen, die
Menschen mit Behinderungen betreffen, führen die
Vertragsstaaten mit den Menschen mit Behinderungen,
einschließlich Kindern mit Behinderungen, über die sie
vertretenden Organisationen enge Konsultationen und
beziehen sie aktiv ein.
23Internationaler Pakt über wirtschaftliche,
soziale und kulturelle Rechte (CESCR)
Right to Health – Article 12 CESCR
1. Die Vertragsstaaten erkennen das Recht eines jeden auf das für ihn
erreichbare Höchstmaß an körperlicher und geistiger Gesundheit an.
Benefits of Scientific Progress – Article 15 CESCR
Die Vertragsstaaten erkennen das Recht eines jeden an (...)
b) an den Errungenschaften des wissenschaftlichen Fortschritts und seiner
Anwendung teilzuhaben; (z.B. : positive Diskriminierung –..... möglichst
früh & umfassend von neuen medizinischen Optionen profitieren).
24Definition von „SUCHT“
Substanzgebrauchsstörung
Ist eine chronisch psychiatrische Krankheit
Kontrollverlust – über die Einnahme einer Droge („Substanz“) oder ein
Verhalten, das trotz schädlicher/ negativer Auswirkungen weiter und
immer wieder ausgeführt wird.
Toleranz/Gewöhnung an bestimmte Dosis/Menge einer Substanz oder an
ein Verhalten- man braucht immer mehr für die gleiche Wirkung.
Entzugssymptome
Unterscheide:
Substanzgebundene Suchterkrankung, z.B. Alkoholabhängigkeit
Substanz-ungebundene Suchterkrankung, z.B. Glücksspiel
Sydney Cohen, 1985Ökonomischer Schaden der
unbehandelten Suchterkrankung
Die Kosten für die Suchtbehandlung in der EU* belaufen sich auf
€ 65.7 Milliarden - die fünft teuerste Erkrankung für die
Gesellschaft1
*In Purchasing Power Parity 2010
1. Wittchen H et al. Eur Neuropsychopharmacol. 2011;21:655–79;
2. Gustavsson A et al. Eur Neuropsychopharmacol. 2011;21:718–779.Jedes Ding ist ein Gift -
es kommt nur auf die Dosis an
Paracelsus 15. Jh.DIAGNOSE VON SUCHTERKRANKUNGEN: Klassifikationssysteme psychischer Störungen
Komorbidität
Substanz Kontroll-
• Psychiatrisch: gebrauchs gruppe
störung
Depression 36.3% 4.2%
Angststörung 16.3% 2.3%
ADHD 17.2% 3.0%
Psychiatrische Diagnose 55.5% 9.0%
Sterling S, Weisner C. Chemical dependency and psychiatric services for adolescents in private managed care: Implications for outcomes. Alcohol Clin Exper
Res. 2005;25(5):801-9.
* Alle pADHD
attention deficit/hyperactivity disorder
Prävalenz bei Kindern weltweit 8-12%:
Burschen 3 mal häufiger als Mädchen betroffen
• unaufmerksamer Typ
• hyperaktiver/impulsiver Typ
• kombinierter Typ
Biederman J, Faraone SV. Attention-deficit hyperactivity disorder. Lancet 2005;366:237-48.
Biederman J, Mick E, Faraone SV, Braaten E, Doyle A, Spencer T, Wilens TE, Frazier E, Johnson MA. Influence of gender
on attention deficit hyperactivity disorder in children referred to a psychiatric clinic. Am J Psychiatry.
2002;159:36-42.Psychiatric comorbidities of ADHD in adults
ADHD only
Anxiety disorders Substance Use
5-10% disorders
50% 50%
Conduct disorder Major depressive
disorder
80%
20% ADHD 35%
Bipolar 10% 10% Antisocial
disorder personality disorder
5% 5%
3% Postnatal
Depression
Borderline
personality disorder
Tourette-Syndrome
The MTA Cooperative Group, Archives of Specific learning
General Psychiatry 1999; 56:1073-1086. disabilities
Grafik: Prof. Dr. Martin LambertAngststörungen:
Geschlechtsunterschiede
16
14
12
10
Male
8
Female
6
4
2
0
PD SAD OCD SP PTSDPrevalence of psychiatric symptoms in
pregnant opioid-dependent
n=174; mean gestational age (weeks): 17
Symptoms at some point %
Psychiatric symptoms % in the past 30 days
One or more psychiatric Mood symptoms 49
65
diagnosis Anxiety symptoms 40
Major depression (MDD) 32 Suicial thinking 13
Dysthymia 31
Hypomanic episode 39
Anxiety disorders
- Generalized anxiety disorder (GAD) 40
- Panic disorder 26
- Agoraphobia 22
Social phobia 16
Post-traumatic stress disorder (PTSD) 16
Obsessive–compulsive disorder (OCD) 3
BulimiaSteuerung des Alkoholkonsum
für die globale Gesundheit
“Regulate alcohol for global health”
Devi Sridhar (2012) Regulate alcohol for global health. Nature, 482Alkohol: Epidemiologie
16
14
12
10
8
6
4
2
0
R N F L E L D L E L K K L E T T P S L A T X
ID
N
IN
D
TU
R
IS ZA EX R IT
A
BR
A IS JP
N
CA
N RC CH US
A
NL EC
D
NZ FI
N
CH PO BR AU
S
DN SV
N
SV BE CZ ES PR ES
N
RU DE
U IR FR
R
AU LU
CH M NO SW G O G HU KO
OECD Factbook 2013: Economic, Environmental and Social Statistics - © OECD 2012 / Alcohol consumption among
population age 15 and over
Litres per capita, 2010 or latest available yearAlkohol: Gesundheitsrisiko
Männer Frauen Risiko
