GERINNUNGSAKTIVIERUNG DURCH SARS-COV-2 UND COVID-19-IMPFUNG - WAS IST BEKANNT?
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Gerinnungsambulanz und Hämophiliezentrum
II. Medizinische Klinik und Poliklinik
Onkologie, Hämatologie und KMT mit der Sektion Pneumologie
4. Schleswig-Holsteiner Tag der Gerinnung – Sonnabend, 11. September 2021
Gerinnungsaktivierung durch SARS-CoV-2 und COVID-19-Impfung –
Was ist bekannt?
Florian Langer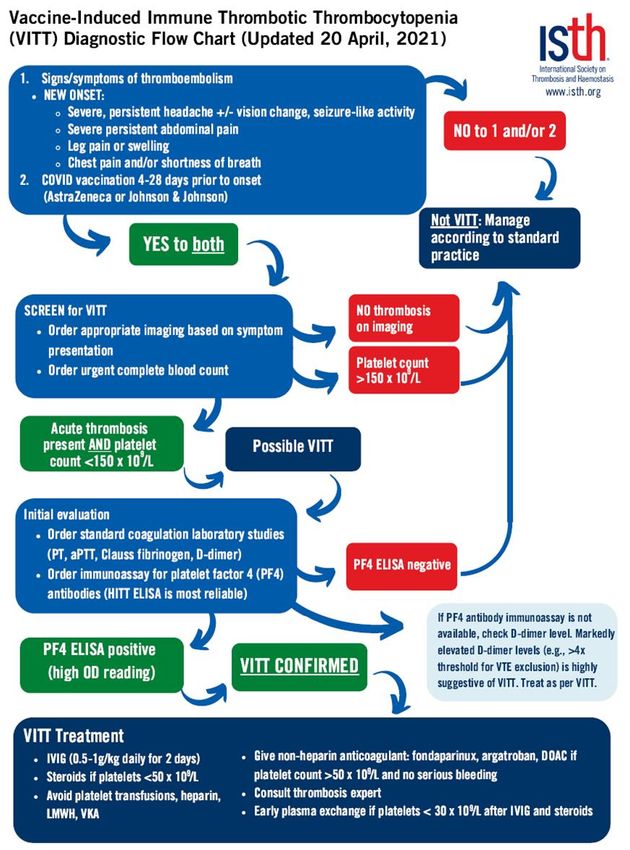
Offenlegung potentieller Interessenkonflikte
Anstellungsverhältnis oder Keine
Führungsposition
Beratungs- bzw. Gutachtertätigkeit Ablynx, Alexion, Aspen, Bayer, BioMarin, Boehringer Ingelheim, BMS, Chugai,
CSL Behring, Daiichi Sankyo, LEO Pharma, Mitsubishi Tanabe Pharma, Novo
Nordisk, Octapharma, Pfizer, Roche, Shire, SOBI, Takeda, Viatris
Besitz von Geschäftsanteilen, Aktien oder Keine
Fonds
Patent, Urheberrecht, Verkaufslizenz Keine
Honorare Alexion, Aspen, Baxalta, Bayer, Boehringer Ingelheim, BMS, Chugai, CSL
Behring, Daiichi Sankyo, Grifols, LEO Pharma, Mitsubishi Tanabe Pharma, Novo
Nordisk, Octapharma, Pfizer, Sanofi, Shire, Siemens, SOBI, Stago, Werfen
Finanzierung wissenschaftlicher Bayer, CSL Behring, Intersero, Novo Nordisk, Pfizer, SOBI
Untersuchungen
Andere finanzielle Beziehungen Keine
Immaterielle Interessenkonflikte Keine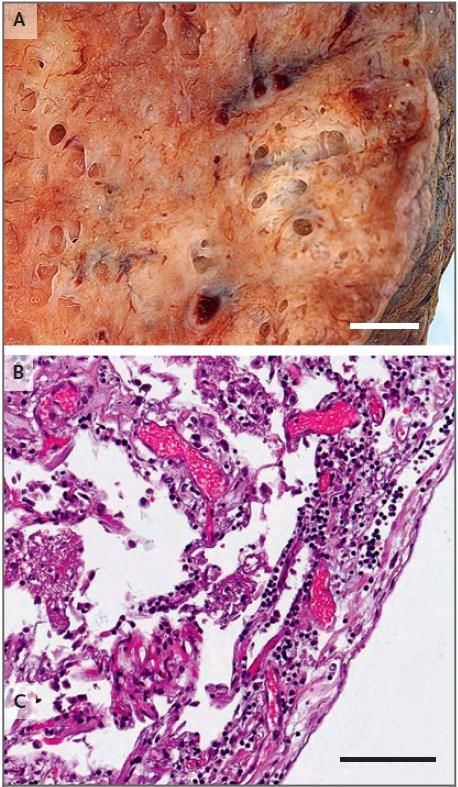
Was sind Thromboinflammation und Immunothrombose?
