Bei fortgeschrittener Niereninsuffizienz? - Neue Antikoagulantien: mehr Risiko als Nutzen
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Neue Antikoagulantien:
mehr Risiko als Nutzen
bei fortgeschrittener Niereninsuffizienz?
Jürgen Floege
Division of Nephrology & Immunology
juergen.floege@rwth-aachen.de
Bansal N et al, Clin J Am Soc Nephrol. 2016 Apr 12
CRIC Studie: Vorhofflimmern und CKD-Progression
3091 CKD Patienten (mittleres Follow-up 5.9 Jahre)
Kein VHF Neues VHF
ESRD (n=581) ESRD (n=47)
3.4/100 Personenjahre 11.8/100 Personenjahre
ESRD Risiko 3.2x
(95% confidence interval, 1.9-5.2)*
* marginal structural models with inverse probability weighting. Association consistent across subgroups by age, sex, race, diabetes
status, and baseline eGFR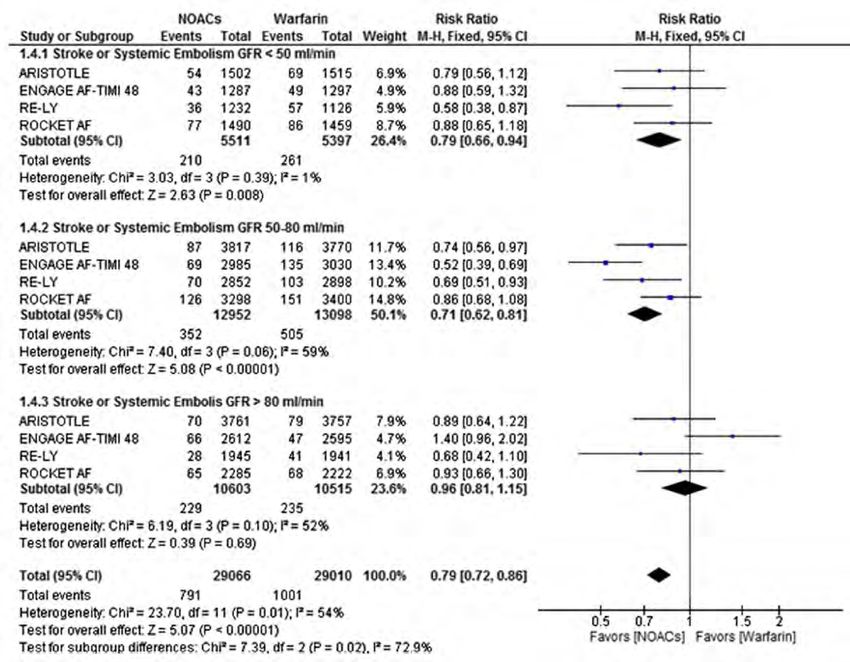
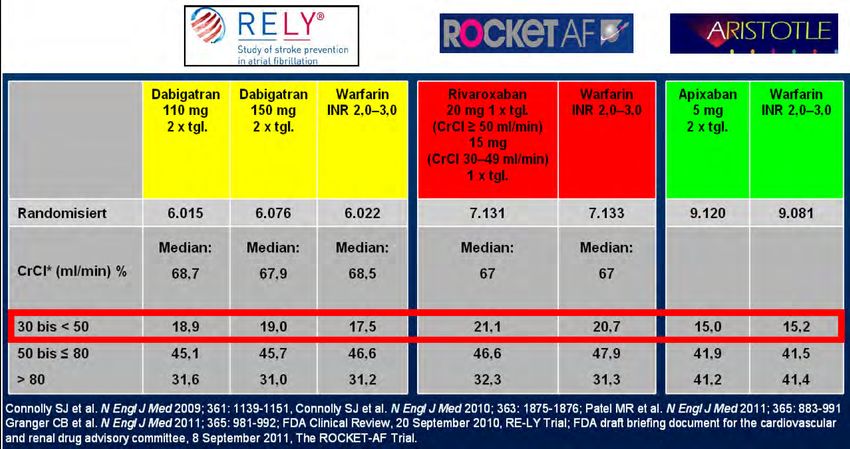
Neue orale Antikoagulantien bei CKD
CKD
Stadium GFR Dabigatran Rivaroxaban Apixaban Edoxaban
1 >90
Ja Ja Ja Ja
2 90-60
Ja Ja Ja Ja
3 59-30
Ja Ja Ja Ja
4 29-15 Nein (EMA) „vorsichtig“ Ja Ja
(FDA: reduced
dose)
(Nur Prophylaxe) (reduz. Dosis) (reduz. Dosis)
5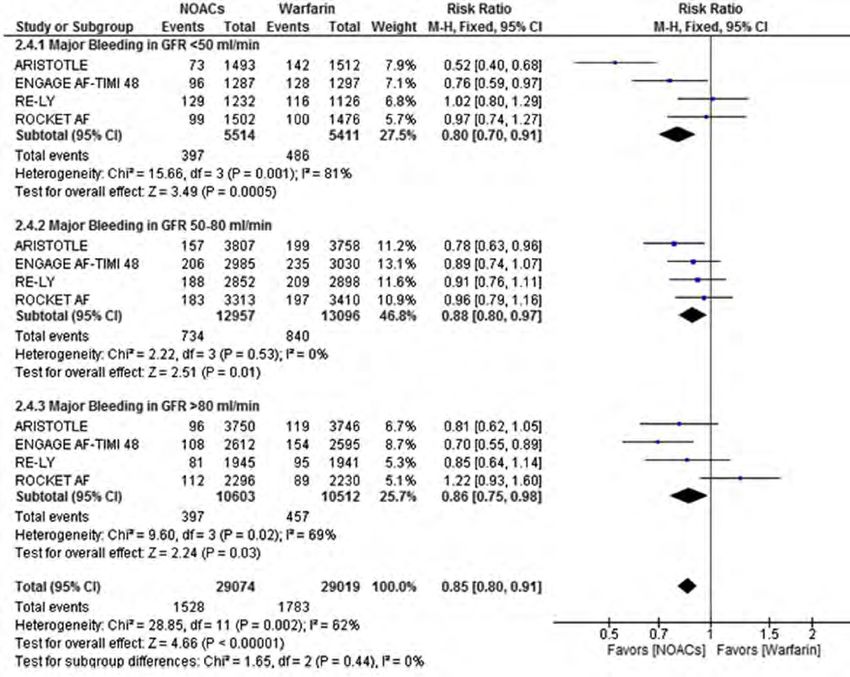
Neue Antikoagulantien: mehr Risiko als Nutzen
bei fortgeschrittener Niereninsuffizienz?
GFR 30-60 ml/min
• NOAKs überwiegend ähnlich wie VKA
evtl. vorteilhaft in Hinblick und Wirkung
und Blutungen
• Aber: rechtfertigt das jährliche NOAK
Therapiekosten >1100 € vs. 65 € für Coumarine?