Bis 40g / Tag Bis 20g / Tag gering
= 500 ml
= 20 g reiner Alkohol
40-60g / Tag 20-40g / Tag mittel
= 200 ml
= 20 g reiner Alkohol 60-100g/ Tag 40-60g / Tag hoch
Über 100g / Über 60g /
Tag Tag
sehr hochMortalität durch Alkoholkonsum & Abhängigkeit
% der Gesamtmortalität durch Alkoholkonsum,-
& Abhängigkeit in der EU (15-64 Jahre)
*
* Net burden: Schädliche Effekte - „beneficial effects“ („pos. Effekte“ des moderaten
Trinkens auf Diabetes & ischaemische Erkrankungen)
Rehm, J., et al. (2012). Toronto: Centre for Addiction and Mental Health.Psychiatrische Komorbidität
& Alkoholerkrankung
Schizophrenie - - ♂
47% Lebenszeitprävalenz von Suchterkrankung
34% Alkohol
28% andere Substanzen
Affektive Störungen --♀
32% Lebenszeitprävalenz von Alkoholerkrankung
Bipolar 56%
Depression 27%
Dysthymie 31%
Angststörungen --♀
15% Lebenszeitprävalenz von Alkoholerkrankung
GAS 21%
PTSD 18%
Soziale Phobie 17%
Regier DA et al. JAMA 1990; 264:2511.Alkohol
Prävalenz bei Adoleszenten
Young SE, Corley RP, Stallings MC, Rhee SH, Crowley TJ, Hewitt JK. Substance use, abuse and
dependence in adolescence: prevalence, symptom profiles and correlates. Drug Alcohol Depend.
2002;68:309-22.“Food Addiction”
Bestimmte Nahrungsmittel weisen ein gewisses Suchtpotential auf und bestimmte
Formen des Überessens („over-eating“) sind dem Suchtverhalten bei
Substanzgebrauchsstörung ähnlich sind.
Das Essen dieser Nahrungsmittel (meist stark zuckerhaltige oder kohlenhydratreiche
bzw. fette Nahrungsmittel) erfüllt in diesem Sinne nicht nur den Zweck der
Energiegewinnung, sondern wird eingesetzt als:
- Belohnung oder
- um negative Affektzustände auszugleichen
BMI < 18,5 – Untergewicht
BMI 18,5 – 24,9 - Normalgewicht
BMI 25,0 – 29,9 - Übergewicht
BMI ≥ 30 - Adipositas
-------------------------------------------------------------------------------------------------------------
Meule et al. (2017). German version of the Yale Food Addiction Scale 2.0.: Prevalence and correlates of “food addiction” in
students and obese individuals. Appetite, 115: 54-61.
Erstes standardisiertes Instrument zur Messung der „Food Addiction“: Yale Food Addiction Scale (YFAS; Gearhardt, Corbin, &
Brownell, 2009)
- Basiert auf den Diagnosekriterien der Substanzabhängigkeit nach DSM-IV
- Aktuell in einer überarbeiteten Form erhältlich: YFAS 2.0. (Gearhardt, Corbin, & Brownell, 2016)-
E,ntronrel
FoodAddiction?
B Brain Structures and Addiction
Mark S. Gold, MD, Noni A. Graharn, MPH, James A. Cocores, MD, and Sara Jo Nixon, PhD
Kcy Words: eatirg, food addiction, overweight, obesity, doparnine
(J Addict Med 2009;3: 4245)
f)ublic and professional acceptancethat use of drugs and alcohol could lead to physical
I and psychiatric disease states, that is, substance use disorders, required enonnous
clinical and research efforts. Now, sonre feel that this hard eamed stafus is threatenedby
discussions suggesting that gambling, sex, and food may result in similar outcomes.r.2
However, the mamcr by ivhich rcscarch was used to establishthe addicting characteristics
of dnrgs and alcohol must be the gold standard against which furlher considelations are
r.nadc.In terms of the qrrcstion of gambling, much of this rvork has been acconrplished
u ' i t h s t u d i e sd e r n o n s t l a t i n ss t r i k i n g s i m i l a l i t i e s b e t r v c e ng a u r b l i n g a n d e x o s e n o u sa d d i c -
t i o n s . I l v e n m o r e v a l u a b l e l c s s o n s h a v c b e e n l e a r n e d r c g a r d i n g t h e p r o c e s s i n go f o d d s ,
a s s c s s i n gr i s k , a n d d e c i s i o n - r n a k i n gd e f i c i t s e v i d e n c c d i n b o t h b c h a v i o r a l a n d n e u r o i n r -
aging studies of compulsive ganrblers and patients ,uvithsubstanceuse disordcrs.3
T'hrough all of the debate and as a result of systemic study, we have leamed that
a d d i c t i o ni s a n a c q u i r c d ,c h r - o n i cr el a p s i n gd i s o r d e rt h a t b e g i n s w i t h s o m e e x p c r i u r e n t a t i o n
a n d p l e a s u r a b l cr c s l ' l o n s e sa. u d t b r s u b g r . o u p o s l ' i n d i r " i d u a l si s f b l l o r v e db y p r e o c c u p r t i o n ,
r s c l l r t i , ) n . t o l c r a t t c c t- l c n i u l .e s c t ' i c so f r l c t l i c l t l . p s y ' c h o l o u i ca. n d s o c i a l c L r n s e ( l u c l r c c s
that lclate dircctly tcr tlie continued usr'. and what has lrcen referred to as a "fätal
attractiou" betr.vccnthe substancc (or activity, eg, garlblin-o) and the patient.
