Achalasie: Methodenvergleich - Georg Spaun
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Achalasie: Methodenvergleich Georg Spaun

Epidemiologie der Achalasie
! Historisch: 0.5-1.2 von 100.000 / Jahr
! neuere Daten: 1.6 - 2.5 von 100.000 /
Jahr
! Männer und Frauen gleich betroffen
! zweigipfelige Alters Verteilung:
! 1. Gipfel: dritte bis vierte Dekade
! 2. Gipfel: nach 60 Lj.
O’Neill OM, Johnston BT, Coleman HG. Achalasia: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J
Gastroenterol 2013; 19(35): 5806-58 Duffield JA, Hamer PW, Heddle R, Holloway RH, Myers JC, Thompson SK (2016) Incidence of Achalasia
in south Australia based on esophageal manometry findings. Clin Gastroenterol Hepatol. doi:10.1016/j.cgh.2016.05.036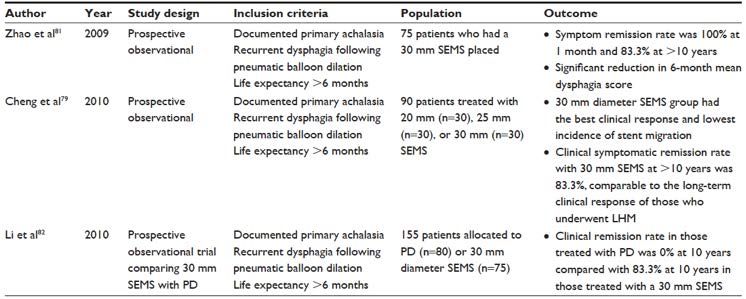
Achalasie
! progressiver Erkrankungsprozess
! Behandlungskonzepte derzeit per Definition
palliativ (neurale Destruktion)
! Heilung kann dzt. nicht erreicht werden
! therapeutischer Erfolg daher relativer Begriff:
! weitgehend definiert von Wahrnehmung des
Pat. betreffend Symptomfreiheit
! Prävention oder Therapie von
Komplikationen
Thomas Watson, World J Surg (2015) 39:1634–1641
Georg Spaun, EndoLinz 1-2018
Achalasie Therapie
! Gratwanderung
zwischen Dysphagie und gastroösophagealem Reflux
Georg Spaun, EndoLinz 1-2018
! 331 Patienten mit pneumatischer Dilatation systematisch
nachuntersucht mittels Gastroskopie und PE’s
! 40% der Pat. entwickeln chronisch aktive oder ulzerierende
Ösophagitis
! Barrett: 37 Pat: (14.7%) nach mittlerem Follow-up von 6 Jahren
! von diesen Pat: 32.4% LGD, 1 HGD, 3 Adenokarzinome
Georg Spaun, EndoLinz 1-2018 Leeuwenburgh et al; Aliment Pharmacol Ther 23, 2005, 1197–1203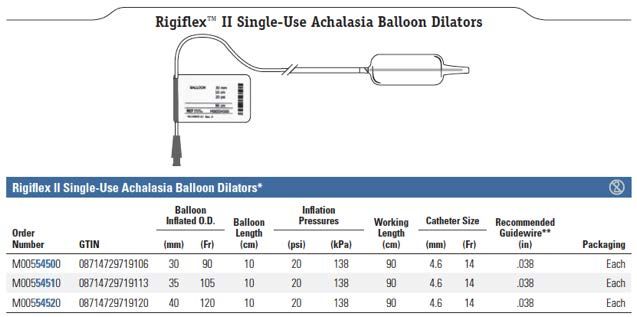
Achalasie: Karzinomrisiko
! Gratwanderung zwischen Adenokarzinom und
Plattenepithelkarzinom-Risiko
Plattenepithelca- Barrett und
Risiko gegenüber Adenoca-Risiko
Normalbevölkerung gegenüber
0 bis 140 fach Normalbevölkerung
erhöht erhöht
Georg Spaun, EndoLinz 1-2018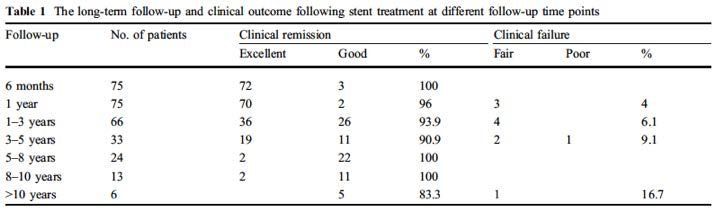
Achalasie: Eckardt Score Thomas Watson, World J Surg (2015) 39:1634–1641 Georg Spaun, EndoLinz 1-2018

Achalasie Therapie
! Heller’sche Myotomie
! offen
! laparoskopisch (LHM)
! thorakoskopisch
! endoskopisch (POEM)
! pneumatische Dilatation (PD)
! Botulinum Toxin Injektion
! Kurzzeit Stent Therapie
! Ösophagusresektion
Georg Spaun, EndoLinz 1-2018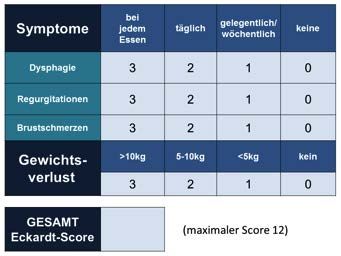
Achalasie: Ösophagusresektion
! Ösophagektomie subtotal mit Magenhochzug
