Chronische lymphatische Leukämie - Lymphome.ch
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

WORLD LYMPHOMA AWARENESS DAY
Chronische lymphatische Leukämie
CLL 18.09.2021 09.50 – 14.45 Uhr
wir informieren, sensibilisieren, beraten, begleiten, vernetzen!
WLAD 2021
LIVE-
WEBINAR
Jörg Halter Vorträge und Workshops
Moderation: Marianne Erdin
Prof. Dr. med. Stephan Dirnhofer
Prof. Dr. med. Urban Novak
Hämatologie Dr. med. Michèle Voegeli
PD Dr. med. Jörg Halter
Prof. Dr. med. Andreas Lohri
Prof. Dr. med. Christoph Mamot
Universitätsspital Basel Das Programm richtet sich an
Erwachsene mit Lymphomen,
Prof. Dr. med. Emmanuella Guenova PhD
PD Dr. med. Christoph Berger
Dr. med. Christiane Jenemann
Prof. Dr. med. Claudia Witt
Angehörige und Interessierte! Claudia Russo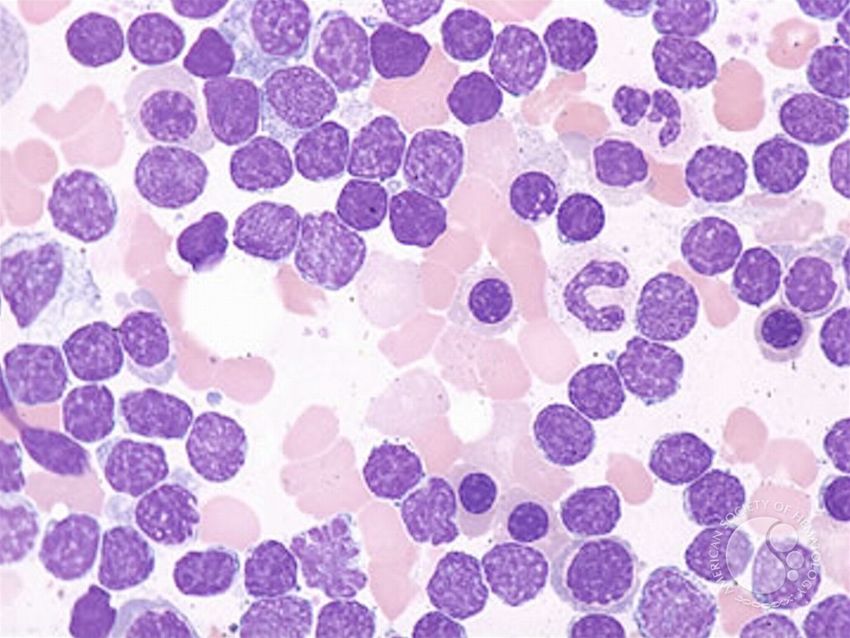
In allen Altersgruppen liegt sowohl die Erkrankungswahrscheinlichkeit (Rate) a
lute Zahl an Neuerkrankungen über der der Frauen. Mit zunehmendem Alte
Unterschied zwischen den Geschlechtern. Die Mortalität folgt diesem Muster
Niveau. Einziger Unterschied ist die Zahl der Sterbefälle in der Altersgruppe 8
Hier liegt die absolute Zahl bei den Frauen höher als bei den Männern. Das is
fisch determiniert.
CLL - Epidemiologie
Häufigste leukämische Erkrankung in
Mitteleuropa
Pro Jahr ca.
5-6/100‘000 Männer
2.5-4/100‘000 Frauen
→ mehr Männer betroffen (1.7:1)
Mittleres Erkrankungsalter 70-75 Jahre
→ grosse Spannweite
Legende:
Quelle: Gesellschaft der epidemiologischen Krebsregister in Deutschland e.V., Sonderauswertung
Onkopedia, 15.09.21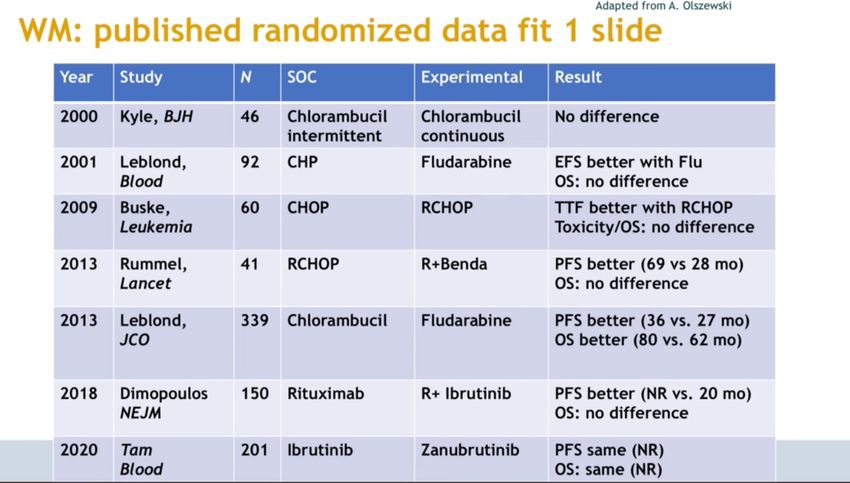
CLL Charakteristika - Sehr heterogen (klinisch, biologisch) - Reifzellige B-Zell-Neoplasie mit (CLL) / ohne (SLL,
Gumprecht‘sche Schollen
CLL Charakteristika
Vermehrung von Lymphozyten in Blut, Lymphknoten, Milz und Knochenmark
- abnorme Lymphozyten, welche normale Aufgabe nicht mehr erfüllen
- Wachstum von Lymphknoten und andere Organe wie Leber und Milz