O b v i o u s l y , t b c p r o c e s sr c s u l t i n g i n a d d i c t i o n i s n o t f u l f i l l c d i n a l l o r c v c n m o s t u s c r s .
Thcre are a nulnber ofhost or individual firctors, such as genetics, intrauterinc exposurc,
c a r l y c h i l d h o o d , a n d a d o l e s c e n c ee x p e d e n c e ,w h i c h i n f l u e n c c s u s c e p t i b i l i t ya n d / o r r e s i l -
ience. Fulthcnnore, phamracological factors such as route of adrninistration are also
irnporlant. To desci'ibe coca leaf cher.ving as cocaine taking docs little to capture the
intensity ofcoca paste or cocaine tieebase or crack smoking. Technologic invcntions havc
a l s o b e e r . ra p p l i c d t o d l u g s o f a b u s c m a k i n g t h e m m o l e r c i n f o r c i n g , c o m p e l l i n g , a n d
addicting. Finally, the same drug can be used by thc same pelson but the experience is
different. For exanrple, nicotine when administcred through cigarettes or smokeless
tobacco is highly addicting. Yet, nicotine patches and gum are so unappealing that many
State programs give them away.
Drugs of abuse or gambling are not, however, a part of everyday life and survival.
Food and sex are and therefore pose particularly difficult questions for clinicians and
rcsearchers including what separates periodic excessive intake (ie, during periods of
vacation or spccial holidays) from abnormal or pathologic intake, and to what extent must
life activities be compromised to meet diagnostic critcria. Fundamentally. we rnust ask if
we cau apply standartls used in clcfirring neurobehavioral changes associated rvith
l c c o g n i z e da d d i c t i o n st o t h e i s s u c so f l b o d a n d s c x , a s w e l l . I f w e c a n , d o , ' v e l i a v e a c h o i c e
to recognize thc potentially addicting capacities of food and sex?
For these "survival-related" addictions, the degree ofaccess and availability may be
essential in creating the opportunity for addiction. For sex, "high-speed," rather than
slower "dial-up," universally accessiblepomclgraphy has provided world-wide accessand
f'rom the l)cpartrncllts of Psychiatry, Ncutoscience, Ancsthesioloey, Cornmunity l{ealth and Fanrily Medicine, Universiry of Flonda College of Medicirre
Gaincsville, FI-.
Copyrighl !:r 1009 Arncrican Society of Addiction Mcdicine
iSSN: l92i 0629t0910301-0012
a> t e d . V o l u m e3 , N u m b e r1 , M a r c h2 0 0 9
I A d d i cM
As tlte Americart Psychiatt'icAssociatiott comrnittees begin fortrnl work ort DSM-V u,e welcorne
brief editorials orzissuesthat should be considered irt its formulation.
lssuesfor DSM-V:Should Obesity Be Included
as a Brain Disorder?
besity (body mass index >30), has increasedsignificantly over the past 30 years
(approximately 50% per decade) (l), afflicting 32.27oof adults in the United States(2).
OFC
Obesity increasesrisk for cardiovasculardisease,diabetes,cancer,and other diseases,
resulting in annual health care costs conservativelyestimated for the United Statesat
$70 to $100 billion a year (3) as well as reductions in life expectancyby 5 to 20 vears (4).
These facts highlight the urgent need to develop strategiesto prevent and treat those
afflicted.
Although there have been major scientific advancesin the treatment of the medical
complications of obesity (i.e.,diabetes,hypertension hvpercholesterolemia),the mor-
bidity from this disorder is hampered by the fail-
ure of interventions to sustainweight loss.Stan-
"i'"lsrm.s irlrirrI lf*ru of'rllri dard interventions based on promoting lifestyle
t n e:w{n{ {{}t tl,fiün t,trt {iJ. changesto decreaseexcessivefood consumption
(dieting) and increased physical activity (exer-
o{;rtstil.' s/rs:r,sJrdd.:sr:rlcs}r cise)are effectiveand can normalizeweight if fol-
frlr3{i"tln lir*l lrr:u.ft;st:ttl*J lowed rigorouslv,but unfortunately they are in-
r:fuer"st f-tr'to "/iarillfrclei credibly difficult to sustain. The discrepancy
between the successesof the metabolic treat-
mtp f fr*II r,v* l rr',1
x;r.r ments of consequencesof obesity and the fail-
"
tn t'rci,nsiz*' r'*tJ*i:r.s*'. ures of behavioraltreatmentsto prevent or re-
verse obesity highlight the fact that this condition
is not onlv a metabolic disorder but also a brain
disorder.Considerationof the mental component of obesityshould be a key target in the
treatment of obesity to facilitate compliance and minimize relapse.Here, rve propose
that some forms of obesity are driven by an excessivemotivational drive for lbod and
should be included as a mental disorder in DSM-V
DSM-IV recognizeseating disorderssuch as anorexiaand bulimia as mental disorders
with severeimpairments and seriousadverseoutcomes but does not recognizeobesity
despite its devastatingmedical and psychologicalconsequences.Obesity is character-
izedby compulsive consumption ol food and the inability to restrain from eating de-
spite the desire to do so. Thesesymptorns are remarkablyparallel to those described in
DSM-IV for substanceabuse and drug dependence(Tablel), which has led some to
suggestthat obesity may be considereda "food addiction" (5).
