Pathogenetische Bedeutung der Verteilung von BRAF Mutationen bei Patienten mit Melanom
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Pathogenetische Bedeutung der Verteilung
von BRAF Mutationen bei Patienten mit
Melanom
Hautklinik des Universitätsklinikums Erlangen
der Medizinischen Fakultät
der Friedrich-Alexander-Universität
Erlangen-Nürnberg
zur
Erlangung des Doktorgrades Dr. med.
vorgelegt von
Mirjam Anna-Sofie BaiterAls Dissertation genehmigt von der
Medizinischen Fakultät der Friedrich-Alexander-Universität
Erlangen-Nürnberg
Vorsitzender des Promotionsorgans: Prof. Dr. Markus F. Neurath
Gutachter: Prof. Dr. Lucie Heinzerling
Gutachter: Prof. Dr. Bastian Schilling
Tag der mündlichen Prüfung: 12.05.2020Inhaltverzeichnis 1. Zusammenfassung / Abstract............................................................. 1 1.1 Hintergrund und Ziele / Background and Objectives ...............................1 1.2 Methoden / Methods...............................................................................1 1.3 Ergebnisse / Results .................................................................................2 1.4 Schlussfolgerungen / Conclusions ............................................................3 2. Einleitung / Introduction .................................................................... 4 3. Literaturverzeichnis / References .................................................... 16 4. Orginalpublikation / Original article................................................. 22 5. Bisherige Veröffentlichungen / Register of publications ................. 23
1. Zusammenfassung / Abstract
1.1 Hintergrund und Ziele / Background and Objectives
Das Onkogen BRAF ist bei 44 bis 48% der Melanompatienten mutiert (Eigentler
et al., 2016, Greaves et al., 2013, Long et al., 2011, Menzies et al., 2012). Die
Häufigkeit der Mutation ist mit dem Subtyp und dem Alter des Patienten
assoziiert (Menzies et al., 2012, Whiteman et al., 2011). Patienten deren
Melanom eine BRAF Mutation aufweist, können mit den B-Raf Inhibitoren
Vemurafenib und Dabrafenib (in Kombination mit MEK-Inhibitoren) wirksam
behandelt werden (Ascierto et al., 2016, Klein et al., 2013, Long et al., 2015,
Parakh et al., 2015). Die von der U.S. Food & Drug Administration zugelassenen
Mutationstests können jedoch lediglich die V600E und teilweise V600K Variante
verlässlich nachweisen (U.S. Food & Drug Administration, 2011b, U.S. Food &
Drug Administration, 2013c).
Diese Studie untersucht die Häufigkeitsverteilung der BRAF V600E und nicht-
V600E Mutationen bei den verschiedenen Melanomsubtypen. Dies hat hohe
klinische Relevanz für den Einsatz der Inhibitortherapie, da Patienten mit
seltenen Mutationen ebenfalls erfolgreich mit BRAF-Inhibitoren behandelt
werden können (Klein et al., 2013, Parakh et al., 2015). Darüber hinaus spielt es
für die Einteilung der Melanomsubtypen auf molekularer Ebene eine wichtige
Rolle und trägt zum Verständnis der Melanomgenese bei. Bei den MUPs
(Melanomas of Unknown Primary/Melanome mit unbekanntem Primarius)
könnte die Verteilung der BRAF Genotypen einen Hinweis auf den Ursprung des
Primarius liefern.
1.2 Methoden / Methods
Bei 179 Patienten mit metastasiertem Melanom wurden retrospektiv der
histologische Subtyp (noduläres, superfiziell spreitendes, akrolentiginöses und
mukosales Melanom, sowie andere1), die Primärtumorlokalisation
1 lentiginöses, nävoides, polypoides, spitzoides und desmoplatisches Melanom
1(‚Extremitäten‘, ‚Rumpf‘ und ‚Kopf und Nacken‘), sowie der BRAF Mutations-
status auf Codon 15 erhoben. Anschließend wurde der BRAF Genotyp mit 1) dem
histologischen Subtyp und 2) der Primärtumorlokalisation in Bezug gesetzt. Bei
den MUPs wurden ebenfalls die BRAF Mutationen bestimmt.
Zur Berechnung der Korrelationen wurde der exakte Test nach Fisher angewandt.
1.3 Ergebnisse / Results
In der untersuchten Kohorte lag bei 82 Tumoren (44.3%) eine BRAF Exon 15
Mutation vor. Von diesen trugen 66 (80.5%) eine BRAF V600E, 7 (8.5%) eine
BRAF V600K und 9 (11%) andere BRAF Mutationen (V600G, V600D, V600D
K601del, V600R, L597S, V600E (GAA), V600E K601del). Die BRAF Mutations-
häufigkeit war je nach histologischem Subtyp unterschiedlich. In der Gruppe der
superfiziell spreitenden Melanome lag in 27 Fällen (57.4%) eine BRAF Mutation
vor und war mit diesem Subtyp signifikant assoziiert (p = 0.042). Bei den
nodulären, akrolentiginösen und mukosalen Melanomen waren es jeweils 29
(54.7%), 4 (28.6%) und 3 (11.1%). Davon trugen in der Gruppe der superfiziell
spreitenden Melanome 8 (17%) und in der Gruppe der nodulären Melanome 5
(9.4%) eine nicht-V600E BRAF Mutation. Die Patienten mit mukosalem und
akrolentiginösem Melanom wiesen keine nicht-V600E Mutation auf. An den
‚Extremitäten‘ wiesen 17 von 33 Primärtumoren (51.5%) eine BRAF V600E und
keiner eine nicht-V600E Mutation auf. Die Assoziation von BRAF V600E und
‚Extremitäten‘ war statistisch signifikant (p = 0.012). Am ‚Rumpf‘ trugen 21 von
53 Tumoren (39.6%) BRAF V600E und 7 (13.2%) nicht-V600E Mutationen. An
‚Kopf und Nacken‘ waren jeweils 9 von 24 (37.5%) der Primärtumore BRAF V600E
und 6 (25%) nicht-V600E BRAF mutiert. Die MUPs ähnelten hinsichtlich ihres
BRAF Mutationsstatus den superfiziell spreitenden und nodulären Melanomen.
Sie grenzten sich in Bezug auf ihre BRAF Mutationshäufigkeit (44.8%) statistisch
signifikant von den mukosalen Melanomen (11%) ab (p = 0.01).
21.4 Schlussfolgerungen / Conclusions
Patienten mit akrolentiginösen und mukosalen Melanomen sollten wie die
nodulären und superfiziell spreitenden Melanome standardmäßig auf BRAF
Mutationen untersucht werden. Des Weiteren sollte ein BRAF-Mutationstest
verwendet werden, der die nicht-V600E BRAF Mutationen verlässlich detektiert,
da sonst seltene aber therapierelevante Mutationen nicht detektiert werden. Die
Unterschiede in der Häufigkeitsverteilung der BRAF Genotypen (Wildtyp, V600E
und nicht-V600E) je nach Primärtumorlokalisation und histologischem Subtyp
bekräftigen die aktuelle Einteilung der Melanome auf molekularer Ebene. MUPs
haben entsprechend ihrer molekularen Einordnung ihren Ursprung in superfiziell
spreitenden und nodulären Melanomen.
32. Einleitung / Introduction
BRAF ist ein Gen, welches die Kinase B-Raf kodiert. B-Raf ist Teil des zellulären
MAPK (mitogen-activated protein kinase) Signalweges, der eine wichtige Rolle
bei der Regulation von Transkriptionsfaktoren spielt, die Wachstum, Überleben,
Seneszenz und Differenzierung einer Zelle bestimmen (Fecher et al., 2008, Solus
und Kraft, 2013). Bei Melanompatienten ist BRAF in 44 bis 48% mutiert (Eigentler
et al., 2016, Greaves et al., 2013, Long et al., 2011, Menzies et al., 2012),
wodurch B-Raf Proteine mit einer erhöhten basalen Kinaseaktivität und
unabhängig von der Aktivität der vorgeschalteten Proteine entstehen können
(Davies et al., 2002). Spezifische B-Raf Inhibitoren stellen eine wirksame
Behandlungsoption des BRAF-mutierten Melanoms dar (Ugurel et al., 2017).
Es gibt Melanome ohne und mit Bezug zum Oberflächenepithel. Die Melanome
ohne Bezug zum Oberflächenepithel sind Melanozytome, Melanome der Uvea
und Melanome, die aus Blauen Nävi entstanden sind (Whiteman et al., 2011).