- Akkumulation führt zu:
- Verminderung der Produktion von gesunden Blutzellen (rote
Blutkörperchen, weisse Abwehrzellen, Blutplättchen
- Funktionseinschränkung des Immunsystems
Langsam fortschreitende / sich entwickelnde Krankheit
- Meist keine oder nur geringe Probleme in Frühstadien
- z.T. nie behandlungsbedürftig oder erst nach vielen Jahren (frühe Behandlung
ohne Vorteil)
- Diagnose häufig Zufallsbefund wegen Blutuntersuchung aus anderen Gründen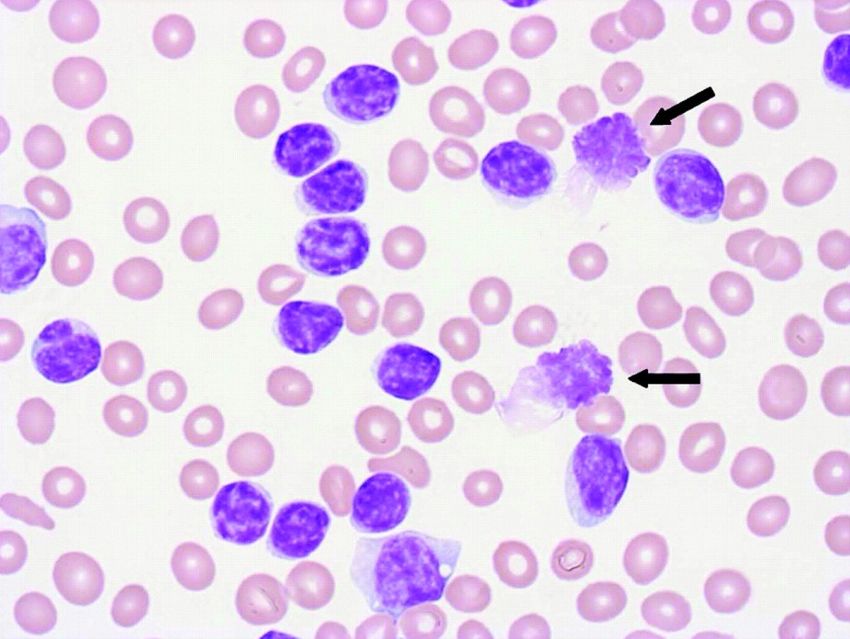
Symptome/Beschwerden durch CLL Zum Zeitpunkt Diagnose meiste Patienten ohne Symptome oder Zeichen der CLL Häufigste Symptome: - Schmerzlose Lymphknotenvergrösserung (Hals, Achselhöhle, Leisten) - Nur bei 5-10% finden sich bei Erstdiagnose: - Müdigkeit mit Einschränkung im Alltag/Beruf - Ungewollter Gewichtsverlust ≥10% Körpergewicht in letzten 6 Monaten - Fieber ≥38°C mit oder ohne Infekte - Nachtschweiss

Lymphknotenstationen
Copyrights apply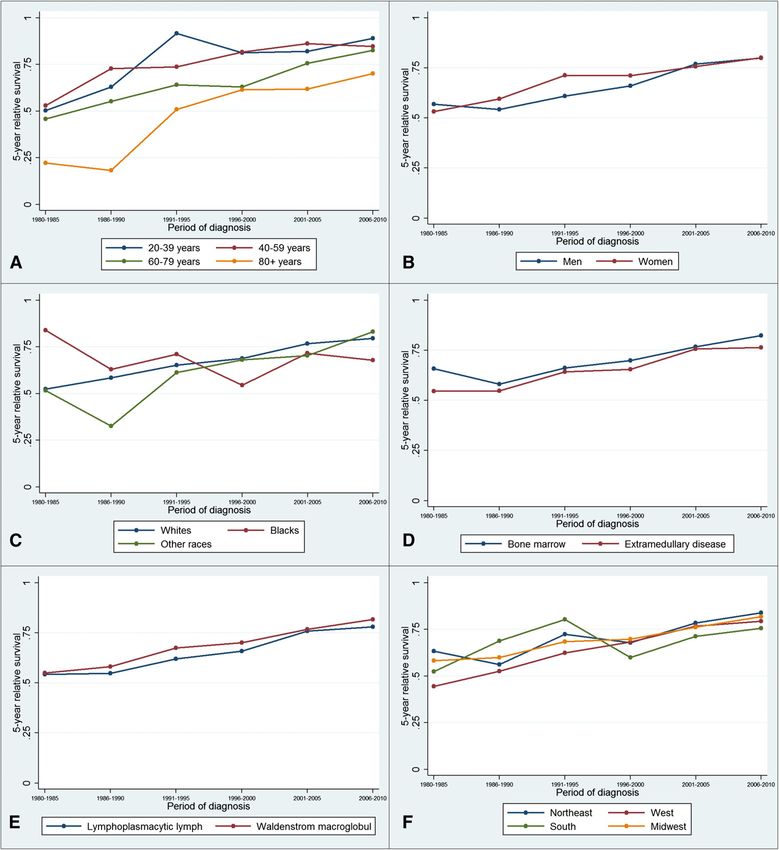
Staging (Stadieneinteilung) der CLL Krankheitsverlauf individuell extrem variabel, Dauer 2 – 20+ Jahre Abschätzung Prognose: - Staging (Standortbestimmung) nach RAI oder BINET - Basis: Blutwerte und körperlicher Untersuchung (Lymphknoten, Milz, Leber) - Resultat: Krankheitsausdehnung im Körper → erlaubt Abschätzung wie schnell oder langsam der weitere Krankheitsverlauf sein wird → Abschätzung Zeitpunkt Therapiebeginn Prädiktive Marker: - Erlauben Vorhersage, mit welcher Wahrscheinlichkeit die CLL auf eine bestimmte Behandlung ansprechen wird → Therapiewahl

Official reprint from UpToDate® www.uptodate.com
©2017 UpToDate®
Survival curves of chronic lymphocytic leukemia (CLL) by Rai
and Binet stage
Staging Systeme: Rai oder Binet
RAI
Prognost. Bedeutung bleibt,
Risiko Stadium Kriterien aber Lebenserwartung mit
low 0 Lymphozytose in PB od. KM neuen Therapien heute
intermediate I Lymphozytose + Lymphadenopathie deutlich besser!