There are multiple mechanismscontributing to the r,ulnerabilityto obesity,including
genetic, developmental,and environmental factors that are likely to interact in diverse
ways among individuals to produce the behavioral phenotype of overeating (6). The
"thrifty genotlpe" hypothesis suggeststhat evolution shaped the circuits involved in
how our bodies store food as well as the circuits involved in the procurement of food in
our ancestorswhen food was scarce.In current environments,where for the nrost part
food is widely availableand diverse,these circuits can lead to food overconsumption.
The "developmentalorigin hypothesis"suggeststhat calorie content aswell as exposure
to certain nutrients during pregnancy modifu horv the body and brain develop in anti-
cipation of future environments with similar nutrient characteristics.
\A4ratbrain circuits are associatedwith obesity?The hypothalamus is recognized as the
main brain region that controlsthe regulatorysignalsfor food consumption.The genetic
704 aj p.psych iatryo n Ii ne.o rg Am J Psychiatry 164:5. May 2OO7
NA : Nucleus Accumbens (Ventral Striatum); VTA : Ventral Tegmental Area; A : Amygdala;
C : Caudate Nucleus (Dorsal Striatum); PFC : Prefrontal Cortex; OFC: Orbitofrontal CortexSTIGMA
Adipositas/Übergewicht – Österreichische Daten
Gesundheitsbefragung 2014/Statistik Austria
Rund 3,4 Mio. ÖsterreicherInnen waren 2014 übergewich{g bzw. adipös. Bei Männern trat
Übergewicht häufiger auf als bei Frauen (39 % bzw. 26 %).
Bei Adipositas waren die Geschlechtsunterschiede geringer (Männer: 16 %, Frauen: 13 %).Childhood Obesity Surveillance Initiative
(COSI) der WHO
• Erfassung von 2510 Drittklässlern in Österreich
• Ca. 30% der Buben in der dritten Schulstufe sind
übergewichtig oder adipös
• Bei den Mädchen reicht die Rate von 21% - 29%
(Ost-West Gefälle)
• Einfluss auf das Gewicht haben z.B.
Verfügbarkeit von Obst in der Schule,
Verfügbarkeit eines Turnsaales & das
Lebensumfeld (in urbanen Gegenden häufiger
Übergewicht)
• Übergewichtige/adipöse Kinder haben ein
erhöhtes Risiko übergewichtige Erwachsene zu
werden!
(Schuljahr 2014)Übergewicht und seine somat. Folgen
• Risikofaktor Adipositas (BMI >30)
Koronare Herzkrankheiten
Diabetes Mellitus Typ II
Arteriosklerose
Hypertonie
Gallenleiden
Malignome
Gicht
• Mehrkosten durch Medikamente
(167 Mill. Euro/Jahr)…..this is how it started
…..and this is how it ended
Globale Rauchprävalenz: 1980-2012
Prävalenzraten täglicher Raucher 1980 und 2012 in ausgewählten Regionen/Ländern
Land Total Männer Frauen
1980 2012 1980 2012 1980 2012
Global 26% 19% 41% 31% 11% 6%
Europa 32% 27% 41% 34% 24% 22%
Spanien 36% 26% 45% 29% 29% 23%
Portugal 22% 23% 37% 32% 9% 16%
Deutschland 33% 24% 39% 28% 28% 22%
Frankreich 29% 31% 41% 34% 19% 28%
Italien 33% 24% 43% 28% 23% 21%
Griechenland 39% 38% 54% 41% 25% 35%
Polen 42% 27% 57% 32% 29% 24%
49
Österreich 28% 32% 34% 37% 22% 29%
Ng, M., et al., (2014). JAMA, 311(2), 183-192.New clip here
The great gender equalizer
Rauchen und Inzidenz des
Brustkrebses
Prospektive Kohortenstudie:
• 111.140 aktive Raucherinnen 1976-2006
• 36.017 passive Raucherinnen 1982-2006
Ergebnisse:
• Inzidenz der Burstkrebserkrankungen stand im sign. Zusammenhang mit:
– starkem Zigarettenkonsum in der Gegenwart p=0,02
– starkem Zigarettenkonsum in der Vergangenheit p=0,003
– längere Dauer des Rauchens p=0,01
– mehr Packungsjahre* p=0,005
Passives Rauchen in der Kindheit und im Erwachsenenalter ergab keinen Zusammenhang
mit dem Brustkrebs
*Packungsjahre=Zahl der Zigarettenpackungen/d x Zahl der Raucherjahre
Xue et al. (2011). Cigarette smoking and the incidence of breast cancer. Arch. Intern. Med.171(2):125-33.Alkoholkonsum und
Brustkrebsrisiko
Kohortenstudie in Schweden:
• Beobachtungszeitraum 1965 – 1995
• 36.856 Frauen mit Diagnose Alkoholabhängigkeit
mindestens ein Jahr vor der Diagnose Brustkrebs
• Durchschnittsalter 42,7 Jahre
• Durchschnittsdauer von Follow-up 9,6 Jahre
• 6,5% Frauen mit Diagnose Leberzirrhose
• 5,4% Frauen mit Diagnose Diabetes Mellitus
Kuper et al. (2000). Alcohol and breast cancer risk: the alcoholism paradox. British Journal of
Cancer, 83 (7):949-951.Alkoholkonsum und
Brustkrebsrisiko
Ergebnisse:
• Das Brustkrebsrisiko bei Frauen mit vorangegangener Diagnose
Alkoholabhängigkeit ist um 15% höher als altersstand.