Diese Gruppe wird aufgrund ihrer Seltenheit nicht in dieser Studie untersucht. In
die Gruppe der Melanome mit Bezug zum Oberflächenepithel gehören 1)
Melanome auf Haut ohne chronischen Sonnenschaden (non chronic sun damage
melanomas/non-CSD melanomas), 2) Melanome auf Haut mit chronischem
Sonnenschaden (CSD melanomas), 3) mukosale Melanome und 4) akrolenti-
ginöse Melanome. Die Non-CSD melanomas sind bei Europäern der häufigste
Melanomsubtyp. Sie betreffen jüngere Menschen mit einer Vielzahl von Nävi und
Hautareale, die intermittierend der Sonne ausgesetzt sind. In 70% ist bei dieser
Subgruppe BRAF mutiert. Diese Entität überlappt sehr stark mit dem superfiziell
spreitenden und umfasst auch das noduläre Melanom. Letzteres ist jedoch
ebenso bei den CSD melanomas, akralen und mukosalen Melanomen vertreten.
CSD melanomas sind die zweithäufigste Entität der malignen Melanome bei
Europäern. Die Häufigkeit nimmt nach der 5. Lebensdekade zu. CSD melanomas
betreffen hauptsächlich die Körperareale Kopf, Nacken, sowie distale und dorsale
Extremität (Whiteman et al., 2011). Die Betroffenen zeigen auf der Haut wenige
4Nävi, jedoch solare Elastose und andere kutane Neoplasien. Als ursächlich wird
eine hohe, kumulative UV-Belastung der Haut angesehen. Auf molekularer Ebene
sind KIT oder NRAS zu 30-40% mutiert; BRAF ist weniger häufig als wie bei den
non-CSD melanomas mutiert. Akrolentiginöse und mukosale Melanome
entstehen ohne Einfluss von UV-Strahlung. Akrolentiginöse Melanome sind
Melanome der nicht behaarten Haut; sie treten an den Handflächen und
Fußsohlen, sowie subungual auf. Ihr Vorkommen ist in allen Weltpopulationen -
unabhängig vom genetischen Pigmentierungsgrad - gleich. In 20% ist KIT mutiert.
In 40% der Fälle kommt es zu einer Genominstabilität mit Amplifikation von
11q13 (Cyclin D1 Lokus). BRAF ist weniger häufig als wie bei den non-CSD
melanomas mutiert. Die mukosalen Melanome betreffen das
Schleimhautepithel des Oropharynx, der Nasennebenhöhlen, der tarsalen
Konjunktiva, sowie der anogenitalen Region. Auf molekularer Ebene treten unter
anderem Genominstabilitäten mit Amplifikation von CDK 4 (Chromosom 12q) auf
(Whiteman et al., 2011).
Das Melanom umfasst jedoch nicht nur verschiedene Subtypen (mit
unterschiedlichen Häufigkeiten von BRAF Mutationen); zusätzlich sind mehrere
BRAF Genotypen bekannt. BRAF befindet sich auf dem langen Arm von
Chromosom 7 (7q34) (Genome Data Viewer on NCBI, 2019). Die häufigste BRAF
Mutation ist mit circa 74-75% die V600E Mutation (Greaves et al., 2013, Long et
al., 2011, Menzies et al., 2012). Es handelt sich dabei um eine Punktmutation auf
Exon 15. Im Basenstrang der DNA wird an Position 1799 anstatt Thymin Adenin
eingebaut (1799T>A); dies entspricht der 2. Stelle im Codon 600 (GTG>GAG).
Dadurch wird nicht mehr die Aminosäure Valin (V), sondern Glutaminsäure (E)
kodiert (V600E) (Greaves et al., 2013, Lovly et al., 2015). Ein Teil der Patienten
trägt nicht-V600E BRAF Mutationen, von denen die meisten ebenfalls die Basen
des Codons 600 betreffen oder in wenigen Fällen in der Nachbarschaft davon
liegen. Die V600K Mutation kommt mit circa 20% besonders oft vor (17.2-20%
(Greaves et al., 2013, Long et al., 2011, Menzies et al., 2012)). Zu einem geringen
5Anteil treten BRAF Mutationen auf Exon 11 auf. In der Studie von Greaves et al.
waren es 0.4% (Greaves et al., 2013).
Obwohl mutiertes BRAF hauptsächlich in kutanen Melanomen vorkommt
(Greaves et al., 2013) und UV-Strahlung der hauptverursachende Umweltfaktor
ist (Whiteman et al., 2011), weisen überraschenderweise nur 2.4% der BRAF
Mutationen eine genetische Veränderung mit UVB-Signatur auf (das heißt
Cytosin zu Thymin Transitionen (G:C>A:T und GG:CC>AA:TT) an
Dipyrimidinstellen (Pfeifer et al., 2005)). Die BRAF Mutationen V600E und V600K
zählen nicht dazu (Hocker und Tsao, 2007). Die karzinogene Wirkung von UV-
Strahlung auf Melanozyten wird durch andere Mechanismen erklärt. UVA wird
nicht signifikant von DNA absorbiert, kann jedoch über die Bildung von Radikalen
oxidative DNA Schäden herbeiführen und bewirkt (zusammen mit UVB) eine
Immunsuppression (Kanavy und Gerstenblith, 2011, Pfeifer et al., 2005). Des
Weiteren gibt es neben BRAF (und NRAS) andere onkogenetische Hotspot
Mutationen beim Melanom. Die Dritthäufigste ist die RAC1 P29S Mutation, die
eine C>T Transition aufweist und vermutlich ausschließlich durch einen UVB
vermittelten DNA Schaden entsteht. Bei Hodis et al. kam diese Mutation in 3.9%
der Melanome vor (Hodis et al., 2012).
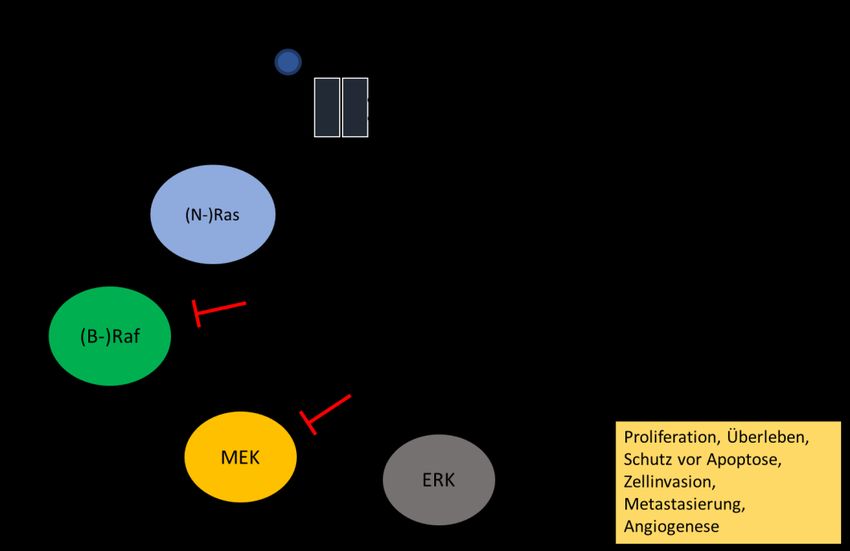
Das Proteinprodukt von BRAF ist - wie oben schon erwähnt - die Kinase B-Raf. Sie
ist Teil des MAPK Signalweges, der im physiologischen Zustand mittels
extrazellulärer Liganden - durch Bindung an einen Tyrosinkinase Rezeptor (RTK) -
aktiviert wird. Das Signal wird (vereinfacht dargestellt) mittels Adaptorproteinen
weitergeleitet und aktiviert Ras (hauptsächlich N-Ras), die unter anderem Raf
(beim Melanom hauptsächlich B-Raf) aktiviert. Der Aktivierungsprozess wird
über MEK an ERK weitergegeben. Aktiviertes ERK transloziert in den Zellkern und
interagiert mit Transkriptionsfaktoren, die die Genexpression für Proliferation,
Überleben, Apoptose, Zellinvasion, Metastasierung, sowie Angiogenese
6regulieren (Fecher et al., 2008, Satyamoorthy et al., 2003, Solus und Kraft, 2013)
(siehe Figur 1. MAPK Signalweg und Inhibitoren).