! 101 pat. Follow-up:10.5 +/- 8.8 Jahre
! Ko alle 2 Jahre
! Barrett: 10.9% zwischen 1 und 5 Jahre
! 29.5% zwischen 5 und 10 Jahre
! 57.5% nach 10 oder mehr Jahren
! 5 Pat. entwickelten Ösophagusstumpfkarzinom
! 3 Plattenepithelca.
! 2 Adenoca.
Georg Spaun, EndoLinz 1-2018 deRocha et al; Ann Surg Oncol. 2008 Oct;15(10):2903-9.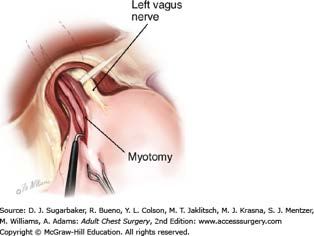
Achalasie Leitlinien
! keine österreichischen oder deutschen Leitlinien
! S.A.G.E.S (Society of the American Gastroenterologic Endoscopic
Surgeons):
! primäre Therapie für Pat. „fit for surgery“: laparoskopische
Heller Myotomie mit Dor Fundoplication
! Pneumatische Dilatation: höchstes Risiko für Komplikationen
! nur ausgewählte Pat: OP Verweigerer oder „poor operative
candidates“ (++++, strong)
Stefanidis D, Richardson W, Farrell TM, Kohn GP, Augenstein V, Fanelli RD, Society of American Gastrointestinal and Endoscopic Surgeons
(2012) SAGES guidelines for the surgical treatment of esophageal achalasia. SurgEndosc26:296–311 ; Vaezi MF, Pandolfino JE, Vela MF
(2013) ACG clinical guideline: diagnosis and management of achalasia.AmJGastroenterol 108:1238–1249Achalasie Leitlinien
! Stents:
! SAGES:
! „use of esophageal stents cannot be recommended for the
treatment of achalasia“ (++, strong)
! ACG (American College of Gastroenterology):
! Pneumatische Dilatation: alternative Methode neben LHM für
primäre Therapie
! beide Guidelines 7 und 5 Jahre alt
! POEM Statement vage gehalten
Stefanidis D, Richardson W, Farrell TM, Kohn GP, Augenstein V, Fanelli RD, Society of American Gastrointestinal and Endoscopic Surgeons
(2012) SAGES guidelines for the surgical treatment of esophageal achalasia. SurgEndosc26:296–311 ; Vaezi MF, Pandolfino JE, Vela MF
(2013) ACG clinical guideline: diagnosis and management of achalasia.AmJGastroenterol 108:1238–1249Achalasie: Botulinumtoxin
! prospektiv randomisierte Studie von Zaninotto 2004
! 80 Patienten: laparoskopische Myotomie vs Botox
! Myotomie besser (82% vs 66%,P < 0.05)
! 2 Jahres Daten: LHM: 87.5% Botox: 34%
! Conclusio: nur für Pat. unfit für Myotomie oder pneumatische
Dilatation
Zaninotto G, Annese V, Costantini M, Del Genio A, Costantino M, Epifani M, Gatto G, D’onofrio V, Benini L, Contini S, Molena D, Battaglia G,
Tardio B, Andriulli A, Ancona E. Randomized controlled trial of botulinum toxin versus laparoscopic hellermyotomy for esophageal achalasia.
Ann Surg 2004; 239: 364-370! 201 Patienten: randomisiert für Pneumatische
Dilatation (95 Pat.) oder LHM (106 Pat.)