Durchschnittsrisiko für Frauen in Schweden.
• Alkoholkonsum und Erhöhung des Östrogenlevels können das
Brustkrebsrisiko wesentlich beeinflussen.
• Das Brustkrebsrisko erhöht sich aber nicht proportional zum
Ethanolkonsum: Brustkrebsrisiko im Vergleich zwischen sehr
hohem (>60g Ethanol/d) und hohem (~50g/ Ethanol/d)
Alkoholkonsum erhöht sich nicht mehr, es scheint → ein Plateau
wird erreicht.
Kuper et al. (2000). Alcohol and breast cancer risk: the alcoholism paradox. British Journal of
Cancer, 83 (7):949-951.Adipositas und Brustkrebs • Methodik: • Daten von 73.542 prämenopausalen Frauen und 103.344 postmenopausalen Frauen aus 9 EU-Ländern teilnehmend an der EPIC-Studie (European Prospective Investigation into Cancer and Nutrition) • In 4,7 Jahren von Follow-up wurde bei 1.879 Frauen Brustkrebs diagnostiziert. • Frauen mit BMI >30 hatten um 31% erhöhtes Risiko, einen Brustkrebs zu bekommen im Vergleich zu Frauen mit BMI
Prostata & Psyche • Prostatakrebs 4.500 Fälle pro Jahr in Österreich (25% aller Tumoren bei Männern) • 5-Jahres-Überlebensrate 47% Zielonke A. (2010). Krebsinzidenz und Krebsmortalität in Österreich. Statistik Austria
Assoziation zwischen Rauchen & Prostatakrebs
Ziel der Studie: Untersuchung der Assoziation zwischen
– Rauchstatus vor der Behandlung
– kumulativer Rauch-Exposition
– vergangener Zeit seit dem Aufhören
und dem biochemischen Wiederauftreten (biochemical recurrence, BCR) von
Prostatakrebs in Patienten die mit radikaler Prostatektomie behandelt
wurden.
Methodik: Retrospektive Analyse von N = 6.538 Patienten, behandelt mit
radikaler Prostatektomie
– Mittleres Alter: 61 Jahre
– Klinisch-pathologische und Rauch Variablen (Rauchstatus, Anzahl tägl. Gerauchter
Zigaretten, Rauchdauer, vergangene Zeit seit dem Aufhören)
Rieken, M., et al. (2015). European urology.Biochemisches Nicht-Wiederauftreten (survival curve) nach Rauchstatus
Blasenkrebs
• >350.000 Personen werden pro Jahr neu mit Blasenkrebs
diagnostiziert
• Rauchen ist der best-etablierte Risikofaktor für ♀ & ♂
gleichermaßen
• Risiko (Odds Ratio) von gegenwärtigen RaucherInnen (vs. Nicht-
RaucherInnen) Blasenkrebs zu entwickeln ist von 1994 bis 2004 von
2,9 auf 4,2 gestiegen
• Zusammensetzung von Zigaretten hat sich in den letzten 50 Jahren
verändert
– Reduktion von Teer & Nikotin
– Aber höhere Konzentration spezifischer Karzinogene (z.B. β-
napthylamine, ein bekanntes Blasen-Karzinogen)
Freedman, et al. (2011). Association between smoking and risk of bladder cancer among men and women. JAMA, 306(7), 737-745.Assoziation zwischen Rauchen & Blasenkrebs ♂ (N=281.394) und ♀ (N=186.134) der National Institutes of Health-AARP (NIH- AARP) Diet and Health Study Kohorte (US) HR = Hazard Ratio (Risiko an Blasenkrebs zu erkranken, abh. vom Rauchstatus) à Rauchen erhöht das Risiko für Blasenkrebs gleichermaßen für ♀ & ♂ Freedman, N. D., et al. (2011). JAMA, 306(7), 737-745.
Ziel der Studie • Komparative Prävalenz sowie determinierende Faktoren für Substanzkonsum unter österreichischen Studierenden • Unterschiede in der Prävalenz anhand der Determinanten Region (Land vs. Stadt) und Geschlecht zu untersuchen.