II Lymphozytose + Hepato- od. Splenomegalie +/-
Lymphadenopathie
high III Lymphozytose + Anämie (
Prädiktive Marker → Mitentscheidend für Therapiewahl Genetische und molekulare Untersuchungen - Zytogenetik: - fehlende Chromosomenteile: del(17p), del(11q), del(13q), Trisomie 12 - Molekular: - TP53 Mutation - IGHV Mutationsstatus fett: wichtigste krankheitsassoziierte Marker für Therapiewahl
The US Department of Veterans Affairs has accepted blood transfusion
that exposure to Agent Orange is a risk factor for CLL, suggests that dieta
which has enabled veterans with CLL to claim benefits the risk of CLL.
if they were previously exposed to Agent Orange while
in military service33. In addition, evidence suggests that Mechanisms/pat
From www.bloodjournal.org by guest on June 27, 2017. For personal use only.
exposure to insecticides might be a risk factor for CLL34. Genetics
By contrast, little evidence indicates that ionizing radi- Genetic alteration
Del(17p), TP53, IGHV ation can increase the risk of CLL35,36. Furthermore, there
is scant evidence that viral infections are risk factors, and
alterations, mutat
miRNAs and epige
17p D ELE TIO N IN M Y EL O D Y SPL A S TIC S Y N DR O M E S 1013 Chromosomal al
F E AT U R E S
patients with CLL
RESCUING THEdeletion generally have complex karyotypes, with unidentified Dark Light chromosomal alte
GUARDIAN
OF THE GENOME
chromosome markers that could contain 17p material, and also
because the chromosomal segment translocated on 17p some-
times cannot be identified.6,19
13q14.3 (del(13q)
(REF. 38). Del(13q)
alteration, eviden
Downloaded from http://science.sciencemag.org/ on February 19, 2021
New drugs combat cancer by propping up
a mutated tumor-fighting protein In the patients where conventional cytogenetics suggested ated with favoura
Apoptosis
By Robert F. Service
unbalanced t(5;17), t(12;17), t(17;18), or t(17;21) translocation region is the DLE
leading to 17p deletion, WCP confirmed the Proliferation
translocation lates the expressio
CD5+ and SHM tosis or that are i
between chromosome 17 and chromosome B cell 5, 12, 18, and 21,
From www.bloodjournal.org by guest on June 27, 2017. For personal use only. FDC
(see Supplementar
respectively. WCP also confirmed conventional cytogenetic
found in 7% of pat
findings in one patient with monosomy 17. However, combina-
tumour suppressor
tion of WCP and FISH analysis 1013 with centromeric probes for TH
17p D ELE TIO N IN M Y EL O D Y SPL A S TIC S Y N DR O M E S
is found in 18% of
chromosome 17 and partner chromosomes modified the interpre- cell
alterations in ATM
Deletion 17p deletiontation
generallyof have complex karyotypes,
cytogenetic datawith in aunidentified
chromosome markers that could contain 17p material, and also
few cases. In particular, one of the SHM?
in DNA repair); ea
because patients thought totranslocated
have t(12;17) by conventional cytogenetics
the chromosomal segment on 17p some-
is associated with
Published by AAAS
2
times cannot be identified.6,19
was shown to have dic(12;17), one patient classified as i(17q)
In the patients where conventional cytogenetics suggested
Class
this has improved
switching
by conventional cytogenetics was
unbalanced t(5;17), t(12;17), t(17;18), or t(17;21) translocation shown to have idic(17)(p11), in 16% of patients
leading to 17p deletion, WCP confirmed the translocation
and one patient classified as der(17)t(5;17) was reclassified as
between chromosome 17 and chromosome 5, 12, 18, and 21, intermediate prog
der(5)t(5;17).
respectively. WCP also confirmed conventional cytogenetic
mantle cell lympho
findings in one patient with monosomy 17. However, combina-
In the three cases where the chromosome segment translo- Class- location t(11;14)(q
tion of WCP and FISH analysis with centromeric probes for IgM+IgD+ switched
chromosome cated to partner
17 and 17p could notmodified
chromosomes be identified
the interpre-by conventional cytogenet- memory that enhance the e
memory
tation of cytogenetic data in a few cases. In particular, one of the
ics, WCP showed that it corresponded to chromosome 22q B cell
patients thought to have t(12;17) by conventional cytogenetics B cell the cell cycle regul
was shown material in one one
to have dic(12;17), case (no.
patient 13).asIni(17q)
classified another patient (no. 14), the
by conventional cytogenetics was shown to have idic(17)(p11),
partner chromosome could not be identified, but it was not
and one patient classified as der(17)t(5;17) was reclassified as Somatic mutation
chromosome 5, 7, 12, 18, 21, or 22. In the last case (no. 15), only
der(5)t(5;17). sequencing and
In the three cases where the chromosome segment translo-
chromosome 5 could be analyzed by WCP, ruling out t(5;17).
cated to 17p could not be identified by conventional cytogenet- sequencing to CLL
ics, WCP showed WCPthat andit corresponded
FISH analysis showed
to chromosome IGHV-unmutated
22q that in two cases ofCLL with limited SHM
t(5;17) IGHV-mutated IGHV-mutated of the genetic heter
material in one case (no. 13). In another patient (no. 14), theIgM+IgD+ CLL (e.g. IGHV3-12/IGLV3-21) IgM+IgD+ CLL Ig+ CLL
Fig 4. Extent of 17p deletion analyzed by FISH using 5 markerspartner (patients chromosome no. could8not andbe 9), no 17p
identified, material
but it was not appeared to be deleted. In that CLL harbours
spanning 17p and a chromosome 17 centromeric probe (D17Z1) in thechromosome those 5, 7, two
12, 18, cases,
21, or 22. WCP
In the lastshowed Figure 1 | Cellular
case (no. 15),chromosome
only originson
17 material of CLL
a cells. Nature Reviews | Disease Primers (FIG. 2). From these
14 patients with confirmed 17p deletion. The deletion involved thechromosome
WCP marker
5 could be analyzed by WCP, ruling out t(5;17).
chromosome
and FISH analysis showed that and
in twoacases
ring unmutiert
chromosome, respectively. The
of t(5;17)
mutiert have been consist
p53 gene in all cases except one, but this patient (patient no. 13) had(patients no. 8 and 9), no 17p material appeared to be deleted. In
20
+
also monosomy 17,
Fig 4. Extent of 17p deletion analyzed by FISH using 5 markers
and therefore loss of one p53 allele.
presence of two copies of all 17p markers studied, including role in DNA dam
spanning 17p and 1998;91:1008
a chromosome 17 centromeric probe The
(D17Z1)proximal
in the those two cases, WCP showed chromosome 17 material on a
Soenen V et
breakpoint was al.inBlood
Soenen
17q in 1998;91:1008
V et al. Blood
3 with
14 patients patients,
confirmedas 17pshown by deletion
deletion. The deletion of D17Z1
involved the p53, wasand
marker chromosome confirmed in both
a ring chromosome, patients
respectively. The by FISH analysis. None of mRNA
Kipps TJ et al. Nat Rev Dis Primers processin
2017;3:1
p53 gene in all cases except one, but this patient (patient no. 13) had
probe, and located alsoin monosomy
17q11 by conventional
17, and therefore loss of one cytogenetic analysis.presencethose
p53 allele. The proximal two ofpatients
of two copies hadstudied,
all 17p markers typical dysgranulopoiesis, and p53
including chromatin modi
D17Z1 notp53, was confirmed in both patients by FISH analysis. None of
(FISH results in patients
breakpointno.was 8
in and
17q in 39,patients,
where 17p by
as shown deletion
deletion of was
probe, and located in 17q11 by conventional cytogenetic analysis. those two mutation
patients had was notdysgranulopoiesis,
typical found in the and assessable
p53 case. By contrast, CHD2 and ZMYM
confirmed, are excluded frominthis
(FISH results figure).
patients no. 8 and 9, where 17p deletion was not mutationWCP was notand ling (for example,
confirmed, are excluded from this figure).