(number-needed-to-treat >200 für NOAK Benefit)
NOAK, neue orale Antikoagulantien VKA, Vitamin K Antagonist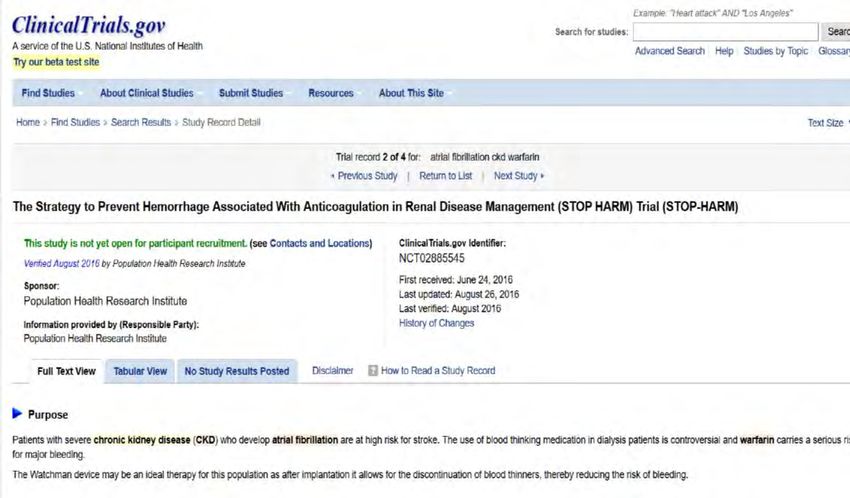
Canadian Journal of Cardiology 31 (2015) 1207e1218 Canadian Society of Cardiology Guidelines 2014 Recommendation 11 – Antithrombotic therapy should relate to eGFR eGFR >30 mL per minute: We recommend that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as detailed in recommendations for patients for patients with normal renal function (Strong Recommendation, High-Quality Evidence). eGFR 15-30 mL per minute and not on dialysis: We suggest that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as for patients with normal renal function. The preferred agent for these patients is warfarin (Conditional Recommendation, Low-Quality Evidence). eGFR
Reinecke H et al, Stroke 2013;44:2935-2941
Jährliche Rate schwerer
Blutungen
Apoplex / Embolie
Prävention vs. Blutungen
6
(RE-LY, ROCKET-AF, ARISTOTLE Studie)
5
Jährliche Rate von Apoplexen / 4
system. Embolien
3 3
[%]
2 2
[%]
1 1
0 0
80 80
Kreatinin Clearance [ml/min]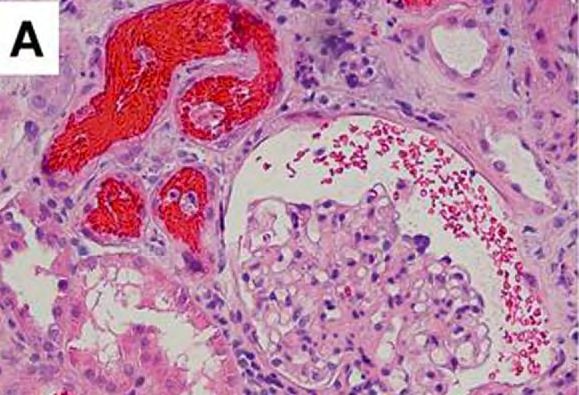
Del-Carpio Munoz F et al
Am J Cardiol
2016; 117: 69-75
GFR 80 ml/min
Apoplexe
Embolien
NOAK Warf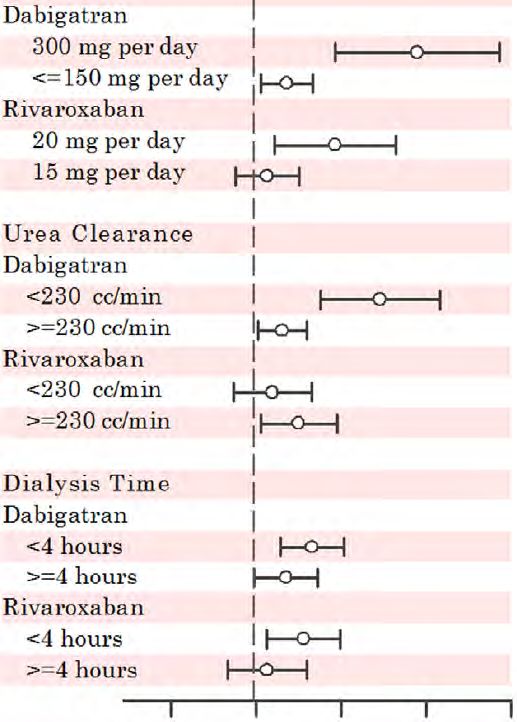
Del-Carpio Munoz F et al
Am J Cardiol
2016; 117: 69-75