Substanzkonsummuster bei Öster. Studierenden
Monatlicher Substanzkonsum
Total Wien Innsbruck
(N=1,893) (N = 907) (N = 829)
Männer Frauen Männer Frauen
(N = 353) (N = 554) (N = 282) (N = 547)
638 90 243 67 238
Alkohol
(33,7%) (25.5%) (43.9%) (23.8%) (43.5%)
190 58 76 23 33
Tabak
(10.0%) (16.4%) (13.7%) (8,2%) (6,0%)
257 73 87 46 51
Cannabis
(23.6%) (20.7%) (15,7%) (16,3%) (9,3%)
84 11 44 10 19
Benzo.
(4,4%) (3,1%) (7,9%) (3,5%) (3,4%)
593 72 272 53 196
Analgetika
(31,3%) (21,5%) (49,0%) (18,7%) (35,8%)
Unger, A., et al. (2014). Suchttherapie, 16: 27-35.Importance of sex issues in substance abuse research Thibaut F. Psychiatric Times. 2018(November):p17–18
Prevalence of illicit drug use:
Differences between and
• In the EU, 34.8 million aged 15 to 64 were reported to have previously
tried an illicit drug, compared with 54.3 million 1
Key:
Illicit highest
drug use: lifetime prevalence in the general population2
rates
lowest
rates
Adapted from EMCDDA2
1. EMCDDA (European Monitoring Centre for Drugs and Drug Addiction) (2016a). European drug report
2016: trends and developments. Publications Office of the European Union, Luxembourg. 2. EMCDDA
(European Monitoring Centre for Drugs and Drug Addiction) (2016b). Statistical bulletin 2016 (data
tables). Available at: http://www.emcdda.europa.eu/data/stats2016 [accessed Feb 2020]Geschlechtsspezifische Unterschiede
Adoleszente
• Percentages of past
year dependence on or
abuse of alcohol or any
illicit drug among
persons aged 12 or
older, by gender: 2003
Ø Males-to-females ratios
of prevalence are
narrowing
National Survey on Drug Use and Health. Gender differences in substance dependence and abuse. SAMHSA 2005Differences between and who use
drugs
The risk of
Substance use acquiring
begins at an certain somatic use different types
earlier age in comorbid of drugs
conditions is compared with
higher in
than in
1 (e.g.
(e.g. HIV)2 amphetamine)3
may be at
have a more
greater risk of
rapid
health and well-
progression to
being issues
dependence and
(e.g. through
organ damage1
prostitution,
violence)1,2
1. Unger A, et al. J Addict Dis. 2010;29(2):217–30. 2. El-Bassel N, et al. J Acquir Immune Defic Syndr. 2015;69:S182–90. 3.
SAMHSA. The TEDS Report: Gender Differences in Primary Substance of Abuse across Age Groups. 2014 Rockville, MD.
Available at: https://www.samhsa.gov/data/sites/default/files/sr077-gender-differences-2014.pdfThe importance of gender issues in
substance abuse research
• Historically, participants in substance abuse research were
largely
• Predictors and progression of SUD are gender-
specific/sensitive
• Comorbidities differ significantly
• Number of with substance use disorder is increasing
Ø Important implications for development of diagnostic and
treatment interventions
Tuchman E. J Addict Diseases. 2010:29(2);127–38Medikations - Optionen
methadone
buprenorphine
buprenorphine +
naloxone naltrexone
SROM
Sc Buprenorphine
depot diacethylmorphine
naloxone - spray
Sc Buprenorphine depotPhysiological considerations for using opioid maintenance
treatment
In comparison to , may have :
A lower body 1.5–2 times A higher risk for Higher Hormonal-
weight and higher CYP3A4 long QT-dependent glomerular specific
higher fat expression1 cardiac arrhythmias filtration rates1 factors:2
percentage1 during methadone Contraception
maintenance Menstrual cycle
treatment1 Pregnancy
Menopause3
Why is this important?