FISH
found in the analysis confirmed
assessable case. By contrast, 17p deletion and loss of one
WCP and FISH analysis confirmed 17p deletion and loss of one
p53 allele p53in theallele
remainingin patients.
the remaining
All had typical patients. regions
dysgranulo- All had of the heavy
typical chain (IGHV
dysgranulo- IGVL ways (for example
studied for p53. The remaining two patients (no. 8 and 9) had no poiesis,
poiesis, and and
all but one all
of the but one
assessable of
cases the
had p53assessable
mutation cases had p53 mutation those found in EG
studied for p53. The remaining two patients (no. 8 and 9) had noand/or overexpression (which in our experience is synonymous
dysgranulopoiesis and, as seen before, no 17p deletion by FISHWer sollte behandelt werden? - Viele CLL-Patienten benötigen über Jahre oder gar nie keine Behandlung - Frühtherapie ohne Symptome bringt keinen Vorteil bezüglich Prognose - In der Regel kann keine Heilung der CLL erreicht werden → Grund, Behandlung zu starten: CLL verursacht Komplikationen
Start Behandlung bei: - Verminderung von normale weissen Blutkörperchen (Neutrophilen) → Infektneigung - Ausgeprägte Vergrösserung von Lymphknoten oder Milz - Zunahme der Lymphozytenzahl (Lymphozytenverdoppelungszeit < 6 Monate v.a. ab Lymphozyten >30G/L oder Zunahme >50% über 2 Monate) - Ausbreitung der CLL in andere Organe (Haut, Niere, Lunge, Wirbelsäule etc.) - Krankheitsbedingte Beschwerden wie - Schwere Müdigkeit/Abgeschlagenheit - Nachtschweiss ≥ 1 Monat - Ungewollter Gewichtsverlust ≥10% - Fieber - Autoimmunhämolytische Anämie (Immunsystem zerstört rote Blutkörperchen) - Immunthrombozytopenie (Immunsystem zerstört Blutplättchen) → ohne genügende Antwort auf übliche Therapie
Erstlinienbehandlung
Verursacht CLL
Komplikationen?
Nein, ja
asymptomatisch
watch & wait: Therapie notwendig
1. Jahr: Kontrolle und Blutbild → Körperliche Verfassung? (Alter)
alle 3 Monate → andere Medikamente?
Ab 2. Jahr: evtl. Ausdehnung → genet. Eigenschaften der CLL
der Intervalle wenn stabilErstlinientherapie (USB 05/21)
First – line therapy
asymptomatic symptomatic
all
fit unfit frail
(go go) (slow go) (no go)
w&w
without with
del (17p13) del (17p13)
without with or BSC 4
or
del (17p13) del (17p13) TP53mut 2 TP53mut 2
or or
TP53mut 2 TP53mut 2
IGHV IGHV
unmutated mutated
≤ 65 years > 65 years Ibrutinib
Ibrutinib Ibrutinib Clb-Obi Ibrutinib
IGHV IGHV IGHV IGHV
unmutated mutated unmutated mutated or or
or or Clb-Obi B*R CR/PR SD/PD
Ibrutinib Ibrutinib FCR Ibrutinib Ibrutinib BR
or
or or Continuous Second line
FCR BR B*R therapy therapy
CR/PR SD/PD CR/PR SD/PD CR/PR SD/PD
Continuous Second line Continuous Second line Continuous Second line
therapy# therapy therapy therapy therapy# therapy
or or
Observation # Observation #
Legend:
w & w watch & wait, B - bendamustin , BSC - best supportive care, - cyclophosphamid, Clb - chlorambucil, F - fludarabin, Obi - obinutuzumab, Ofa - ofatumumab, R -
rituximab, CR - complete remission, PD - progress, PR partial remission, SD stable disease. *Dosage reduction of bendamustin to 70mg/m2 (day 1+2) in patients with
reduced performance status (slow go); #continuous therapy with ibrutinib, observation with chemotherapyErstlinientherapie (USB 05/21)
First – line therapy
asymptomatic symptomatic
all
fit unfit frail Therapietoleranz
(go go) (slow go) (no go) Therapieintensität
w&w
without with
del (17p13) del (17p13)
without with or BSC 4
or
del (17p13) del (17p13) TP53mut 2 TP53mut 2
or or
TP53mut 2 TP53mut 2
IGHV IGHV
unmutated mutated
≤ 65 years > 65 years Ibrutinib
Ibrutinib Ibrutinib Clb-Obi Ibrutinib
IGHV IGHV IGHV IGHV
unmutated mutated unmutated mutated or or
or or Clb-Obi B*R CR/PR SD/PD
Ibrutinib Ibrutinib FCR Ibrutinib Ibrutinib BR
or
or or Continuous Second line
FCR BR B*R therapy therapy
CR/PR SD/PD CR/PR SD/PD CR/PR SD/PD
Continuous Second line Continuous Second line Continuous Second line
therapy# therapy therapy therapy therapy# therapy
or or
Observation # Observation #
Legend:
w & w watch & wait, B - bendamustin , BSC - best supportive care, - cyclophosphamid, Clb - chlorambucil, F - fludarabin, Obi - obinutuzumab, Ofa - ofatumumab, R -
rituximab, CR - complete remission, PD - progress, PR partial remission, SD stable disease. *Dosage reduction of bendamustin to 70mg/m2 (day 1+2) in patients with
reduced performance status (slow go); #continuous therapy with ibrutinib, observation with chemotherapyErstlinientherapie (USB 05/21)
First – line therapy
asymptomatic symptomatic
all
fit unfit frail Therapietoleranz
(go go) (slow go) (no go) Therapieintensität
w&w
without with
del (17p13) del (17p13)
without with or BSC 4
or
del (17p13) del (17p13) TP53mut 2 TP53mut 2
or or
TP53mut 2 TP53mut 2 Genetik CLL
IGHV IGHV
unmutated mutated
≤ 65 years > 65 years Ibrutinib