Figur 1. MAPK Signalweg und Inhibitoren
Ras GTPase. Raf Serin/Threonin Kinase. MEK Serin/Threonin/Tyrosin Kinase. ERK
Serin/Threonin Kinase. (Gene Cards, 2019a, Gene Cards, 2019b, Gene Cards, 2019c, Gene Cards, 2019d)
Mutierte B-Raf Kinasen weißen eine erhöhte Aktivität auf und steigern
nachfolgend die Aktivität von ERK (Davies et al., 2002). In diesen zellulären
Signalweg greifen die Kinaseinhibitoren ein und stellen eine wirksame
Behandlungsoption nicht resezierbarer oder metastasierter Melanom-
erkrankungen dar. Es gibt einerseits die seit 2011 und 2013 von der U.S. Food &
Drug Administration (FDA) für Melanompatienten mit einer BRAF V600E
Mutation zugelassenen B-Raf Inhibitoren Vemurafenib und Dabrafenib (U.S.
Food & Drug Administration, 2011a, U.S. Food & Drug Administration, 2013b).
Trametinib und Cobimetinib sind - seit jeweils 2013 und 2015 - zugelassene MEK
Inhibitoren (siehe Figur 1. MAPK Signalweg und Inhibitoren). Sie sind als
Einzeltherapeutikum (Trametinib) oder in Kombination mit Dabrafenib
(Trametinib) und Vemurafenib (Cobimetinib) bei Melanomen mit der BRAF
V600E oder V600K Mutation indiziert (U.S. Food & Drug Administration, 2013a,
7U.S. Food & Drug Administration, 2015). Die B-Raf und MEK Inhibitorkombination
aus Encorafenib und Binimetinib wurde 2018 zugelassen (U.S. Food & Drug
Administration, 2018). Somit stehen aktuell drei Kombinationen aus B-Raf- und
MEK-Inhibitoren für die Therapie von Melanompatienten mit BRAF-Mutation zur
Verfügung. In der Studie von Long et al. erreichte die Kombination von
Dabrafenib und Trametinib mit 25.1 Monaten ein längeres medianes
Gesamtüberleben als die Dabrafenib-Monotherapie mit 18.7 Monaten. Das
mediane progressionsfreie Überleben betrug in der Gruppe mit der
Kombinationstherapie 11 Monate, in der Gruppe mit der Monotherapie lag es
bei 8 Monaten (Long et al., 2015). Vemurafenib zeigte in Kombination mit
Cobimetinib bei Patienten mit BRAF V600 mutierten Melanomen ein medianes
Gesamtüberleben von 22.3 Monaten und ein medianes progressionsfreies
Überleben von 12.3 Monaten. In der Gruppe der Patienten, die eine
Vemurafenib Monotherapie erhielten, betrugen die Überlebenszeiten jeweils
17.4 (medianes Gesamtüberleben) und 7.2 Monate (medianes progressionsfreies
Überleben) (Ascierto et al., 2016). Encorafenib und Binimetinib zeigten ein
medianes progressionsfreies Überleben von 14.9 Monaten (Dummer et al.,
2018). Zusätzlich zu den BRAF V600E und V600K Genotypen zeigten weitere
nicht-V600E BRAF Mutationen ein Ansprechen auf die BRAF Inhibitortherapie. In
einem Fallbericht wies ein Patient - mit BRAF V600M positivem, metastasierten
Melanom und einer Kombinationstherapie aus Dabrafenib und Trametinib - ein
noch nach 10 Monaten anhaltendes Ansprechen auf (Parakh et al., 2015). In der
Studie von Klein et al. wurden sechs Patienten mit einem BRAF V600R positivem,
metastasierten Melanom klinisch und radiologisch nach einer Therapie mit
Dabrafenib oder Vemurafenib beurteilt. Hiervon zeigten fünf ein partielles
Ansprechen. Zwei weitere BRAF V600R mutierte Melanompatienten wiesen kurz
nach dem Beginn einer spezifischen BRAF Inhibitortherapie eine Verkleinerung
subkutaner Metastasen und einen Rückgang neurologischer Symptome auf (Klein
et al., 2013).
8In der vorliegenden Studie wurde die Häufigkeit der BRAF Genotypen Wildtyp,
V600E und nicht-V600E bei Patienten mit metastasiertem Melanom in den
folgenden Kategorien untersucht: 1) Histologischer Subtyp (superfiziell
spreitendes, noduläres, akrolentiginöses und mukosales Melanom, sowie
andere1), 2) Lokalisation kutaner Primärtumore (‚Rumpf‘, ‚Extremitäten‘ und
‚Kopf und Nacken‘) sowie 3) MUP (Melanoma of Unknown Primary).
Die Häufigkeitsverteilung von BRAF Mutationen je histologischen Subtyps wurde
unter anderem auch in der Studie von Menzies et al. untersucht. BRAF
Mutationen kamen bei den superfiziell spreitenden und nodulären Melanomen
jeweils zu 64 und 50% vor; bei den mukosalen und akrolentiginösen Melanomen
waren es jeweils 17 und 0%. Somit zeigte sich eine signifikante Assoziation
zwischen mutiertem BRAF und den superfiziell spreitenden und nodulären
Melanomen, sowie keine Assoziation zwischen mutiertem BRAF und den
mukosalen oder akrolentiginösen Melanomen (im Vergleich zum BRAF Wildtyp).
Eine Assoziation zwischen einem bestimmten mutierten BRAF Genotyp und
histologischem Subtyp kutaner Melanome ließ sich nicht nachweisen (Menzies et
al., 2012). In der vorliegenden Studie wurden ebenfalls die Häufigkeiten der BRAF
V600E und nicht-V600E Mutationen separat je nach histologischem Subtyp
untersucht. Insgesamt traten bei den superfiziell spreitenden, nodulären,
mukosalen und akrolentiginösen Melanomen zu jeweils 57.4, 54.7, 11.1 und
28.6% BRAF Mutationen auf. Signifikant war die Assoziation des mutierten BRAF
mit dem superfiziell spreitenden Melanom. Die Verteilung der spezifischen BRAF
Genotypen je Subtyp zeigte, dass die superfiziell spreitenden Melanome in 17%
und die nodulären Melanome in 9.4% der Fälle eine nicht-V600E BRAF Mutation
trugen. Die Patienten mit mukosalem und akrolentiginösem Melanom wiesen
keine nicht-V600E Mutation auf.
Aus diesen Ergebnissen folgernd sollten Patienten mit akrolentiginösem und
mukosalem Melanom ebenso standardmäßig auf BRAF V600 Mutationen
1 lentiginöses, nävoides, polypoides, spitzoides und desmoplastisches Melanom
9untersucht werden, denn entsprechende Mutationen kommen auch bei diesen
Subtypen vor und durch Unterlassung bliebe eine wirksame Behandlungsoption
unberücksichtigt. Des Weiteren sollte insbesondere bei den superfiziell
spreitenden und nodulären Melanomen ein Verfahren zur Mutationstestung
verwendet werden, dass die nicht-V600E BRAF Mutationen verlässlich nachweist,
damit die Indikationsstellung zur Therapie mit Kinaseinhibitoren erfolgen kann.
Die U.S. Food and Drug Administration fordert vor der Zuführung zu einer
Inhibitortherapie den BRAF Mutationsnachweis mittels COBAS 4800 BRAF V600
Mutation Test oder bioMérieux THxID BRAF Assay Kit. COBAS 4800 Test ist
zugelassen für die Therapie mit Vemurafenib bei Patienten mit der BRAF V600E
Mutation, THxID BRAF Assay Kit für die Therapie mit Dabrafenib und Trametinib
bei Patienten mit der BRAF V600E oder V600K Mutation. Aufgrund der im Test
verwendeten Primerpaare sind beide dafür ausgelegt ausschließlich die V600E
(COBAS 4800 Test) bzw. V600E und V600K Mutation (THxID BRAF Assay Kit) zu
detektieren (U.S. Food & Drug Administration, 2011b, U.S. Food & Drug
Administration, 2013c). Es gibt zwar Kreuzreaktivitäten zwischen den
Primerpaaren für andere nicht-V600E Mutationen, jedoch sind diese nicht
verlässlich. In der Zulassungsstudie von COBAS 4800 Test wurden beispielsweise
25 von 38 (65.8%) V600K Mutationen detektiert und zu einem geringen Teil
V600D und V600E2 (U.S. Food & Drug Administration, 2011b). Vergleichbare
Ergebnisse lieferte die Studie von Andersen et al.: COBAS 4800 Test erkannte
70% der V600K Mutationen (Anderson et al., 2012). In der Studie von Heinzerling
et al. wurden bei der Anwendung von COBAS 4800 Test von 14 Patienten mit
nicht-V600E Mutationen sieben detektiert (V600K 6 x, V600DK601del 1 x). Die
anderen sieben wurden nicht erkannt (darunter V600EK601del, V600D, V600G,
L597S, V600E2 (GAA), V600R) (Heinzerling et al., 2013). Die V600E PCR von THxID
BRAF Assay Kit kann zusätzlich die seltene Form der V600E Mutation (Codon
GAA), sowie die V600E/K601E Mutation erkennen. In der Zulassungsstudie zeigte
sich zudem eine Kreuzreaktion mit V600D; die Zuverlässigkeit wurde nicht
bestätigt (U.S. Food & Drug Administration, 2013c). Insgesamt bleiben dadurch
Patienten mit nicht-V600E Mutationen möglicherweise unentdeckt.