! durchschnittliches Follow-up: 43 Monate
! intention-to-treat Analyse: kein signifikanter
Unterschied zwischen beiden Gruppen betreffend
„primary outcome“: (Eckardt score ≤3)
! Therapeutische Erfolgsrate:
! Pneumatische Dilatation: 90% nach 1 Jahr, 86% nach
2 Jahren
! LHM: 93% nach 1 Jahr, 90% nach 2 Jahren (P = 0.46)
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.! 2 Jahres Follow-up:
! kein signifikanter Unterschied:
! LES Druck: LHM: 10 mm Hg, PD: 12 mm Hg; P = 0.27
! Ösophagusentleerung, gemessen an der Barium Kontrast Säule:
LHM: 1.9 cm; PD: 3.7 cm; P = 0.21
! Lebensqualität
! per-protocol Analyse: Perforation: 4% PD; Mukosariss: 12% bei
LHM
! abnormale ösophageale Säureexposition: 15% PD and 23% LHM:
P = 0.28
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.! aber:
! Perforationsrate: 4 von 13 (30,8%)
ursprüngliches Protokoll: 35 mm ballon
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.! geändertes Protokoll: erste PD: 30 mm; 1 bis 3
Wochen später: 35 mm:
! Alle Patienten hatten daher mindestens 2
Dilatationen
! 4 Wochen später: (falls Eckardt > 3): dritte
Dilatation: 40-mm
! bei neuerlichen Symptomen während follow-up:
Dilatation wieder mit 35-mm und falls notwendig
40-mm Ballon
! 25% der PD Pat. hatten weitere Dilatation
während follow up
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.! aber:
! weitere 4 Perforationen: bei folgenden 96 Pat.
(Perforationsrate: 4,2%, 2 op, 2 gestentet)
! Literatur Perforationsrate: 2%-15%
! Mukosaeinrisse: 12% während LHM (intraop-
versorgt: vergleichbar mit Perforationen???)
! gesamt Perforationsrate 108 Pat. bei
Pneumatischer Dilatation: 7,4% (8,2%, 5y)
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.! alternative Botschaft dieses Artikels:
! 1 LHM ist deutlich effektiver als 1 PD
! PD hat höheres Perforationsrisiko als LHM
! PD hat ein 2% Risko für Notfall Ösophagus
Chirurgie
Georg Spaun, EndoLinz 1-2018 N Engl J Med 2011;364:1807-16.Achalasie: Pneumatische Dilatation
! Technik:
! Rigiflex Ballon (Boston Scientific)
! positioniert am ösophagogastrischen
Übergang
! dilatiert: mit 5 PSI für 1 min.
! gefolgt von 8 PSI für 1 min.
! Durchmesser: 30 mm
! 1 bis 3 Wochen später 35 mm
! wenn Eckhard Score ≤3: Therapieerfolg
! wenn nicht: 40 mm Dilatation
Georg Spaun, EndoLinz 1-2018Achalasie: Pneumatische Dilatation Georg Spaun, EndoLinz 1-2018
Achalasie: Pneumatische Dilatation
! zwei unterschiedliche Strategien:
! einzelne Dilatation vs stufenweise Dilatation
! stufenweise Dilatation: Symptomerleichterung: 50%–93% der
Pat.
! Therapieerfolg:
! einzelne PD: 62% nach 6 mo. und 28% nach 2 Jahren
! stufenweise PD: 90% nach 6 mo. und 44% nach 6 Jahren
! 1/3 der PD Pat: wieder Symptome nach 4–6 Jahren
Vela MF, Richter JE, Khandwala F, et al. The long-term efficacy of pneumatic dilatation and Heller myotomy for the treatment of achalasia.
Clin Gastroenterol Hepatol. 2006;4(5):580–587. Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of
achalasia. Am J Gastroenterol. 2013;108(8):1238–1249
Georg Spaun, EndoLinz 1-2018Achalasie: Pneumatische Dilatation
! prädiktive Faktoren für schlechtes klinisches Ansprechen:
! Alter < 45 Jahre
! männliche Pat
! dickere LES Muskulatur
! LES Druck nach Dilatation größer als 10–15 mmHg
! persistierende Symptome nach ein oder zwei
Behandlungen
Vela MF, Richter JE, Khandwala F, et al. The long-term efficacy of pneumatic dilatation and Heller myotomy for the treatment of achalasia.