Thromboinflammation
Hämostase Entzündung
Immunothrombose
Engelmann & Massberg. Nat Rev Immunol 2013; 13: 34-45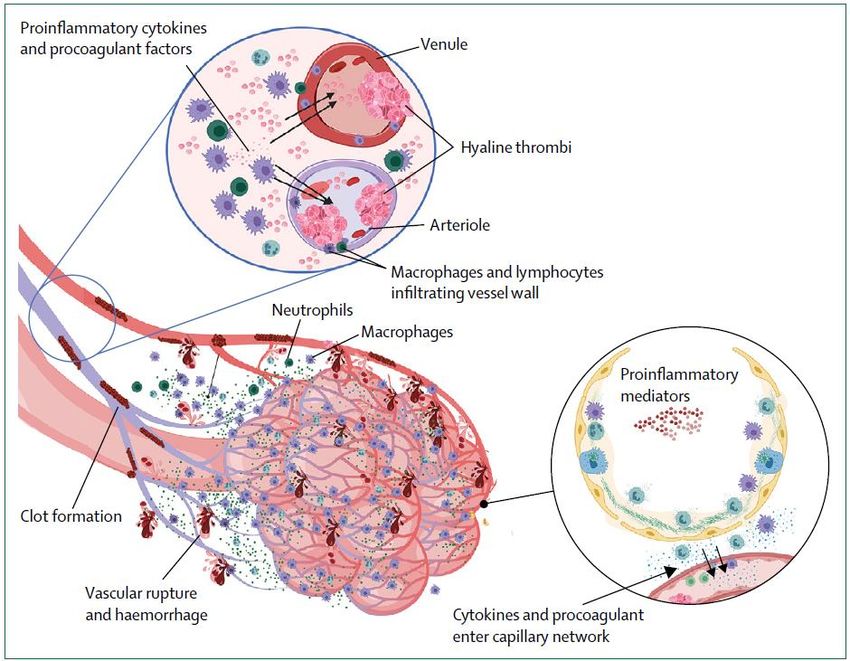
Thromboembolische Ereignisse bei COVID-19
1 Tiefe Venenthrombose (TVT)
59 %
(95% KI 42 – 72 %)
Migration
Embolus 9.2 %
(95% KI 2.6 – 21.0 %)
Thrombus • 198 COVID-19 Patienten (n=75 ICU, n=123 Normalstation)
• Prophylaktische oder (vorbestehende) therapeutische
2 Lungenarterienembolie (LAE) Antikoagulation bei n=186 (94 %)
• VTE bei n=39 (20 %): 13 LAEs ± TVT, 26 TVTs
ICU Intensivstation Middeldorp et al. J Thromb Haemost 2020; 18: 1995-2002
VTE Venöse Thromboembolie Modifiziert nach Tapson. N Engl J Med 2008; 358: 1037-52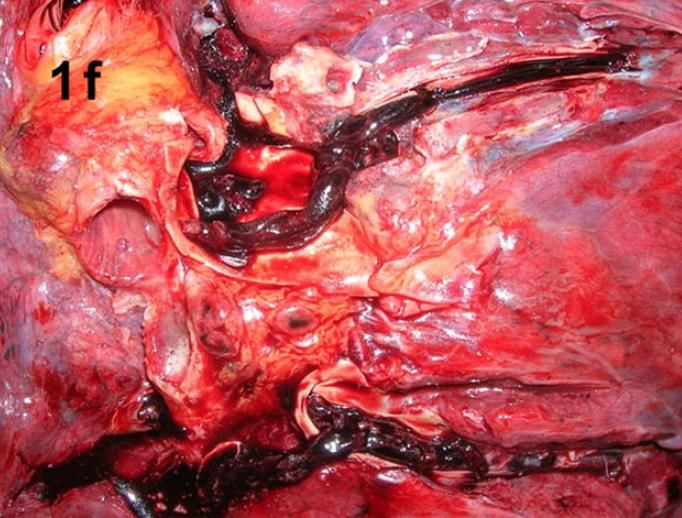
Die VTE trägt bei COVID-19 in erheblichem Maße zur Morbidität und Mortalität bei
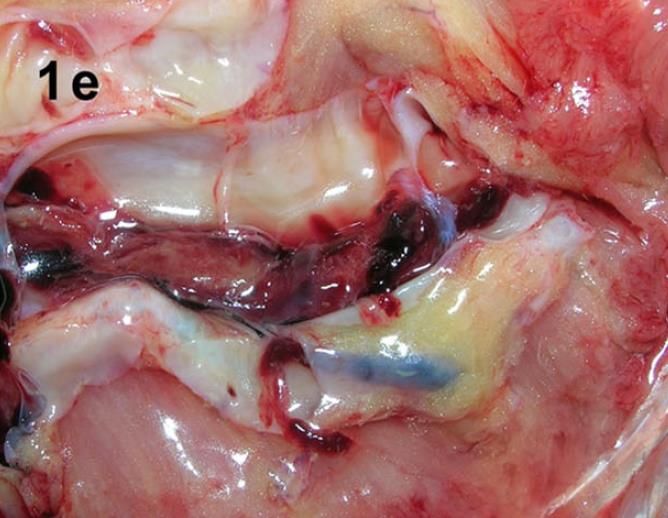
• 12 konsekutive Patienten • 80 konsekutive Patienten mit kompletter Autopsie
mit kompletter Autopsie • Massive, letale LAE (+ TVT) bei 8 Patienten (10 %)
• Beidseitige TVT bei 7/12 • Periphere LAE (+ TVT) bei 9 Patienten (11 %)
Patienten (58 %)
• Isolierte TVT bei 16 Patienten (20 %)
• Massive, letale LAE (+ TVT)
• VTE (LAE und/oder TVT) bei 33 Patienten (41 %)
bei 4/12 Patienten (33 %)
• 36 % der VTE-Patienten ambulant verstorben
• 2 Patienten ambulant an
LAE verstorben
• Thrombosierte Prostata-
Venen bei 6/9 Männern
• Keine VTE ante mortem
diagnostiziert