Ibrutinib Ibrutinib Clb-Obi Ibrutinib
IGHV IGHV IGHV IGHV
unmutated mutated unmutated mutated or or
or or Clb-Obi B*R CR/PR SD/PD
Ibrutinib Ibrutinib FCR Ibrutinib Ibrutinib BR
or
or or Continuous Second line
FCR BR B*R therapy therapy
CR/PR SD/PD CR/PR SD/PD CR/PR SD/PD
Continuous Second line Continuous Second line Continuous Second line
therapy# therapy therapy therapy therapy# therapy
or or
Observation # Observation #
Legend:
w & w watch & wait, B - bendamustin , BSC - best supportive care, - cyclophosphamid, Clb - chlorambucil, F - fludarabin, Obi - obinutuzumab, Ofa - ofatumumab, R -
rituximab, CR - complete remission, PD - progress, PR partial remission, SD stable disease. *Dosage reduction of bendamustin to 70mg/m2 (day 1+2) in patients with
reduced performance status (slow go); #continuous therapy with ibrutinib, observation with chemotherapyErstlinientherapie (USB 05/21)
First – line therapy
asymptomatic symptomatic
all
fit unfit frail
(go go) (slow go) (no go)
w&w
without with
del (17p13) del (17p13)
without with or BSC 4
or
del (17p13) del (17p13) TP53mut 2 TP53mut 2
or or
TP53mut 2 TP53mut 2
IGHV IGHV
unmutated mutated
≤ 65 years > 65 years Ibrutinib
Ibrutinib Ibrutinib Clb-Obi Ibrutinib Ibrutinib
IGHV IGHV IGHV IGHV
or IMBRUVICAÒ
unmutated mutated unmutated mutated or
or or Clb-Obi B*R CR/PR SD/PD
Ibrutinib Ibrutinib FCR Ibrutinib Ibrutinib BR
or
or or Continuous Second line
FCR BR B*R therapy therapy
CR/PR SD/PD CR/PR SD/PD CR/PR SD/PD
Continuous Second line Continuous Second line Continuous Second line
therapy# therapy therapy therapy therapy# therapy
or or
Observation # Observation #
Legend:
w & w watch & wait, B - bendamustin , BSC - best supportive care, - cyclophosphamid, Clb - chlorambucil, F - fludarabin, Obi - obinutuzumab, Ofa - ofatumumab, R -
rituximab, CR - complete remission, PD - progress, PR partial remission, SD stable disease. *Dosage reduction of bendamustin to 70mg/m2 (day 1+2) in patients with
reduced performance status (slow go); #continuous therapy with ibrutinib, observation with chemotherapyErstlinientherapie (USB 05/21)
First – line therapy
asymptomatic symptomatic
all
fit unfit frail
(go go) (slow go) (no go)
w&w
without with
del (17p13) del (17p13)
without with or BSC 4
or
del (17p13) del (17p13) TP53mut 2 TP53mut 2
or or
TP53mut 2 TP53mut 2
IGHV IGHV
unmutated mutated
≤ 65 years > 65 years Ibrutinib
Ibrutinib Ibrutinib Clb-Obi Ibrutinib Ibrutinib
IGHV IGHV IGHV IGHV
or IMBRUVICAÒ
unmutated mutated unmutated mutated or
or or Clb-Obi B*R CR/PR SD/PD
Ibrutinib Ibrutinib FCR Ibrutinib Ibrutinib BR
or Immun-
or or Continuous Second line
FCR BR B*R therapy therapy Chemotherapie
Antikörper + X
CR/PR SD/PD CR/PR SD/PD CR/PR SD/PD Rituximab
(Mabthera Ò,
Continuous Second line Continuous Second line Continuous Second line
Rixathon Ò,
therapy# therapy therapy therapy therapy# therapy Truxima Ò)
or or Obinutuzumab
Observation #
(GazyvaroÒ)
Observation #
Legend:
w & w watch & wait, B - bendamustin , BSC - best supportive care, - cyclophosphamid, Clb - chlorambucil, F - fludarabin, Obi - obinutuzumab, Ofa - ofatumumab, R -
rituximab, CR - complete remission, PD - progress, PR partial remission, SD stable disease. *Dosage reduction of bendamustin to 70mg/m2 (day 1+2) in patients with
reduced performance status (slow go); #continuous therapy with ibrutinib, observation with chemotherapyA PROSPECTIVE, RANDOMIZED, OPEN-LABEL, MULTICENTRE PHASE-III TRIAL OF
IBRUTINIB VERSUS VENETOCLAX PLUS OBINUTUZUMAB VERSUS IBRUTINIB PLUS
VENETOCLAX FOR PATIENTS WITH PREVIOUSLY UNTREATED CHRONIC LYMPHOCYTIC
LEUKAEMIA
TREATMENT SCHEDULE
TIMELINES
Start of recruitment Q1/2021
Expected end of recruitment Q4/2023
End of study Q1/2027
897 patients
Primary endpoint:
Progression-free survivalZweitlinientherapie: wann? Intoleranz/Nebenwirkungen der Erstlinientherapie Bsp: Imbruvica-Unverträglichkeit Mögliche Massnahmen vor Wechsel: - Dosisreduktion - Symptomatische Therapie - Paracetamol gegen Muskel-/Gelenk- oder Kopfschmerzen - Loperamid gegen Durchfall - Blutdrucksenker evtl. Wechsel auf anderen BTK-Inhibitor (Acalabrutinib) oder Venetoclax
Zweitlinientherapie: wann? Rückfall (Rezidiv) oder Progression - Zunahme der Lymphozytenzahl - Wachstum von Lymphknoten, Milz oder zunehmende Verminderung der Blutwerte - Transformation in aggressiveres Stadium (Richter-Syndrom) → falls noch unter Therapie: evtl. Fortsetzung solange noch wirksam – engere Kontrollen abhängig von Krankheitsentwicklung → Zweitlinientherapie
Zweitlinientherapie (USB 05/21)
Second – line therapy fit unfit frail
(go go) (slow go) (no go)
Therapietoleranz
Therapieintensität
without with
del (17p13) del (17p13) Genetik CLL
or or
TP53mut TP53mut
Vorbehandlung?
after without
Ibrutinib Ibrutinib
pre-therapy
PD Late relapse
or Abstand zu letzter
or
early relapse
Therapie?