Understanding of physiological differences between and can provide a better understanding of pharmacological
differences of OMT, opioid use and allow for gender-tailored therapy
1. Graziani M, Nisticò R. Frontiers in Pharmacology. 2015;6(122). 2. Unger A, et al. J Addict Dis. 2010;29(2):217–30. 3. Tuchman E. Soc Work Health Care. 2007;45:43–62Current rates of entering treatment1
According to the European Drug
In 2017, ~662,000 of people Report (2019),
who use opioids in the EU (and were entering treatment for
Norway), received opioid 30
26
Percentage of women entering
substitution therapy (OMT)1 25
20
20 17
treatment (%)
15
15
10
5
0
25% of those who bi
s
ne e t…
oi
n
n a ai ph e r
received OST were C
an C
oc A
m H
1. EMCDDA. European Drug Report 2019. Available at:
http://www.emcdda.europa.eu/system/files/publications/11364/20191724_TDAT19001ENN
_PDF.pdf [accessed Feb 2020]Psychosocial considerations and barriers
to OMT for 1
Stigma
Discrimination
Few -only services
Lack of adequate care in prisons
More likely to experience sexual and physical
abuse than non-drug using
Childcare responsibilities
Difficulty in becoming financially independent
High unemployment rates
1. El-Bassel N, Stathdee SA. J Acquir Immune Defic Syndr. 2015;69:S182–90Psychiatric comorbidity and OMT • If possible, diagnose and treat after proper stabilisation • Medications are likely to be almost as effective as in non- addicted patients • Generally, successful treatment of comorbid disorder has positive effects on substance abuse • Integrated double (or triple) treatments are neccessary to address substance use disorder and comorbidity successfully
Considerations for pregnant using
OMT
OMT in pregnant has been shown to improve Important things to keep in mind when
pregnancy outcomes by:1 managing pregnant with OMT:
• Reducing withdrawal episodes • Both methadone and buprenorphine can be
• Reducing high-risk drug-seeking behaviours prescribed during pregnancy2
• Improving compliance with prenatal care
• The pharmacokinetics of methadone in
pregnant differs from non-pregnant and
significantly changes throughout pregnancy1
Neonate-related considerations1
• Many experience vomiting during pregnancy
In utero exposure to opioids is associated
which can affect the amount of methadone absorbed2
with a 60–80% appearance of neonatal
abstinence syndrome (NAS); therefore,
• Buprenorphine/naloxone combination products
close monitoring of this condition is
recommended are not recommended for pregnant 2 as
NAS is characterised by CNS hyperirritability, pre-clinical data suggest that naloxone may lead to
autonomic nervous system dysfunction, and maternal and foetal hormonal changes3
gastrointestinal disturbances
1. Stover MW, Davis JM. Semin Perinatol. 2015;39(7):561–65. 2. Arunogiri S,
et al. Aust. Fam. 2013;42(10):713–16. 3. Unger A, et al. J Addict Dis.
2010;29(2):217–30How can HCPs support opioid-dependent
pregnant who decide to take OMT?1
• Diagnose substance use disorder and psychiatric and somatic comorbidity
• Carefully titrate OMT to manage opioid cravings and physiological withdrawal
• If the client is maintained on an opioid combination product, transfer them onto the
mono-buprenorphine2
• Consider dose increments as the pregnancy progresses (particularly in the third trimester) –
titrate the dose of OMT after delivery
• Counsel the client on the risk of their baby developing NAS
• Closely monitor the client for psychosocial stressors and mental state
• Communicate effectively with the obstetrics team, particularly during the peri-partum and post-
partum period to effectively manage the client’s pain during delivery
• Regularly monitor the neonate for NAS and liaison with services
1. Arunogiri S, et al. Aust Fam. 2013;42(10):713–16. 2. Unger A, et al.
J Addict Dis. 2010;29(2):217–30Physiological considerations for
menopausal using OMT1
• There are limited data encompassing
drug use, menopause and health
Opioid
Menopause Withdrawal • Despite this, symptoms associated with
Sweats menopause are similar to symptoms
Insomnia Drug craving reported in opioid withdrawal
Hot flashes
Anxiety
Depression Vomiting • In a study exploring the prevalence
Menstrual-
irregularities Poor concentration of menopause symptoms in methadone-
Decreased libido Diarrhoea
maintained aged 40–55 (N=135),
Vaginal dryness Fatigue
Weight gain Shaking the most common symptoms were
Achy joints insomnia (62.2%), depression (64.4%),
irritability (68.9%) and hot flashes
(58.5%)
1. Tuchman E. Soc Work Health Care. 2007;45:43–62Abused prescription opioids
Fentanyl
Tramadol Hydromorphone
Codeine
Aspirin and
Oxycodone
OxycodoneFalco
Whitney Houston
Amy Winehouse
Michael JacksonIllicit drug use (including alcohol) is
increasing among older people
Older People with Drug Problems (OPDP) in Scotland: population estimates/projections (both sexes,
2009/10 – 2027/28)*
Scottish Drug Forum Older People with Drug Problems in Scotland: Addressing the needs of an ageing population Available at: http://www.sdf.org.uk/wp-
content/uploads/2017/06/Working-group-report-OPDPs-in-2017.pdf [Accessed Sept 2020]Missbrauch verschreibungspflichtiger