VTE Venöse Thromboembolie
LAE Lungenarterienembolie Edler et al. Int J Legal Med 2020; 134: 1275-84
TVT Tiefe Venenthrombose Wichmann et al. Ann Intern Med 2020; 173: 268-77
VTE-Prävalenz bei COVID-19: Systematische Übersicht und Metaanalyse
Nicht-
Intensivstation
7,9 %
Kein Screening (95 %-KI 5,1–11,2)
9,5 %
(95 %-KI 7,5–11,7)
Gesamt Intensivstation
14,1 % 22,7 %
(95 %-KI 11,6–16,9) (95 %-KI 18,1–27,6)
Screening
40,3 %
(95 %-KI 27,0–54,3)
Nopp et al. Res Pract Thromb Haemost 2020; 4: 1178-91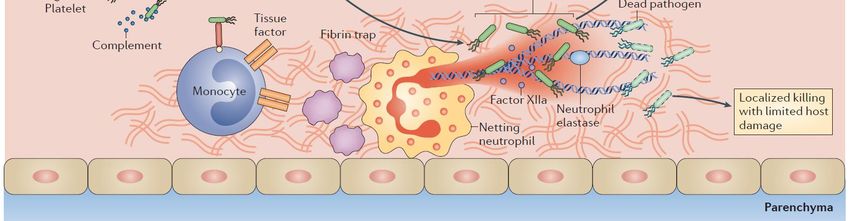
Alveoläre Entzündung, kapilläre Mikrothromben und Angiogenese bei COVID-19
Pulmonale intravaskuläre Koagulopathie (PIC)
Ackermann et a. N Engl J Med 2020; 383: 120-8
Mc Gonagle et al. Lancet Rheumatol 2020; 2: e437-45
Thrombin verstärkt die SARS-CoV-2-induzierte Thromboinflammation: Circulus vitiosus GPCR G-Protein-gekoppelter Rezeptor ANG II Angiotensin II ACE2 Angiotensin-konvertierendes Enzym 2 Sriram & Insel. Br J Pharmacol 2020; 177: 4971–4
COVID-19: (Exponentieller) Anstieg der D-Dimere mit ungünstiger Prognose assoziiert
Fibrinopeptide A Fibrinopeptide B
D E D Fibrinogen
D-dimer (µg/mL)
Fibrin Clot
D E D D E D D E D D
D D E D D E D D E
Plasmin Fibrinolyse
D E D D E D D E D D
D D E D D E D D E
Intermediäre Fragmente
Days from admission D E D D E D D D D
D D E D D E E
Komplette Clot Lyse
D D E