or or
Venetoclax + Ibrutinib Venetoclax + Repeat primary Ibrutinib Venetoclax + BSC
Rituximab Rituximab therapy Rituximab Venetoclax
(Venclyxto Ò)
+
CR/PR SD/PD SD/PD CR/PR SD/PD
Antikörper
or
or
allo SZT 1,6 Maintenance 3d line 3d line allo SZT 1,6 Maintenance 3d line
therapy therapy therapy therapy therapy
Legend: PD – progress, SD – stable disease, CR – complete remission, PR – partial remission, early relapse – within 2-3 years, late relapse – after 2-3
years, allo SZT – allogeneic stem cell transplantation, BSC – Best Supportive CareMedikamentöse Behandlung der fortgeschrittenen oder symptomatischen CLL Zielgerichtete Therapie / targeted therapy Meistens erste Wahl – Medikamente beeinflussen spezifische Typen von Tumorzellen - BTK Inhibitoren: - Ibrutinib, Acalabrutinib - BCL-2 Inhibitor - Venetoclax - PI3K Inhibitoren - Idelalisib - Duvelisib Alles Tabletten Evtl. Kombination mit Immuntherapie ? Jedes Medikament mit anderem Nebenwirkungsprofil
Medikamentöse Behandlung der fortgeschrittenen oder symptomatischen CLL
Chemoimmuntherapie: Mögliche Erstlinienbehandlung falls CLL gewisse genetische
Charakteristika aufweist
Kombination von:
- Chemotherapie
- Substanzen, welche das Wachstum von Tumorzellen verlangsamen oder stoppen
- Wirken auf Zellen, welche sich teilen und vermehren – Knochenmark, Haarwurzeln,
Magendarm
- Fludarabin
- Cyclophosphamid
- Bendamustin
- Chlorambucil
Infusion oder Tabletten je nach Medikament
Therapiedauer definiert, danach therapiefreie Periode bis zum erneuten Fortschreiten der CLLIbrutinib
Filmtabletten, 1xtägliche Einnahme mit Wasser
nicht auf vollkommen nüchternen Magen
Wechselwirkungen mit anderen Medikamenten vor Therapiebeginn prüfen
Erhöht Blutungsneigung (Verminderung der Plättchenfunktion) → 3-7 Tage vor
Ibrutinib-induced lymphocytosis in CLL
SEM Herman et al
und nach chirurg. Eingriff absetzen 2190
200
Herzrhythmusstörungen (Vorhofflimmern, andere Rhythmusstörungen) 150
ALC (103/! L)
Hoher Blutdruck 100
50
Bei Therapiebeginn innerhalb von 24h Anstieg (!) der Lymphozytenzahl –
0
Spitzenwert nach 1-2Montaen, dann langsames Sinken der Werte innerhalb 0 60 120 180
Day on study
von ca. 6-8 Monaten
100
Optimale Therapiedauer? In der Regel Dauertherapie bis CLL progredient
80
% of patients with
oder nicht-akzeptable Nebenwirkungen
peak ALC
60
40
20
0
0 10 20 30 40 50 60 70 80 90 100
Day on study
Figure 1. Ibrutinib-induced lymphocytosis develops rapidly, peaks w
patients with complete counts for the first 6 months on ibrutinib are dVenetoclax
Filmtablette, 1x tägliche Einnahme
Wechselwirkungen mit anderen Medikamenten – evtl. Dosis
anpassen
Therapie langsam einschleichen um schnellen massiven Zellzerfall Woche Tagesdosis Venetoclax
zu verhindern (Tumorlyse-Syndrom) 1 20 mg
2 50 mg
Nebenwirkungen
Blutbildveränderungen: Verminderung der gesunden weissen 3 100 mg
Blutkörperchen (Neutrophile Granulozyten) ->> Infektgefahr 4 200 mg
5 400 mg
In CH nicht zugelassen für Erstlinientherapie, dennoch evaluieren,
va. Begleiterkrankungen (Blutungsneigung,Herzkrankheiten) oder
Unverträglichkeit mit Medikamenten (Blutverdünner)
In der Regel kombiniert mit Antikörperinfusion
– Therapiedauer 12 Mte (bei Erstlinientherapie)Immunchemotherapie Antikörperinfusion + Chemotherapeutikum (evtl. in Zukunft vermehrt auch subcutan) Immuntherapie - Antikörperpräparate – zielen gegen spezifische Oberflächeneigenschaften auf Zellen (Tumorzellen): Rituximab, Obinutuzumab, Ofatumumab - Alle als Infusion verabreicht – zielen gegen B-Lymphozyten - Wenn als Erstlinientherapie verabreicht dann in Kombination mit einem oder mehreren Chemotherapeutika Nebenwirkungen: - Infusionsreaktionen (1.Gabe) - Hepatitis B-Reaktivierung (ohne Prophylaxe) - Infekte
Acalabrutinib Ähnliche Wirksamkeit wie Ibrutinib Insgesamt weniger Nebenwirkungen Zulassung CH: CLL (Monotherapie) Als Monotherapie zur Behandlung erwachsener Patienten mit unbehandelter chronischer lymphatischer Leukämie (CLL) mit 17p-Deletion oder TP53-Mutation: - die 65 Jahre und älter sind ODER - die 18-64 Jahre sind und Begleiterkrankungen haben 2L+ CLL (Monotherapie) Als Monotherapie zur Behandlung erwachsener Patienten mit CLL, die mindestens eine Vortherapie erhalten haben. Acalabrutinib wird jedoch nicht bei Patienten vergütet, bei denen unter Ibrutinib eine Krankheitsprogression auftrat.
Therapie von rezidivierter oder refraktärer CLL Meiste CLL-Patienten sprechen auf Erstlinientherapie an Selbst wenn komplette Remission kommt es im Verlauf oft zu Rückfällen (Rezidiv) oder die CLL spricht nicht genügend auf die Therapie an (refraktär) Optionen: Zielgerichtete Therapien (targeted therapy) Wechsel auf andere Substanz: - Ibrutinib – Venetoclax – Acalabrutinib - Idelalisib (Zydelig) - Duvelisib - Evtl. Kombination mit Immunotherapie Chemoimmunotherapie selten(er) indiziert Blutstammzelltransplantation für junge Patienten mit aggressiver Krankheit
Behandlung von CLL-Komplikationen
Häufigste Komplikationen:
- Verminderte Blutwerte
Anämie
Häufig → verminderte Sauerstofftransportkapazität: Müdigkeit, Schwäche, evtl. Brustschmerzen
Evtl. Notwendigkeit für Bluttransfusionen
Tiefe Blutplättchen (Thrombozytopenie)
vermehrten Verbrauch und/oder verminderte Produktion
Blutungsgefahr, wenn eine bestimmte Schwelle unterschritten wird,
Evtl. Transfusionen, evtl. Cortisonpräparate
evtl. zusätzliche Beeinträchtigung der Plättchenfunktion
- Unter-/Fehlfunktion des Immunsystems (durch CLL oder Therapie)
Infekte
v.a. obere Luftwegen, Nasennebenhölen, Bronchien → Rauchstopp hifreich!