GFR 80 ml/min
Blutungen
NOAK Warf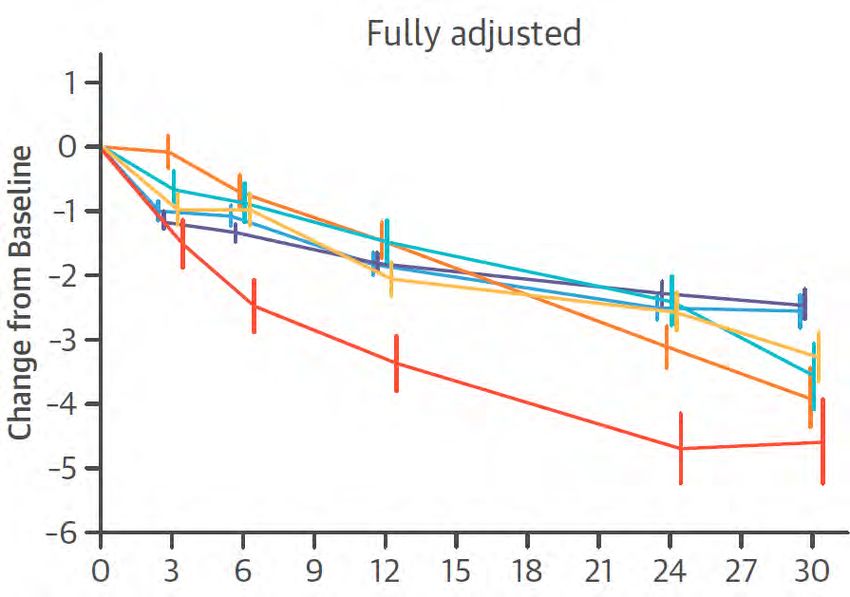
(GFR 30-50 ml/min) • 8 randomisierte Studien, ca. 10.000 Patienten • KEIN sign. Unterschied in Hinblick auf Apoplex / Embolien • KEIN sign. Unterschied bei Blutungen

Lega JC et al, J Thromb Haemost 2013
Renale Exkretion von oralen Antikoagulantien
versus Blutungsereignisse
Meta-Regressionsanalyse von Phase III Studien zu NOAKs versus Vitamin-K
Antagonisten (VKAs) in Patienten mit eGFR < 50 mL/min.
Risk Ratio NOAK / Vit K Antag
2 35% Vit K Antagonist
Edo besser
1
0,5
80%
NOAK besser
Dabi
0,1 25% 33% Ximel
Apix Riva
20 40 60 80
Renale Exkretion [%]SV Brodsky et al Am J Kidney Dis 2009 Antikoagulantien-induzierte Nephropathie
Böhm M et al. J Am Coll Cardiol. 2015;65:2481-93
Antikoagulation versus GFR-Verlust
18.113 Patienten mit VHF
CHA2DS2-VASC ≥ 1
Dabigatran Dabigatran Warfarin
2 x 110 mg 2 x 150 mg INR 2.0 – 3.0
eGFR 66 ml/min eGFR 66 ml/min eGFR 66 ml/min
eGFR VerlaufBöhm M et al. J Am Coll Cardiol. 2015;65:2481-93
Antikoagulation versus GFR-Verlust
Delta eGFR vs. Baseline
Dabigatran (2x150 mg)
Dabigatran (2x110 mg)
Warfarin
(INR meist OK)
Warfarin
Warfarin (INR meist zu niedrig)
(INR meist zu hoch)
Fully adjusted modelNeue Antikoagulantien: mehr Risiko als Nutzen
bei fortgeschrittener Niereninsuffizienz?