10Bei den Primärtumorlokalisationen kutaner Melanome - eingeteilt in
‚Extremitäten‘, ‚Rumpf‘ und ‚Kopf und Nacken‘ - weisen die BRAF Genotypen
signifikante Unterschiede auf. In der Studie von Menzies et al. waren in der
Gruppe der BRAF V600E mutierten Melanome die ‚Extremitäten‘ häufiger
betroffen als der ‚Kopf und Nacken‘. In der Gruppe der BRAF V600K mutierten
Melanome verhielt es sich umgekehrt; ein größerer Prozentsatz der
Primärtumore kam an ‚Kopf und Nacken‘ - im Vergleich zu den ‚Extremitäten‘ -
vor. In beiden Gruppen (BRAF V600E und V600K) war die jeweils häufigste
Primärtumorlokalisation der ‚Rumpf‘ (Menzies et al., 2012). In der vorliegenden
Studie wurde - im Unterschied zu Menzies et al. - die prozentuale Verteilung der
Genotypen in Bezug auf die Körperregionen nicht je nach Genotyp, sondern je
nach Körperregion untersucht. Begründung ist, dass die Körperregionen
unterschiedlich groß sind und es zu einer verzerrten Darstellung kommen könnte
(Whiteman et al., 2011). In unserer Kohorte waren am ‚Rumpf‘ jeweils 39.6%
BRAF V600E und 13.2% nicht-V600E BRAF mutiert. An den ‚Extremitäten‘ trugen
51.5% eine BRAF V600E Mutation und kein Primärtumor eine nicht-V600E
Mutation. An ‚Kopf und Nacken‘ waren 37.5% der Primärtumore BRAF V600E
und 25% nicht-V600E mutiert. Die Assoziation der ‚Extremitäten‘ mit der BRAF
V600E Mutation war signifikant.
Um die Ergebnisse von Menzies et al. mit unseren vergleichen zu können,
berechneten wir anhand der in Tabelle 1 in Menzies et al. aufgeführten Daten
(Menzies et al., 2012) die prozentuale Häufigkeit der nach Genotyp
unterschiedenen Primärtumoren je Körperregion aus. Es zeigte sich, dass in der
Studie von Menzies et al. am ‚Rumpf‘ 37.9% der Primärtumore BRAF V600E und
10.7% V600K mutiert waren. An den ‚Extremitäten‘ waren es jeweils 38.6%
(V600E) und 3.4% (V600K), an ‚Kopf und Nacken‘ 20.4% (V600E) und 16.7%
(V600K). Die Ergebnisse deckten sich mit unseren. Am ‚Rumpf‘ überwog die BRAF
V600E Mutation gegenüber den nicht-V600E BRAF mutierten Genotypen. An den
‚Extremitäten‘ kam hauptsächlich die BRAF V600E Mutation vor. An ‚Kopf und
11Nacken‘ war die prozentuale Häufigkeit der nicht-V600E BRAF mutierten
Primärtumore am größten.
Unter der Annahme, dass ‚Kopf und Nacken‘ (anders als ‚Extremitäten‘ und
‚Rumpf‘) mit einem hohen Grad an chronischem Sonnenschaden (CSD) assoziiert
ist (Curtin et al., 2005, Whiteman et al., 2011), könnte der BRAF Genotyp ein
weiterer Unterschied zwischen den CSD und non-CSD melanomas sein. Die nicht-
V600E BRAF Mutationen könnten - wie bereits auch durch Menzies et al.
vermutet - durch kumulative Dosen an UV-Strahlung und V600E BRAF
Mutationen durch intermittierende Sonneneinstrahlung hervorgerufen werden
(Menzies et al., 2012). Menzies et al. zeigte, dass zwar kein signifikanter
Unterschied zwischen dem Grad an CSD und dem Vorhandensein einer Mutation
bestand (BRAF mutiert versus BRAF Wildtyp), jedoch war innerhalb der Gruppe
der mutierten BRAF Genotypen BRAF V600K signifikant mit einem hohen Grad an
CSD und BRAF V600E mit einem niedrigen Grad oder keinem CSD assoziiert
(Menzies et al., 2012). Dazu passend ist die BRAF Mutationsverteilung je nach
Patientenalter unter der Annahme, dass mit steigendem Alter die UV-
Strahlenbelastung kumulativ höher ist als bei jüngeren Menschen. Menzies et al.
beschrieb, dass mit steigendem Alter die nicht-V600E BRAF Mutationen bei
kutanen Melanomen zunehmen. Weniger als 20% der Patienten unter 50 Jahren
mit einer BRAF Mutation wiesen einen nicht-V600E Genotyp auf. Bei den über
70-jährigen machten die nicht-V600E BRAF Mutationen mehr als 40% aus
(Menzies et al., 2012).
Ungefähr 4% aller Melanomerkrankungen weisen keinen Primärtumor auf
(MUP/Melanoma of Unknown Primary) (Chang und Knapper, 1982,
Panagopoulos und Murray, 1983, Schlagenhauff et al., 1997). Erklärungen für die
Abwesenheit eines sichtbaren Primärtumors sind bei Dutton-Regester et al.
zusammengefasst: Spontane Regression (Panagopoulos und Murray, 1983),
Entstehung aus Nävus-Vorläuferzellen in Lymphknoten (Ridolfi et al., 1977), ein
unerkannter oder bereits exzidierter und/oder fehldiagnostizierter Primärtumor,
12und der Ursprung an einer ungewöhnlichen oder versteckten Stelle (Dutton-
Regester et al., 2013, Hussein, 2008).
MUPs haben gegenüber Melanomerkrankungen mit bekanntem Primarius eine
bessere Prognose. Dieser Umstand spräche für die Hypothese der spontanen
Regression, wenn man davon ausgeht, dass diese eine bessere Immunreaktion
des Erkrankten bedeutet (Bae et al., 2015). Ebenso könnte es sein, dass
Nävuszellen in Lymphknoten wandern (metastasieren) und erst dort zu einem
invasiven Karzinom transformieren. Somit wären MUPs einem Primärtumor
ähnlicher als einem bereits metastasierten Tumor (Shain und Bastian, 2016).
Dutton-Regester et al. proklamierte des Weiteren einen kutanen Ursprung der
MUPs. In seiner Studie wurde nachgewiesen, dass in MUP-Zelllinien (mit einer
hohen Rate an Mutationen) der Anteil an C>T/G>A Transitionen erhöht ist und
somit auf Veränderungen durch UV-Strahlung hinweist. Des Weiteren neigten
MUPs dazu in Lymphknoten aufzutreten, welche sonnenexponierte Stellen
drainierten und MUPs zeigten häufig BRAF und NRAS Mutationen (Dutton-
Regester et al., 2013), die vor allem in kutanen Melanomen (CSD und non-CSD
melanomas) vorkommen (Curtin et al., 2005). In dieser Studie wurde bei den
MUPs das Verteilungsmuster der BRAF Genotypen untersucht. Die MUPs waren
zu 34.5% BRAF V600E und zu 10.3% nicht-V600E BRAF mutiert. In der Gruppe der
kutanen Melanome (superfiziell spreitendes und noduläres Melanom) waren es
43.0% (V600E) und 13.0% (nicht-V600E). Die mukosalen und akrolentiginösen
Melanome trugen keine nicht-V600E BRAF Mutation; der BRAF V600E Genotyp
lag in jeweils 11.1% (mukosales Melanom) und 28.6% (akrolentiginöses
Melanom) vor. Die höhere BRAF Mutationsrate der MUPs gegenüber den
mukosalen Melanomen war signifikant. Diese Ergebnisse stützen die Aussagen,
dass MUPs kutanen Ursprungs sein könnten.