Medikation bei Menschen >50
• 25% der verschreibungspflichtigen Medikamente
werden Patienten > 50 verschrieben
Indikationen:
• Chronischer Schmerz
• Schlaflosigkeit
• Spannungszustände
11% der Frauen > 50: Missbrauch von
verschreibungspflichtigen Medikamenten
Cluberson & Ziska, Geriatrics 63(9):22-26, 2008
Simoni-Wastila, Am. J. Geriatr. Pharmacother. 4(4): 380-394, 2006Beeinflussende Faktoren - PatientInnen
Folgende PatientInnen-Faktoren sind signifikant mit
einer erhöhten Verschreibung von „Beruhigungsmittel“ assoziiiert:
• höheres Alter
• weibliches Geschlecht
• Arbeitslosigkeit
• Verlust des Partners
• psychische Erkrankung
Kisely et al. (2000). Why are patients prescribed psychotropic drugs by general practitioners? Results of an international study. Psychological
Medicine (30):1217-25.Beeinflussende Faktoren –
verschreibende ÄrztInnen
Erläuterung der Ergebnisse:
Folgende Faktoren sind signifikant mit einer erhöhten
Verschreibung von Psychotropika assoziiert:
• weibliches Geschlecht des verschreibenden Allgemeinmediziner
Folgende Faktoren vermindern die Verschreibung von Psychotropika
um bis zu 50 %:
• Subjektiv empfundene Relevanz einer postgraduellen Ausbildung
(Fachbereich Psychiatrie) der verschreibenden ÄrztIn
• Tatsächlich absolvierte postgraduelle Ausbildung
Kisely et al. (2000). Why are patients prescribed psychotropic drugs by general practitioners? Results of an international study. Psychological
Medicine (30):1217-25.Drogenscreening
bei verletzten Unfallopfern
(Quelle: Österreichische Gesellschaft für Unfallchirurgie, 2007)Prevalence rates of in prison
Between 1980 and 2017, the number of incarcerated in the USA rose
by > 750%1
• increased from ~26,400 in 1980 to ~225,000 in 2017
• the rate of growth of imprisonment was twice as high as that for
Systematic review (13 studies/7563 prisoners) demonstrated prevalence of2
• alcohol abuse and dependence: 18–30% 10–24%
• drug abuse and dependence: 10–48% 30–60%
Ø Necessity for screening at entry in prison, treatment in custody, follow-up on release; specialized gender-specific service2
1. The sentencing project. Incarcerated women and girls. Available at:
https://www.sentencingproject.org/publications/incarcerated-women-and-girls/ [accessed
Sep 2020]. 2. Fazel S, et al. Addiction. 2006;101(2):181–91Early warning systeme in the EU for NPS:
2018 around 600
Assessment Scientific board, EMCDDANew psychoactive Substances (NPS)
Geschlechts- und Alterseinflüsse bei pathologischen
SpielerInnen in Behandlung (1)
Variable Junge Erwachsene Mittleres Alter Ältere
18-35 J. 36-55 J. >55 J.
n=97 (22,7% ♀) n=197 (44,2% ♀) n=49 (55,1%♀)
Alter bei Mittelwert Mittelwert Mittelwert
Spielbeginn***
Männer 17,0 17,5 21,2
Frauen 21,3 30,4 41,7
Alter bei Beginn des
regelmäßigen
Spielens***
Männer 21,0 27,5 33,2
Frauen 25,5 39,1 54,8
Jahre des
Problemspielens**
Männer 5,8 12,4 16,0
Frauen 4,6 5,1 5,6
*** pGeschlechts- und Alterseinflüsse bei pathologischen
SpielerInnen in Behandlung (2)
Variable Junge Erwachsene Mittleres Alter Ältere
18-35 J. 36-55 J. >55 J.
n=97 (22,7% ♀) n=197 (44,2% ♀) n=49 (55,1%♀)
Spieleinsätze im Means Means Means
letzten Monat*
Männer $ 1.000 $ 1.000 $ 1.500
Frauen $ 800 $ 1.000 $ 1.800
Spieleinsätze als %
des monatl. % % %
Einkommens*
Männer 94 67 187
Frauen 125 77 249
Spielschulden
Männer $4.000 $6.000 $25.000
Frauen $3.250 $5.000 $12.000
* pKey note der Literatin Chimamanda Ngozi Adichie bei
der Chatham House Konferenz in London,
UK – Juni 2018
“In our world,
a man is confident, but a women is arrogant.
A man is uncompromising, but a women is a ball-breaker.
A man is assertive, a women is aggressive.
A man is strategic, a women is manipulative.
A man is a leader, a women is controlling.
A man is authoritative, a women is annoying.
The characteristic of behavior is the same, what is
different is the sex. And based on the sex, the world makes
assumptions and treats us differently (...)”
https://ChathamHouse/Stereotyp- Mann/Frau I
• Ein Familienfoto steht auf seinem Schreibtisch:
Er ist ein solider, treusorgender Mann.
Ein Familienfoto seht auf ihrem Schreibtisch:
Ihre Familie kommt vor dem Beruf
• Sein Schreibtisch ist überladen: Er ist belastbar und fleißig
Ihr Schreibtisch ist überladen: Sie ist unordentlich und
zerfahren.
• Er spricht mit Kollegen: Er wälzt geschäftliche Probleme.
Sie spricht mit Kolleginnen: Sie klatscht.
• Er ist nicht am Schreibtisch: Er wird in der Konferenz sein.
Sie ist nicht am Schreibtisch: Sie wird auf der Toilette sein.Stereotyp: Mann/Frau II
• Er ist nicht im Büro: Er trifft sich mit Kunden.
Sie ist nicht im Büro: Sie ist einkaufen
• Er ist mit dem Chef zum Essen: Er macht Karriere
Sie ist mit dem Chef zum Essen: Sie hat was mit ihm
• Er heiratet: Das gibt ihm Beständigkeit
Sie heiratet: Dann kommt ein Kind und sie geht
• Er kündigt und verbessert sich: Er weiß die Chance zu
nützen
Sie kündigt und verbessert sich: Sie ist unzuverlässig
Nach N.Josefowitz; Impression from an officeLIFE IS A RACE BETWEEN
EDUCATION AND DISASTER
H.G. Wells - 1904
Drugs of Abuse
Engage Systems in
the Motivation and
Pleasure Pathways
of the BrainSie können auch lesen