GFR 15-30 ml/min
• Keine guten Daten zu NOAKs versus
VKA in Hinblick auf Effektivität und
Blutungen
NOAK, neue orale Antikoagulantien VKA, Vitamin K AntagonistNOAKs: Erfahrungen bei höhergradiger CKD Randomized:
Canadian Journal of Cardiology 31 (2015) 1207e1218 Canadian Society of Cardiology Guidelines 2014 Recommendation 11 – Antithrombotic therapy should relate to eGFR eGFR >30 mL per minute: We recommend that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as detailed in recommendations for patients for patients with normal renal function (Strong Recommendation, High-Quality Evidence). eGFR 15-30 mL per minute and not on dialysis: We suggest that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as for patients with normal renal function. The preferred agent for these patients is warfarin (Conditional Recommendation, Low-Quality Evidence). eGFR
Schlieper, Floege et al., DGfN Kongress 2016
GCKD-Studie (CKD IV und V):
Antikoagulation bei VHF-Patienten
140,0%
chronic atrial fibrillation (n=250)
120,0%
intermittent atrial fibrillation (n=208)
100,0%
80,0%
60,0%
40,0%
20,0%
0,0%Neue Antikoagulantien: mehr Risiko als Nutzen
bei fortgeschrittener Niereninsuffizienz?
GFR unter 15 ml/min
• Fast keine Daten zu NOAKs versus VKA
in Hinblick auf Effektivität + Blutungen
• Nur Apixaban zugelassen in reduzierter
Dosis (USA)
NOAK, neue orale Antikoagulantien VKA, Vitamin K AntagonistCanadian Journal of Cardiology 31 (2015) 1207e1218 Canadian Society of Cardiology Guidelines 2014 Recommendation 11 – Antithrombotic therapy should relate to eGFR eGFR >30 mL per minute: We recommend that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as detailed in recommendations for patients for patients with normal renal function (Strong Recommendation, High-Quality Evidence). eGFR 15-30 mL per minute and not on dialysis: We suggest that such patients receive antithrombotic therapy according to their risk as determined by the “CCS algorithm” as for patients with normal renal function. The preferred agent for these patients is warfarin (Conditional Recommendation, Low-Quality Evidence). eGFR
Limdi NA et al, J Am Soc Nephrol. 2009;20:912-21
Vitamin K Antagonisten:
„time-in-therapeutic range“ sinkt mit sinkender GFR
GFR (ml/min per 1.73 m2)
≥60 30 to 59 4
Ereignisse: 392 251 93
INR >4 Inzidenz 84 104 189
Rate (76 - 93) (92 - 118) (153 - 232)
Große
Hämorrhagie 6 8 31
Inzidenz Rate (4,1 - 8,9) (5,1 – 12,8) (17,0 – 50,3)Jun M et al, BMJ 2015; 350: h246
GFR und schwere Blutungen bei Patienten mit VHF
zu Beginn von Vitamin-K Antagonisten
Inzidenz schwerer Blutungen pro 100
Personenjahre (95% CI)
Hohes Risiko bei reduzierter GFR innerhalb der ersten 30 TageModified after Shah M et al. Circulation 2014
Warfarin-Therapie vs. Risiko von Apoplex / Tod
in Dialysepatienten mit Vorhhofflimmern
Chan 2009 (stroke/death)
Wizeman 2010 (stroke/death 75y)
Winkelmayer 2011 (ischemic stroke)
Winkelmayer 2011 (hemorrhagic stroke)
Shah 2014 (ischemic stroke)
„Renal replace-
ment therapy“
Olesen 2012 (stroke/death)
Bonde 2015 (death)
0.01 0.1 1 10 100
Pro Warfarin Kontra WarfarinKrüger T, Brandenburg V, Schlieper G, Marx N, Floege J. NDT 2013; 28:534-41
Wenn Sie heute mein Dialysepatient mit
Vorhofflimmern wären: Coumarin ja oder nein?
„Keine Frage“ „Unsicherheit Risiko-Nutzen-Ratio“ „Keine Frage
Komorbidität Keine eindeutige (Kontra-)Indikation Komorbidität
(mechan. (z.B. Stürze,
Klappe, Blutungen)
Lungen-
Embolie etc)
Risiko Risiko Risiko Risiko
Embolien Blutung kardio- Calci-
ischäm. (GI, vaskul. phylaxie
Coumarin Apoplex? zerebral..) Kalk Coumarin
CoumarinBuiten MS et al, Heart 2014; 100: 685-90 Vorhofflimmern bei HD Patienten: 1) Häufig 2) meist an HD Tagen 3) meist an/früh nach HD 14/40 ICD Patienten mit 1-213 VHF-Episoden
Chan KE et al, Circulation 2015; 131: 972-79 Schwere Blutungen unter Dabigatran
oder Rivaroxaban versus Warfarin
NOAKs
NOAK better NOAK worse
bei Dialysepatienten:
Die Realität…..