In dem Artikel von Shain und Bastian (Shain und Bastian, 2016) werden die
neuen Kenntnisse über den Mutationsstatus bei Melanomen und deren
Vorläufern in Kombination mit histologischer Ausprägung, Alter und
13Körperlokalisation/CSD zusammengeführt. Es entstanden sechs Modelle der
kutanen Melanomgenese, welche die Darstellung der Melanomsubtypen in
Whiteman et al. (2011) präzisiert.
Ein Melanom-Subtyp (gehörend zu den non-CSD melanomas) entsteht aus
Melanozyten (hauptsächlich am Rumpf und den proximalen Extremitäten), die in
der ersten Lebensdekade eine BRAF V600E Mutation erwerben. Durch
Proliferation entstehen Nävi, die zwei bis drei Dekaden später nach dem Erwerb
einer TERT Promotor Mutation in Melanome in situ mit pagetoidem Wachstum
übergehen. Die Inaktivierung von CDKN2A und anderen Genen lässt invasive
Karzinome entstehen, zu denen auch die superfiziell spreitenden Melanome
gehören.
Jeweils ein weiterer Subtyp der CSD und non-CSD melanomas entsteht aus
Melanozyten mit vorbestehender pathogenetischer Variante. Diese Variante
kann sowohl somatisch erworben als auch bereits in der Keimbahn festgelegt
sein (es wird daher zwischen sporadischen und syndromalen Melanomen
unterschieden). Keimbahnvarianten, sowie häufige Mutationen in sporadischen
Melanomen sind genetische Veränderungen in CDKN2A, CDK4, TERT und POT1.
Eine aktivierende Mutation im MAPK Weg löst die Proliferation aus. Bei den non-
CSD melanomas ist dies vorwiegend eine BRAF V600E Mutation. Eine mögliche
Ausprägungsform des späteren invasiven Karzinoms ist - wie auch bei dem
vorher genannten Subtyp - das superfiziell spreitende Melanom. Bei den CSD
melanomas sind die Mutationen, welche die Proliferation initiieren, nicht-V600E
BRAF und NRAS Mutationen.
Noduläre Melanome sind sowohl den CSD als auch den non-CSD melanomas
gleichermaßen zugeordnet. Sie sind definiert durch die Abwesenheit einer
erkennbaren Vorläuferläsion. Zugrundeliegend sind in rascher Folge auftretende
Mutationen oder in bestimmten Melanozyten bereits vorhandene sekundäre
und tertiäre Mutationen. Eine aktivierende MAPK Mutation (siehe oben) löst
sodann die Proliferation und Karzinogenese aus.
14Die Lentigo Maligna Melanome sind auf Körperarealen mit schwerem
Sonnenschaden (CSD melanoma) lokalisiert und entstehen aus der Lentigo
Maligna, einem Melanoma in situ. Sie korrelieren invers mit der BRAF V600E
Mutation und treten vornehmlich bei älteren Menschen auf (Shain und Bastian,
2016).
153. Literaturverzeichnis / References
Anderson S, Bloom KJ, Vallera DU, Rueschoff J, Meldrum C, Schilling R, Kovach B, Lee JR,
Ochoa P, Langland R, Halait H, Lawrence HJ , Dugan MC (2012) Multisite analytic
performance studies of a real-time polymerase chain reaction assay for the detection of
BRAF V600E mutations in formalin-fixed, paraffin-embedded tissue specimens of
malignant melanoma. Arch Pathol Lab Med. 136:1385-1391.
http://www.archivesofpathology.org/doi/pdf/10.5858/arpa.2011-0505-OA
Ascierto PA, McArthur GA, Dreno B, Atkinson V, Liszkay G, Di Giacomo AM, Mandala M,
Demidov L, Stroyakovskiy D, Thomas L, de la Cruz-Merino L, Dutriaux C, Garbe C, Yan Y,
Wongchenko M, Chang I, Hsu JJ, Koralek DO, Rooney I, Ribas A , Larkin J (2016)
Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma
(coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial.
Lancet Oncol. 17:1248-1260.
Bae JM, Choi YY, Kim DS, Lee JH, Jang HS, Lee JH, Kim H, Oh BH, Roh MR, Nam KA , Chung
KY (2015) Metastatic melanomas of unknown primary show better prognosis than those
of known primary: a systematic review and meta-analysis of observational studies. J Am
Acad Dermatol. 72:59-70.
Chang P , Knapper WH (1982) Metastatic melanoma of unknown primary. Cancer.
49:1106-1111.
Curtin JA, Fridlyand J, Kageshita T, Patel HN, Busam KJ, Kutzner H, Cho KH, Aiba S,
Brocker EB, LeBoit PE, Pinkel D , Bastian BC (2005) Distinct sets of genetic alterations in
melanoma. N Engl J Med. 353:2135-2147.
Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, Teague J, Woffendin H,
Garnett MJ, Bottomley W, Davis N, Dicks E, Ewing R, Floyd Y, Gray K, Hall S, Hawes R,
Hughes J, Kosmidou V, Menzies A, Mould C, Parker A, Stevens C, Watt S, Hooper S,
Wilson R, Jayatilake H, Gusterson BA, Cooper C, Shipley J, Hargrave D, Pritchard-Jones K,
Maitland N, Chenevix-Trench G, Riggins GJ, Bigner DD, Palmieri G, Cossu A, Flanagan A,
Nicholson A, Ho JW, Leung SY, Yuen ST, Weber BL, Seigler HF, Darrow TL, Paterson H,
16Marais R, Marshall CJ, Wooster R, Stratton MR , Futreal PA (2002) Mutations of the BRAF
gene in human cancer. Nature. 417:949-954.
Dummer R, Ascierto PA, Gogas HJ, Arance A, Mandala M, Liszkay G, Garbe C,
Schadendorf D, Krajsova I, Gutzmer R, Chiarion-Sileni V, Dutriaux C, de Groot JWB,
Yamazaki N, Loquai C, Moutouh-de Parseval LA, Pickard MD, Sandor V, Robert C ,
Flaherty KT (2018) Encorafenib plus binimetinib versus vemurafenib or encorafenib in
patients with BRAF-mutant melanoma (COLUMBUS): a multicentre, open-label,
randomised phase 3 trial. Lancet Oncol. 19:603-615.
Dutton-Regester K, Kakavand H, Aoude LG, Stark MS, Gartside MG, Johansson P,
O'Connor L, Lanagan C, Tembe V, Pupo GM, Haydu LE, Schmidt CW, Mann GJ, Thompson
JF, Scolyer RA , Hayward NK (2013) Melanomas of unknown primary have a mutation
profile consistent with cutaneous sun-exposed melanoma. Pigment Cell Melanoma Res.
26:852-860.
Eigentler T, Assi Z, Hassel JC, Heinzerling L, Starz H, Berneburg M, Bauer J , Garbe C
(2016) Which melanoma patient carries a BRAF-mutation? A comparison of predictive
models. Oncotarget. 7:36130-36137.
Fecher LA, Amaravadi RK , Flaherty KT (2008) The MAPK pathway in melanoma. Curr
Opin Oncol. 20:183-189.
Gene Cards (2019a) BRAF Gene (Protein Coding) P-Raf Proto-Oncogene,
Serine/Threonine Kinase GCID: GC07M140719. Available from www.genecards.org/cgi-
bin/carddisp.pl?gene=BRAF&keywords=BRAF [accessed 2019-01-27, 10:22].
Gene Cards (2019b) MAP2K1 Gene (Protein Coding) Mitogen-Activated Protein Kinase
Kinase 1 GCID: GC15P066386. Available from www.genecards.org/cgi-
bin/carddisp.pl?gene=MAP2K1&keywords=MEK [accessed 2019-01-27, 11:30].
Gene Cards (2019c) MAPK1 Gene (Protein Coding) Mitogen-Activated Protein Kinase 1
GCID: GC22M021754. Available from www.genecard.org/cgi-
bin/carddisp.pl?gene=MAPK1&keywords=ERK [accessed 2019-01-27, 11:35].
17Gene Cards (2019d) NRAS Gene (Protein Coding) NRAS Proto-oncogene, GTPase GCID:
GC01M114704. Available from www.genecards.org/cgi-
bin/carddisp.pl?gene=NRAS&keywords=ras [accessed 2019-01-27, 11:20].