Clin Gastroenterol Hepatol. 2006;4(5):580–587. Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of
achalasia. Am J Gastroenterol. 2013;108(8):1238–1249
Georg Spaun, EndoLinz 1-2018kann Myotomie mehr?
! Metaanalyse von Weber:
! 36 Studien:
! 3,211 Pat. PD Gruppe: 1,526 Pat. LHM Gruppe
! PD: durchschnittliche 5-Jahre Remissionsrate: 61.9% und 10-Jahre:
47.9%
! LHM: durchschnittliche 5-Jahre Remissionsrate: 76.1% und 10-Jahre
79.6%
! Perforationsrate: LHM: 4.8% vs PD 2.4%; P = 0.05
! (Perforationsrate POEM: < 1%)
! LHM deutlich bessere Langzeitergebnisse als PD
Georg Spaun, EndoLinz 1-2018 Weber CE et al. Surg Laparosc Endosc Percutan Tech. 2012;22(4):289–296.Heller Myotomy
! original Heller Myotomie:
! offene Operation
! anteriore und posteriore Myotomie
! keine Fundoplikation
! entscheidender Op Schritt: Myotomie der zirkulären Muskelfasern
! POEM ist genauso Heller Myotomie wie LHM
! aber: POEM RCT’s immer noch nicht publiziert
! Rösch: POEM vs LHM (ClinicalTrials.gov: NCT01601678)
! Boeckxstaens: POEM vs PD (ClinicalTrials.gov: NCT01793922)
Georg Spaun, EndoLinz 1-2018Georg Spaun, EndoLinz 1-2018 Inhoue et al. J Am Coll Surg 2015;221:256e 264.
Achalasie: POEM
! Efficacy of peroral endoscopic myotomy (POEM) in the
treatment of achalasia: a systematic review and meta-analysis
! Talukdar R, Inoue H, Nageshwar Reddy D
! 1,045 Pat. mit POEM in 29 Studien: 90 Pat mit POEM wurden mit
160 Pat mit LHM in 5 Studien verglichen
! keine Unterschiede: Eckardt's Score, post-operative Schmerz
Scores, Schmerzmittelbedarf, Spitalverweildauer, Komplikationen,
symptomatischer gastroösophagealer Reflux/Reflux Ösophagitis
! Operationszeit war signifikant kürzer für POEM
Georg Spaun, EndoLinz 1-2018 Surg Endosc. 2015 Nov;29(11):3030-46.Achalasie: POEM
! A comparative study on comprehensive, objective outcomes
of laparoscopic Heller myotomy with per-oral endoscopic
myotomy (POEM) for achalasia
! Bhayani NH, Kurian AA, Dunst CM, Sharata AM, Rieder E,
Swanstrom LL
! 101 Pat: 64 HM (42% Toupet und 58% Dor Fundoplikation) und 37
POEM
! ein-Monat Eckardt Score: signifikant besser für POEM (1.8 vs 0.8,
P < 0.0001)
! nach 6 Monaten: ähnliche Verbesserung der Eckardt Scores (1.7
vs 1.2, P = 0.1)
Georg Spaun, EndoLinz 1-2018 Ann Surg. 2014 Jun;259(6):1098-103Achalasie: POEM
! A comparative study on comprehensive, objective outcomes
of laparoscopic Heller myotomy with per-oral endoscopic
myotomy (POEM) for achalasia
! Beide Gruppen hatten signifikante Verbesserungen der
Postmyotomie LES Profile
! Postmyotomie Ruhedruck: höher für POEM als für HM (16 vs 7.1
mm Hg, P = 0.006)
! Postoperativ: 39% der POEM und 32% der HM abnormale Säure
Exposition (P = 0.7)
Georg Spaun, EndoLinz 1-2018 Ann Surg. 2014 Jun;259(6):1098-103Achalasie: POEM
! Per-Oral Endoscopic Myotomy: A Series of 500 Patients
! Haruhiro Inoue et al.