Impfungen à jour
Antibiotika
Antikörper-Infusionen (Immunglobuline IVIG) → vermindern bei tiefen eigenen Ig Anfälligkeit für
mildere Infekte
Therapiebedingter Abfall der weissen Blutkörperchen (evtl. Medikamente um gesunde weisse
Blutkörperchen zu fördern, GCSF)WORLD LYMPHOMA AWARENESS DAY
18.09.2021 09.50 – 14.45 Uhr
wir informieren, sensibilisieren, beraten, begleiten, vernetzen!
WLAD 2021
LIVE-
WEBINAR
Vorträge und Workshops
Moderation: Marianne Erdin
Prof. Dr. med. Stephan Dirnhofer
Morbus Waldenström
Prof. Dr. med. Urban Novak
Dr. med. Michèle Voegeli
PD Dr. med. Jörg Halter
Prof. Dr. med. Andreas Lohri
Prof. Dr. med. Christoph Mamot
Prof. Dr. med. Emmanuella Guenova PhD
Das Programm richtet sich an PD Dr. med. Christoph Berger
Dr. med. Christiane Jenemann
Erwachsene mit Lymphomen, Prof. Dr. med. Claudia Witt
Angehörige und Interessierte! Claudia Russo
Jörg Halter
Hämatologie
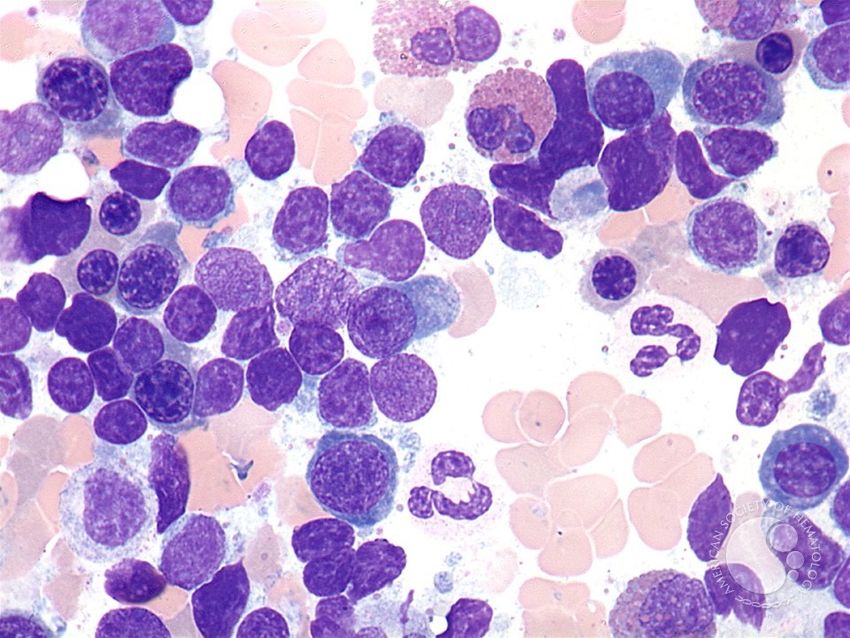
Universitätsspital BaselEinleitung
Lymphoplasmozytisches Lymphom in
Knochenmark +/- ausserhalb Knochenmark
+
IgM Paraprotein im Blut
klonale B-Zellen
Copyrights applyEinleitung Symptome durch: Verdrängung der normalen Blutbildung im Knochenmark + zuviel Eiweiss (IgM) im Blut Seltene Erkrankung: Pro Jahr: 3.4/1‘000‘000 Männer und 1.7/1‘000‘000 Frauen Langsamer, chronischer Verlauf Prognose hat sich im Verlauf der letzten Dekaden ständig verbessert
BLOOD, 19 JUNE 2014 x VOLUME 123, NUMBER 25
Downloaded from
Castillo JJ et al. Blood 2014;123:3999-4000Krankheitsentstehung Ursache - Unklar - Gehäuft bei cronischer Immunstimulation (Hepatitis C, HIV, Autoimmunkrankheiten) - Familiäre Häufung (20x höher) Genetische Veränderungen: - MYD88 bei Mehrheit der MW (90-100%) - Mutationen in CXCR4-Gen bei ca. 40% → vereinbar mit selektion durch chronische Stimulation des Immunsystems
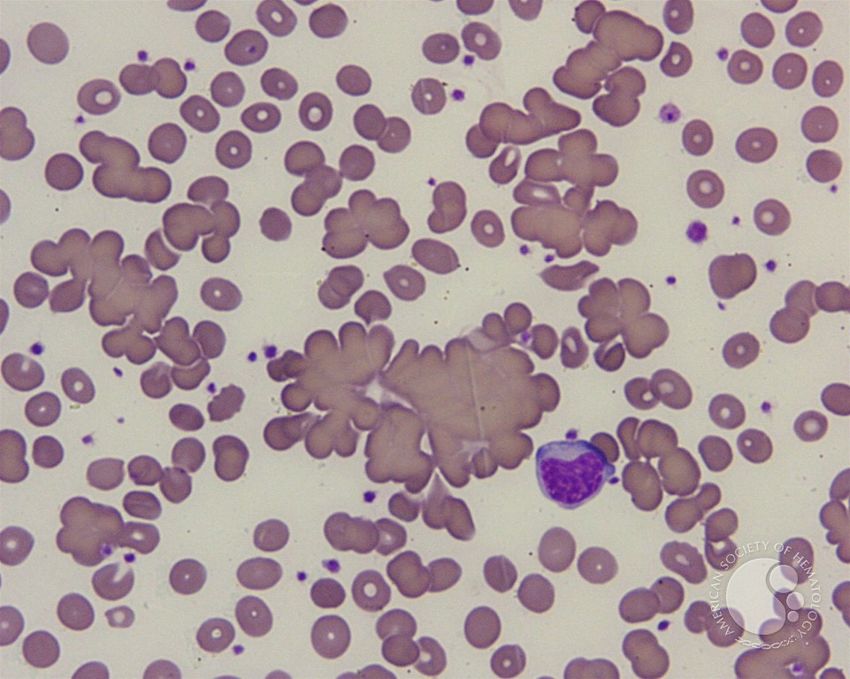
Symptome
Wachstum/Verdrängung ← Klonale B-Zellpopulation → produziert abnormes IgM
Schwäche/Müdigkeit/ Gewichtsverlust Hyperviskositätssyndrom
→ Blut zähflüssiger, Durchblutungsstörungen
KM-Infiltration: Anämie (Blutarmut) → Kopfschmerzen, Sehstörungen,
Vergrösserte Lymphknoten, Milz und/oder Leber Verwirrtheit, Nasenbluten, Atemnot
Blutungsneigung
IgM-Ablagerung in Nieren, Darm (Durchfall),
Haut
IgM gegen körpereigene Strukturen:
periphere Polyneuropathie (Nervenscheiden)
→ Gefühlsstörungen, Ameisenlaufen,
Muskelschwäche (Anti-MAG-Ak)
25% ohne Symptome bei Diagnose Kälteagglutinin-Krankheit (rote BK)
Kryoglobulinämie (Ausfällung bei Kälte)Symptome
Kälteagglutinin-
krankheit
Kryoglobulinämie
-Vaskulitis/Purpura
Hyperviskosiktät -Raynaud
Copyrights applyWann behandeln und wie? Warten bis zum Auftreten von krankheitsassoziierten Symptomen (B-Symptome, Blutarmut, Hyperviskosität, Neuropathie, verminderte Lebensqualität) Therapiebeginn wenn Symptome (oder kurz davor) → wiederholte aktive Suche nach Zeichen der Hyperviskosität
Bustoros et al
A
100
Cumulative Probability of
80
Progression (%)
60
40
30.8% (95% CI, 26.7% to 35.3%)
20
0 2 4 6 8 10
Follow-Up (years)
No. at risk
439 298 183 112 61 34
C BM involvement 70%