Genome Data Viewer on NCBI (2019) BRAF B-RAF proto-oncogene, serine/threonine
kinase [Homo sapiens (human)]. Available from
https://www.ncbi.nlm.nih.gov/gene?Db=gene&Cmd=DetailsSearch&Term=673
[accessed 2019-01-15, 10:00].
Greaves WO, Verma S, Patel KP, Davies MA, Barkoh BA, Galbincea JM, Yao H, Lazar AJ,
Aldape KD, Medeiros LJ , Luthra R (2013) Frequency and spectrum of BRAF mutations in
a retrospective, single-institution study of 1112 cases of melanoma. J Mol Diagn. 15:220-
226.
Heinzerling L, Kuhnapfel S, Meckbach D, Baiter M, Kaempgen E, Keikavoussi P, Schuler G,
Agaimy A, Bauer J, Hartmann A, Kiesewetter F , Schneider-Stock R (2013) Rare BRAF
mutations in melanoma patients: implications for molecular testing in clinical practice.
Br J Cancer. 108:2164-2171.
Hocker T , Tsao H (2007) Ultraviolet radiation and melanoma: a systematic review and
analysis of reported sequence variants. Hum Mutat. 28:578-588.
Hodis E, Watson IR, Kryukov GV, Arold ST, Imielinski M, Theurillat JP, Nickerson E, Auclair
D, Li L, Place C, Dicara D, Ramos AH, Lawrence MS, Cibulskis K, Sivachenko A, Voet D,
Saksena G, Stransky N, Onofrio RC, Winckler W, Ardlie K, Wagle N, Wargo J, Chong K,
Morton DL, Stemke-Hale K, Chen G, Noble M, Meyerson M, Ladbury JE, Davies MA,
Gershenwald JE, Wagner SN, Hoon DS, Schadendorf D, Lander ES, Gabriel SB, Getz G,
Garraway LA , Chin L (2012) A landscape of driver mutations in melanoma. Cell. 150:251-
263.
Hussein MR (2008) Extracutaneous malignant melanomas. Cancer Invest. 26:516-534.
Kanavy HE , Gerstenblith MR (2011) Ultraviolet radiation and melanoma. Semin Cutan
Med Surg. 30:222-228.
18Klein O, Clements A, Menzies AM, O'Toole S, Kefford RF , Long GV (2013) BRAF inhibitor
activity in V600R metastatic melanoma. Eur J Cancer. 49:1073-1079.
Long GV, Menzies AM, Nagrial AM, Haydu LE, Hamilton AL, Mann GJ, Hughes TM,
Thompson JF, Scolyer RA , Kefford RF (2011) Prognostic and clinicopathologic
associations of oncogenic BRAF in metastatic melanoma. J Clin Oncol. 29:1239-1246.
Long GV, Stroyakovskiy D, Gogas H, Levchenko E, de Braud F, Larkin J, Garbe C, Jouary T,
Hauschild A, Grob JJ, Chiarion-Sileni V, Lebbe C, Mandala M, Millward M, Arance A,
Bondarenko I, Haanen JB, Hansson J, Utikal J, Ferraresi V, Kovalenko N, Mohr P,
Probachai V, Schadendorf D, Nathan P, Robert C, Ribas A, DeMarini DJ, Irani JG, Swann S,
Legos JJ, Jin F, Mookerjee B , Flaherty K (2015) Dabrafenib and trametinib versus
dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-
blind, phase 3 randomised controlled trial. Lancet. 386:444-451.
Lovly CM, Pao W , Sosman J (2015) BRAF c.1799T>A (V600E) Mutation in Melanoma.
Available from My Cancer Genome
https://www.mycancergenome.org/content/disease/melanoma/braf/54/ [accessed
2018-11-26, 10:45].
Menzies AM, Haydu LE, Visintin L, Carlino MS, Howle JR, Thompson JF, Kefford RF,
Scolyer RA , Long GV (2012) Distinguishing clinicopathologic features of patients with
V600E and V600K BRAF-mutant metastatic melanoma. Clin Cancer Res. 18:3242-3249.
Panagopoulos E , Murray D (1983) Metastatic malignant melanoma of unknown primary
origin: a study of 30 cases. J Surg Oncol. 23:8-10.
Parakh S, Murphy C, Lau D, Cebon JS , Andrews MC (2015) Response to MAPK pathway
inhibitors in BRAF V600M-mutated metastatic melanoma. J Clin Pharm Ther. 40:121-
123.
Pfeifer GP, You YH , Besaratinia A (2005) Mutations induced by ultraviolet light. Mutat
Res. 571:19-31.
Ridolfi RL, Rosen PP , Thaler H (1977) Nevus cell aggregates associated with lymph
nodes: estimated frequency and clinical significance. Cancer. 39:164-171.
19Satyamoorthy K, Li G, Gerrero MR, Brose MS, Volpe P, Weber BL, Van Belle P, Elder DE ,
Herlyn M (2003) Constitutive mitogen-activated protein kinase activation in melanoma
is mediated by both BRAF mutations and autocrine growth factor stimulation. Cancer
Res. 63:756-759.
Schlagenhauff B, Stroebel W, Ellwanger U, Meier F, Zimmermann C, Breuninger H,
Rassner G , Garbe C (1997) Metastatic melanoma of unknown primary origin shows
prognostic similarities to regional metastatic melanoma: recommendations for initial
staging examinations. Cancer. 80:60-65.
Shain AH , Bastian BC (2016) From melanocytes to melanomas. Nat Rev Cancer. 16:345-
358.
Solus JF , Kraft S (2013) Ras, Raf, and MAP kinase in melanoma. Adv Anat Pathol. 20:217-
226.
U.S. Food & Drug Administration (2011a) Drug Approval Package: Zelboraf
(vemurafenib) tablet (Approval Letter(s)) Available from
https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/202429s000TOC.cfm
[accessed 2019-03-21, 10:25].
U.S. Food & Drug Administration (2011b) List of Nucleic Acid Based Tests: Roche cobas
DNA Sample Preparation Kit, COBAS 4800 BRAF V600 MUTATION TEST (Summary of
Safety and Effectiveness). Available from
https://www.fda.gov/medicaldevices/productsandmedicalprocedures/invitrodiagnostics
/ucm330711.htm [accessed 2018-05-28, 09:50].
U.S. Food & Drug Administration (2013a) Drug Approval Package: Mekinist (trametinib)
Tablets (Printed Labeling). Available from
https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204114Orig1s000TOC.cfm
[accessed 2019-03-21, 10:40].
U.S. Food & Drug Administration (2013b) Drug Approval Package: Tafinlar (dabrafenib)
Capsules (Approval Letter(s)). Available from
https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/202806Orig1s000TOC.cfm
[accessed 2019-03-21, 10:30].
20U.S. Food & Drug Administration (2013c) List of Nucleic Acid Based Test: THXID-BRAF KIT
(Labeling). Available from
https://www.fda.gov/medicaldevices/productsandmedicalprocedures/invitrodiagnostics
/ucm330711.htm [accessed 2017-10-28, 21:05].
U.S. Food & Drug Administration (2015) Cotellic (cobimetinib) tablet (Printed Labeling).
Available from
https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/206192Orig1s000TOC.cfm
[accessed 2019-03-21, 10:45].
U.S. Food & Drug Administration (2018) Drug Approval Package: Mektovi (Approval
Letter(s)). Available from
https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/210498Orig1s000TOC.cfm
[accessed 2019-03-20, 12:50].
Ugurel S, Rohmel J, Ascierto PA, Flaherty KT, Grob JJ, Hauschild A, Larkin J, Long GV,
Lorigan P, McArthur GA, Ribas A, Robert C, Schadendorf D , Garbe C (2017) Survival of
patients with advanced metastatic melanoma: the impact of novel therapies-update
2017. Eur J Cancer. 83:247-257.
Whiteman DC, Pavan WJ , Bastian BC (2011) The melanomas: a synthesis of
epidemiological, clinical, histopathological, genetic, and biological aspects, supporting
distinct subtypes, causal pathways, and cells of origin. Pigment Cell Melanoma Res.
24:879-897.