! Komplikationen: 3.2%
! signifikante Reduktion: Eckardt Score und LES Druck
! persistieren 3 Jahre nach POEM
! Gastroösophagealer Reflux: 21.3% bei 3-Jahres Follow-up
Georg Spaun, EndoLinz 1-2018 J Am Coll Surg 2015;221:256e 264.Achalasie: POEM
! Per-Oral Endoscopic Myotomy: A Series of 500 Patients
! drei-Jahres (und länger) Follow-up Daten: (Interviews) bei 61 von
105 Pat (58.1%)
! Manometrie und Endoskopie Daten für 16 (15.2%)
! Signifikante Symptom und LES Druck Reduktion
! Erfolgsrate: 88.5% (54 von 61)
! 21.3%: Sodbrennen oder Regurgitation; Ösophagitis bei 9 von 16
Pat. (56.3%)
! alle Pat: Reflux Symptome einfach mit intermittierenden PPI
beherrscht
Georg Spaun, EndoLinz 1-2018 J Am Coll Surg 2015;221:256e 264.Achalasie: Stents
! Temporary self-expanding metallic stents for achalasia: A
prospective study with a long-term follow-up
! Ying-Sheng Cheng, Fang Ma, Yong-Dong Li, Ni-Wei Chen, Wei-
Xiong Chen, Jun-Gong Zhao, Chun-Gen Wu
! 90 Achalasie Patienten: temporary SEMS (partially
covered)
! 20 mm ( n = 30, Gruppe A)
! 25 mm ( n = 30, Gruppe B)
! 30 mm ( n = 30, Gruppe C)
! Follow-up: 6 Monate und 1, 3-5, 5-8, 8-10 und > 10 Jahre
Georg Spaun, EndoLinz 1-2018 World J Gastroenterol 2010; 16(40): 5111-5117Achalasie: Stents
! Temporary self-expanding metallic stents for achalasia: A
prospective study with a long-term follow-up
! Brustschmerz: höher aber Stentmigration geringer in Gruppe C als in
Gruppen A und B
! Therapieversagerrate geringer in Gruppe C (13%) als in Gruppen A
(53%) und B (27%)
Georg Spaun, EndoLinz 1-2018 World J Gastroenterol 2010; 16(40): 5111-5117Achalasie: Stents Georg Spaun, EndoLinz 1-2018
Achalasie: Stents Clinical management of achalasia: current state of the art. Krill et al. Clinical and Experimental Gastroenterology 2016:9 71–82 Georg Spaun, EndoLinz 1-2018
Achalasie: Stents Georg Spaun, EndoLinz 1-2018
Stent vs Pneumatische Dilatation
! Comparison of temporary stent insertion with pneumatic dilation
of the same diameter in the treatment of achalasia patients: a
retrospective study.
! SEMS vs PD
! Schmerzen: 42.9% vs 23.6% und Blutung: 15.9% vs 8%
! teilweise beschichteter SEMS
! Durchmesser: Ballon oder Stent: 30 mm
! Stent Entfernung < 7 d
! Follow up: klinisch und manometrisch > 10 Jahre
Zhu YQ, Cheng YS, Tang GY, Li MH, Zhao JG, Li F. J Gastroenterol Hepatol 2010; 25: 499-505
Georg Spaun, EndoLinz 1-2018Stent vs Pneumatische Dilatation
! Perforationsrisiko:
! PD: 2-15%
! 15 Stents für 100 Pat
! primärer Stent:
! 100 Stents für 100 Pat
! + 68.000 € primärer
Stent / 100 pat.
! aber: - 15 Perf.
! Blutungen und
Schmerzen verdoppelt
Georg Spaun, EndoLinz 1-2018POEM eigene Daten
! 2014 bis jetzt 21 Pat. POEM operiert und nachkontrolliert
! 19 Pat sehr zufrieden Eckhardt Score: 0 bis 1 (90,4%)
! 2 Pat Therapieversager: Eckhardt Score > 3 (9,5%)
! 2 minor Komplikationen (9,5%)
! 1 Hämatom unter Marcoumar: konservativ
! 1 Ulcus an Ora serrata: passagerer Stent und AB
! beide Pat. trotzdem sehr zufrieden mit Ergebnis
! keine maior Komplikationen
Georg Spaun, EndoLinz 1-2018Zusammenfassung
! Heller Myotomie effektivste Therapie für idiopathische Achalasie
! POEM ist ebenso Heller Myotomie wie LHM
! PD und LHM haben höheres Perforationsrisiko als POEM
! Heller Myotomie ist erste Wahl für alle Patienten „fit for surgery“,
speziell für Patienten < 45 Jahre
! 30 mm Kurzzeit Stents eventuell so effektiv wie PD
! Vergleichende randomisierte Studien werden benötigt und sind
unterwegs
! Achalasie ist eine seltene Erkrankung und sollte in
spezialisierten Zentren behandelt werden
! regelmäßige Gastroskopiekontrolle mit PE’s
Georg Spaun, EndoLinz 1-2018Sie können auch lesen