(29977 HD Patienten mit VHF)
3 Dabi 2x75 mg
Point prevalence (per 100 pts)
Riva 15 mg
2
1 Dabi 2x150 mg
Riva 20 mg
0
2010 2012 2014
0 1 2 3 4Monitoring & Antagonismus oraler Antikoagulantien
Monitoring Antagonismus
Vitamin K Vitamin K
INR
Antagonisten FFPs
Thrombinzeit Idarucizumab
Dabigatran Ecarin clotting time Dialyse
(Blutspiegel) Faktoren-Substitution*
Anti-Xa Aktivität Andexanet alfa
Rivaroxaban
(Blutspiegel) Faktoren-Substitution*
Anti-Xa Aktivität Andexanet alfa
Apixaban
(Blutspiegel) Faktoren-Substitution*
Anti-Xa Aktivität Andexanet alfa
Edoxaban
(Blutspiegel) Faktoren-Substitution*
* - Prothrombinkomplex Konzentrat,
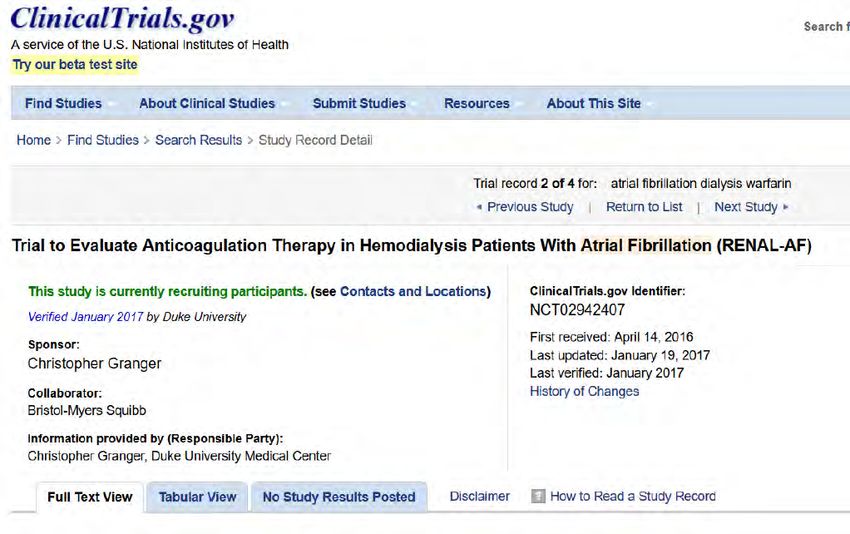
Aktivierter Faktor VIIUSA (Dez. 2016 bis Ende 2019): • Apixaban versus Warfarin bei 762 Dialyse- patienten mit VHF • Primärer Endpunkt Blutungen nach 15 Monaten • Sekundärer Endpunkt Apoplex
Kanada (Ende 2016 bis Ende 2021): • Vorhofohr-Verschluss versus orale Antikoagulation (VKA, NOAK) bei 23 (?) Dialysepatienten oder GFR
Was hat Floege gesagt….? GFR 30-60 ml • NOAKs i.d.R. ähnlich wie oder etwas besser als VKA in Hinblick auf Benefit und Blutungen • Apixaban (evtl.) besser angesichts AKI Risiko bei CKD • Benefit NOAK vs. VKA in Hinblick auf CKD-Progression?? • Aber: hohe Therapiekosten + hohe number-needed-to-treat GFR 15-30 ml • Keine guten Daten NOAKs meiden GFR
Sie können auch lesen