214. Orginalpublikation / Original article
Pathogenetic Implications of BRAF Mutation
Distribution in Stage IV Melanoma Patients
Pathogenetische Bedeutung der Verteilung von BRAF
Mutationen bei Patienten mit Melanom
22Original Paper
Dermatology 2015;231:127–133 Received: September 26, 2014
Accepted after revision: March 23, 2015
DOI: 10.1159/000381849
Published online: June 27, 2015
Pathogenetic Implications of
BRAF Mutation Distribution in Stage IV
Melanoma Patients
Mirjam Baiter a Gerold Schuler a Arndt Hartmann b Regine Schneider-Stock b, c
Lucie Heinzerling a
a
Department of Dermatology, b Institute of Pathology and c Experimental Tumor Pathology, University Hospital
Erlangen, Friedrich Alexander University Erlangen-Nürnberg, Erlangen, Germany
Key Words pend on histological subtype and localization of primary
Histological melanoma subtypes · Localization of primary · melanoma. Non-V600E BRAF mutations mostly occur in pa-
Melanoma of unknown primary · Acral lentiginous tients with primaries on ‘head and neck’ as well as ‘trunk’ but
melanoma · Mucosal melanoma · Pathogenesis not on ‘extremities’. © 2015 S. Karger AG, Basel
Abstract
Background: BRAF mutation frequencies in melanoma sub- Introduction
types have clinical implications and offer pathogenetic clues.
Objectives: To characterize BRAF mutation status in mela- Since 2011 and 2013 the BRAF inhibitors vemurafenib
noma of unknown primary (MUP) patients, in histological and dabrafenib have been approved by the Food and Drug
melanoma subtypes and by localization of primary tumors. Administration to treat unresectable or metastatic mela-
Methods: In 179 patients with stage IV metastatic melano- noma in patients with BRAF V600 mutations. Although
ma, BRAF mutation status, histological subtype and localiza- BRAF inhibitors achieve a median progression-free sur-
tion of primary (except for 29 MUP patients) were analyzed. vival of 5.3 (vemurafenib) and 5.1 months (dabrafenib) [1,
Results: BRAF mutations were found in 44.3%, of which 2], resistance develops under treatment [3, 4]. Thus, meta-
80.5% were BRAF V600E and 19.5% showed non-V600E BRAF static melanoma remains incurable with a 1-year survival
mutations. BRAF mutation frequency depended on histolog- rate of 83% in patients with stage IV BRAF mutant mela-
ical subtype (57.4% superficial spreading melanoma, 54.7% noma treated with a BRAF inhibitor, 29% BRAF mutant
nodular melanoma, 11.1% mucosal melanoma, 28.6% acral melanoma not treated with a BRAF inhibitor, and 37% in
lentiginous melanoma) and concerning non-V600E BRAF
mutations on localization of primary. In MUP the BRAF muta-
tion pattern resembled superficial spreading and nodular The present work was performed in fulfillment of the requirements
melanomas. Conclusion: BRAF mutation frequencies de-
Universitaetsbibliothek Erlangen-Nuernberg
for obtaining the degree Dr.med.
149.126.78.65 - 12/15/2015 12:13:24 PM
© 2015 S. Karger AG, Basel Lucie Heinzerling, MD, PhD, MPH
1018–8665/15/2312–0127$39.50/0 Department of Dermatology
University Hospital Erlangen
Downloaded by:
E-Mail karger@karger.com
DE–91052 Erlangen (Germany)
www.karger.com/drm
E-Mail lucie.heinzerling @ uk-erlangen.depatients with BRAF wild-type melanoma [5]. Recently, Furthermore, about 4% of all melanomas are melano-
trametinib, an oral selective MEK inhibitor, was approved mas of unknown primary (MUPs), and thus their origin
[6] and the combination of dabrafenib plus trametinib is unknown [22–25]. Explanations for the absence of a
showed response rates of 76% compared to 54% with dab- visible primary include spontaneous regression of the
rafenib monotherapy [7, 8]. Likewise, the combination of primary tumor [23, 25], origin from ancestral nevus cells
vemurafenib and the MEK inhibitor cobimetinib has in lymph nodes [26], an unrecognized primary tumor or
shown response rates of 68% compared to 45% with ve- a previously excised but misdiagnosed lesion, or origin
murafenib monotherapy and significant improvement in at an unusual or concealed primary site [27]. First studies
progression-free survival with 9.9 months compared to 6.2 investigating mutation status have indicated a mutation
months among patients with BRAF V600-mutated meta- profile consistent with cutaneous melanomas rather
static melanoma [9]. Most BRAF mutations are V600E, than from melanomas of acral, mucosal or uveal origins,
although a subset of patients exhibits non-V600E exon 15 on grounds of increased C>T/G>A alterations, frequent
mutations at or around V600. Both, melanomas carrying oncogenic mutations in BRAF and NRAS, and a propen-
BRAF V600E and non-V600E mutations, have been shown sity for tumors to arise in skin-draining lymph nodes
to respond to mitogen-activated protein (MAP) kinase in- [27].
hibition [1–3, 7, 9–11]. Since inhibition of the MAP kinase This study investigates the distribution of BRAF muta-
pathway is an effective treatment in patients exhibiting the tions in melanomas according to localization and histo-
BRAF V600 mutation, it is essential to acquire knowledge logical subtype. It compares the BRAF mutation profile
about the distribution of these mutations. of MUPs with those with known primary.
Interestingly, the historical melanoma subtypes classi-
fied by anatomical site show a differential distribution of
mutation frequencies [12]. BRAF mutations in cutaneous
Patients and Methods
melanomas without chronic sun-induced damage yielded
a BRAF mutation rate of 59%, while other cutaneous mel- Patients
anomas on skin with chronic sun-induced damage, mu- A total of 179 consecutive stage IV metastatic melanoma pa-
cosal and acral melanomas showed a comparatively lower tients (excluding uveal melanoma) with 185 tumor lesions (156
BRAF mutation rate with 11, 11 and 23%, respectively [13, primary tumors, 29 melanoma metastases with unknown primary)
consulting the University Hospital Erlangen were reviewed. Data
14]. Although it has been shown in epidemiologic studies on the patients’ histological melanoma subtype, localization of pri-
that ultraviolet (UV) light plays a causative role in the de- mary tumor and BRAF mutation status were gathered from patient
velopment of cutaneous malignant melanomas (reviewed files.
in Whiteman et al. [15]), its role for the most common One patient showed two histological components in the pri-
melanoma-associated mutations remains controversial mary tumor, the nodular and the superficial spreading subtypes,
and was thus counted as two tumor samples. Five patients pre-
since BRAF V600E and NRAS Q61L/R do not carry the sented with two primary tumors, respectively. In 5 cases there were
genetic alterations typically provoked by UV light [16, 17]. no data available on histological melanoma subtype, so these pa-
UV-induced mutations present as alterations in adjacent tients were excluded from our calculations.
pyrimidines with the transcription errors G:C>A:T or
GG:CC>AA:TT. The latter, cytosine tandem mutation, is Tumor Samples
Tumor material was taken from 185 formalin-fixed paraffin-
considered as specific marker of UVB-induced gene al- embedded tissue samples from metastatic lesions with 48.7% skin
teration [18, 19]. Since only 2% of the BRAF (not at codon metastases, 8.3% lymph node metastases, 10.9% visceral metasta-
600) and 15% of the NRAS mutations in melanoma car- ses and from 43 primary tumors (16.2%). In 15.8% there were no
ry mutations specific for UVB [20], malignant transfor- data available which localization the sample for mutation analysis
mation may be explained by the sun’s ability to generate was taken from.
reactive oxygen species, inflammation and immunosup- DNA Extraction and Mutation Analysis
pression [19]. In favor of the sun’s direct involvement in DNA extraction and mutation analysis were performed as de-
melanomagenesis are statistically significant hot spot mu- scribed recently in Heinzerling et al. [28]. Briefly, genomic DNA
tations in three melanoma genes (RAC1, STK19, PPP6C) was extracted from 2- to 3.5-µm sections of formalin-fixed paraf-
fin-embedded tissue blocks. The relevant tumor area was marked
linking UVB mutagenesis mechanistically to this malig-
by a pathologist (A.H.) and microdissected. After deparaffiniza-
nancy [17]. Additionally, p53 previously thought not to be tion, DNA was prepared as described recently using the Nu-
relevant in melanomagenesis has been shown to accelerate cleoSpin® Tissue kit according to the manufacturer’s instructions
BRAF V600E-driven melanomagenesis [21]. [29].