100Wann behandeln und wie? Warten bis zum Auftreten von krankheitsassoziierten Symptomen (B-Symptome, Blutarmut, Hyperviskosität, Neuropathie, verminderte Lebensqualität) Therapiebeginn wenn Symptome (oder kurz davor) Symptome Labor Konstitutionelle Symptome Symptomat. Kryoglobulinämie Hyperviskosität Kälteagglutinin-Krankheit Symptomatische Lymphknotenvergrösserung Blutarmut/tiefe Blutplättchen (
Therapiewahl
Plasmapherese Systemische Therapie
→ rasche Gewinnung
Entfernung von Eiweissen
von Blutstammzellen: die periphere Blutstammzellspende
- Vorbehandlung mit G-CSF und/oder
anderen mobilisierenden Medikamenten
- evtl. zentraler Venenkatheter
- Blutverdünnung während
Stammzellsammlung
® Herausforderung: Begleitkrankheiten
Ziel:
≥ 2 Mio Blutstammzellen/kg für autolog
≥ 2(-8) Mio Blutstammzellen/kg für allogen
® Herausforderung: ungenügende
Sammlung („poor mobilizer“)
Josephine Vos, ESH E-Conference 2021Bevorzugte Behandlungsoptionen
Bendamustin + Rituximab
→ für meiste Patienten erste Wahl
Bortezomib + Dexamethason + Rituximab
→ Alternative (z.B. bei aggressiverem Krankheitsverlauf)
Cyclophosphamid + Dexamethason + Rituximab
→ Alternative (z.B. bei geringerer Tumorlast)
Ibrutinib (+/- Rituximab)
→ bei Rezidiv oder keine Immunchemotherapie möglich/gewünscht
Keine Erhaltungstherapie
IWMM10 Consensus, Lancet Haematol 2020Therapie (USB 03/2021)
Morbus Waldenstroem
symptomatic asymptomatic
Plasmapheresis for Plasmapheresis for Observation
symptomatic symptomatic q2-3m, year 1
hyperviscosity, severe hyperviscosity, severe q3-6m > year 1 if stable
cryoglobulinemia or cold cryoglobulinemia or cold
agglutinemia agglutinemia
Reduzierter AZ: R-Benda
or BDR
Niedrig dosierte (Bortezomib, Refractory or
Relapse > 2 years
ChT+Rituximab Dexamethasone, relapse < 2 years
Rituximab) or
Oder I-R or RCD
Ibrutinib (Rituximab,
Endoxan, Ibrutinib Ibrutinib
Oder Dexamethason) (or re-use of previous (or alternative first line
Rituximab first line therapy) regimen)
Monotherapie
Multiple relapses: Alternative regimens and/or subsequent therapies:
autologous or Carfilzomib-D-R
( allogeneic HSCT ) I-DR, R-CHOP, R-CVP, Acalabrutinib, Zanubrutinib,
VenetoclaxTherapie (USB 03/2021)
Morbus Waldenstroem
symptomatic asymptomatic
Plasmapheresis for Plasmapheresis for Observation
symptomatic symptomatic q2-3m, year 1
hyperviscosity, severe hyperviscosity, severe q3-6m > year 1 if stable
cryoglobulinemia or cold cryoglobulinemia or cold
agglutinemia agglutinemia
Reduzierter AZ: R-Benda
or BDR
Niedrig dosierte (Bortezomib, Refractory or
Relapse > 2 years
ChT+Rituximab Dexamethasone, relapse < 2 years
Rituximab) or
Oder I-R or RCD
Ibrutinib (Rituximab,
Endoxan, Ibrutinib Ibrutinib
Oder Dexamethason) (or re-use of previous (or alternative first line
Rituximab first line therapy) regimen)
Monotherapie
Multiple relapses: Alternative regimens and/or subsequent therapies:
autologous or Carfilzomib-D-R
( allogeneic HSCT ) I-DR, R-CHOP, R-CVP, Acalabrutinib, Zanubrutinib,
VenetoclaxAusblick Unter Evaluation für Erstlinientherapie (und Rezidivbehandlung) Ibrutinib + Rituximab Acalabrutinib Zanabrutinib Venetoclax Ixazomib + Rituximab + Dexamethason Carfilzomib-basierte Therapien → Alternative bei Polyneuropathie
Sie können auch lesen