Universitaetsbibliothek Erlangen-Nuernberg
149.126.78.65 - 12/15/2015 12:13:24 PM
128 Dermatology 2015;231:127–133 Baiter/Schuler/Hartmann/
DOI: 10.1159/000381849 Schneider-Stock/Heinzerling
Downloaded by:DNA was amplified using the multiplex PCR kit according to Table 1. Distribution of BRAF mutations in histological melanoma
the instructions of the manufacturer (Qiagen, Hilden, Germany) subtypes
and the following primers: forward: 5′-TGA AGA CCT CAC AGT
AAA AAT AGG-3′, and reverse: 5′-biotin AAA ATG GAT CCA Melanoma BRAF BRAF Non-V600E Total
GAC AAC TGT TC-3′. The cycling was performed as follows: a subtype wild-type V600E BRAF
single cycle of denaturation at 95 ° C for 15 min, 42 cycles of 95 ° C mutation mutation
for 20 s, 61 ° C for 30 s and 72 ° C for 5 min, and a final 5-min exten-
sion at 72 ° C. For pyrosequencing (PyroMark Q24, Qiagen) single- SSM 20 (42.6) 19 (40.4) 8 (17.0) 47
stranded DNA was prepared from 40 µl biotinylated PCR product NM 24 (45.3) 24 (45.3) 5 (9.4) 53
with streptavidin-coated sepharose and 0.5 µM of the sequencing ALM 10 (71.4) 4 (28.6) – 14
primer: 5′-GGT GAT TTT GGT CTA GC-3′ using the PSQ Vac- Mucosal melanoma 24 (88.9) 3 (11.1) – 27
uum Prep Tool (Qiagen). The setup for the pyrosequencing assay Other 6 (60.0) 4 (40.0) – 10
was selected with the following sequence in ‘sequence to analyze’: MUP 16 (55.2) 10 (34.5) 3 (10.3) 29
TACAGA/TGAAA. The A/T describes the hot spot mutation site All 100 64 16 180
at codon 600 and primarily describes the V600E with a substitu-
tion of GTG (valine) by GAG (glutamic acid). The following dis- Values are numbers of tumor probes with percentages in pa-
pensation order was used: GTACACGATG. The ‘C’ was included rentheses. Other = Lentigo maligna melanoma, nevoid, polypoid,
as an internal control. desmoplastic and spitzoid melanoma.
Statistical Analyses
Fisher’s exact test was used to test for correlations.
Distribution of BRAF Mutations Depending on
Histological Subtype and Localization of the Primary
Results Tumor
The BRAF V600E mutation rates in SSM and NM were
A total of 179 patients were characterized for BRAF 40.4 and 45.3%, respectively. ALM and mucosal melano-
mutation status. Out of these, 145 patients had 151 pri- ma showed a lower BRAF V600E mutation rate with
mary tumors which were additionally assessed for histo- 28.6% (ALM) and 11.1% (mucosal melanoma), respec-
logical subtype and localization. Twenty-nine patients tively. While none of ALM or mucosal melanoma carried
had MUPs and 5 patients presented without data on the a non-V600E BRAF mutation, 17.0% of the SSM and
primary tumor. To acquire BRAF mutation status, an ac- 9.4% of the NM subtypes presented with a non-V600E
cessible tumor sample was analyzed including primary BRAF mutation (table 1). BRAF mutations were signifi-
tumors, skin metastases, lymph nodes and distant metas- cantly associated with SSM (p = 0.042) and showed a ten-
tases (lung, liver, gastric, pancreas, brain, intestinal, soft dency of association with NM (p = 0.099). ALM was not
tissue). BRAF wild-type was present in 55.7% (n = 103) associated with BRAF mutation status (p = 0.269), while
and mutant BRAF in 44.3% (n = 82) of tumor samples. In mucosal melanoma was highly significantly associated
the group with BRAF mutations, 80.5% (n = 66) were with BRAF wild-type (p < 0.001). The difference in fre-
BRAF V600E and 19.5% (n = 16) non-V600E BRAF mu- quency of non-V600E BRAF mutations in NM and SSM
tations including the variants V600K, V600G, V600D, was not significant (p = 0.373).
V600D K601del, V600R, L597S, V600E (GAA), V600E Analysis of frequency of BRAF mutations in cutaneous
K601del (details published in [30]). melanomas on ‘head and neck’, ‘trunk’ and ‘extremities’
There were 5 patients who presented with two primary showed the highest BRAF mutation rates in melanomas
tumors. Both tumors in each patient carried the same mu- on ‘head and neck’ (62.5%), followed by ‘trunk’ (52.8%)
tation. SSM (superficial spreading melanoma) was present and ‘extremities’ (51.5%; fig. 1). The proportion of BRAF
in 26.1% (n = 47), NM (nodular melanoma) in 29.4% (n = V600E mutations was at all body sites higher than the
53), ALM (acral lentiginous melanoma) in 7.8% (n = 14) proportion of non-V600E BRAF mutations, but not
and mucosal melanoma in 15.0% (n = 27). Overall, 5.6% equally distributed. While on ‘trunk’ 39.6% of cutaneous
(n = 10) presented with other cutaneous melanoma sub- melanomas showed V600E and 13.2% non-V600E BRAF
types (lentigo maligna melanoma, n = 1; desmoplastic mutations, on ‘head and neck’ it was 37.5 vs. 25.0%, re-
melanoma, n = 2; nevoid melanoma, n = 5; polypoid mel- spectively. Strikingly, patients with primary tumors on
anoma, n = 1; spitzoid melanoma, n = 1). In 16.1% (n = ‘extremities’ never presented with non-V600E BRAF mu-
29) no primary tumor could be detected (MUP). tations and thus showed a statistically significant associa-
tion with the BRAF V600E mutation (51.1%, p = 0.012;
Universitaetsbibliothek Erlangen-Nuernberg
149.126.78.65 - 12/15/2015 12:13:24 PM
Distribution of BRAF Mutations Dermatology 2015;231:127–133 129
DOI: 10.1159/000381849
Downloaded by:Head and neck: 62.5% BRAF mutated
37.5% BRAF V600E mutations, 25% non-V600E BRAF mutations (p = 0.07)
Trunk: 52.8% BRAF mutated
39.6% BRAF V600E mutations, 13.2% non-V600E BRAF mutations (p = 0.755)
Extremities: 51.5% BRAF mutated
51.5% BRAF V600E mutations, 0% non-V600E BRAF mutations (p = 0.012)
Cutaneous melanomas on ‘head and neck’, ‘trunk’ and ‘extremities’: SSM; NM; lentigo maligna melanoma; nevoid, polypoid, spitzoid
and desmoplastic melanoma.
p values indicate correlations between BRAF mutation status and body site.
Fig. 1. Distribution of V600E and non-V600E BRAF mutations in cutaneous melanomas on ‘head and neck’, ‘trunk’ and ‘extremities’.
Table 2. Comparison of results between this study and Menzies et al. [5] concerning BRAF mutation status of the primary site
Primary site This study Menzies et al.
head and trunk extremities data presented in published paper (table 1) calculated data for comparison1
neck
head and trunk extremities head and trunk extremities
neck neck
Wild-type 9 (37.5) 25 (47.2) 16 (48.5) 34 (58.0) 53 (50.0) 51 (59.0) 34 (62.9) 53 (51.4) 51 (58.0)
Mutant BRAF 15 (62.5) 28 (52.8) 17 (51.5) 24 (42.0) 54 (50.0) 37 (41.0) 20 (37.1) 50 (48.6) 37 (42.0)
V600E 9 (37.5) 21 (39.6) 17 (51.5) 11 (20.4) 39 (37.9) 34 (38.6)
Non-V600E 6 (25.0) 7 (13.2) 0 (0.0) 9 (16.7)2 11 (10.7)2 3 (3.4)2
Total 24 53 33 58 107 88 54 103 88
Data are expressed as numbers of tumor probes with percentages in parentheses.
1 Synopsis of data and calculation of percentages were performed within this study to allow comparison between our data and the
data from Menzies et al. [table 1 (numbers of BRAF wild-type) and table 2 (numbers of BRAF V600E and V600K)].
2
The data from Menzies et al. comprise BRAF V600K mutations only.
Universitaetsbibliothek Erlangen-Nuernberg
149.126.78.65 - 12/15/2015 12:13:24 PM
130 Dermatology 2015;231:127–133 Baiter/Schuler/Hartmann/
DOI: 10.1159/000381849 Schneider-Stock/Heinzerling
Downloaded by:Sie können auch lesen

















