Was ist die primäre Ursache erhöhter D-Dimere: Fibrinolyse? Thrombingenerierung? Beides? D-Dimer Fragment E
Zhou et al. Lancet 2020; 395: 1054-62
Tang et al. J Thromb Haemost 2020; 18: 844-7
Modifiziert nach Bockenstedt. New Engl J Med 2003; 349: 1203-4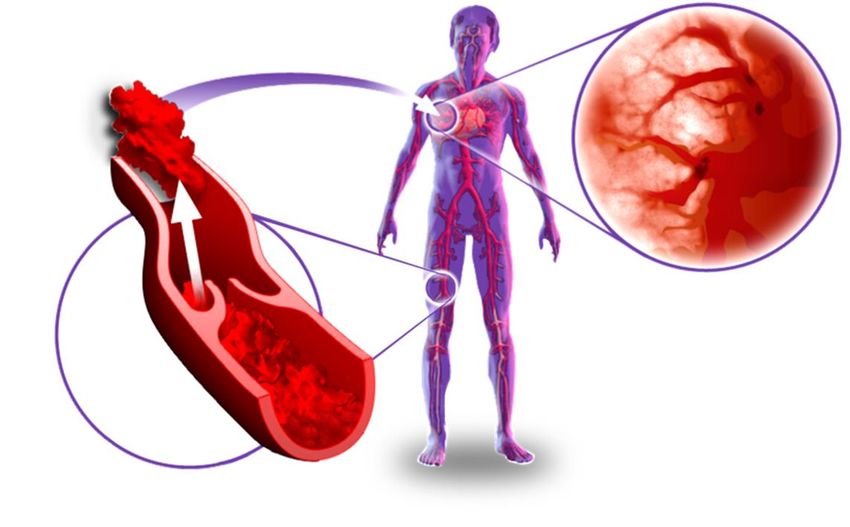
Das antikoagulatorische System
TF
VIIa
Xa PT Va + VIIIa
Thrombin
APC Protein S
Thrombin
Thrombomodulin
Protein C
APC Aktiviertes Protein C
PT ProthrombinDas antikoagulatorische System
TF
VIIa
Xa PT Va + VIIIa
Thrombin
APC Protein S
Thrombin
Thrombomodulin
Protein C
APC Aktiviertes Protein C
PT ProthrombinEndothelinfektion bei COVID-19: Endotheliitis/Endotheliopathie
Viruspartikel peritubulär Apoptose von mononuklären Apoptose von mononuklären
und in Endothelzellen der und Endothelzellen in der und Endothelzellen in der
Nierenglomeruli Intima von Dünndarmgefäßen Intima von Lungengefäßen
Varga et al. Lancet 2020; 395: 1417-8Biomarker der Endotheliopathie mit ungünstiger Prognose bei COVID-19 assoziiert
• Freisetzung von sTM
durch Aktivierung oder
Schädigung von
Endothelzellen
• Lösliches P-Selektin als
weiterer Biomarker der
Endotheliopathie
à Hinweis für defekte
Aktivierung des
antikoagulatorischen
Protein C-Weges
sTM Lösliches Thrombomodulin
TAT Thrombin-Antithrombin-Komplex
VWF Von-Willebrand-Faktor Goshua et al. Lancet Hematol 2020; 7: e575-82Thromboinflammation und Krankheitsprogression bei COVID-19 VWF von Willebrand factor PAI-1 plasminogen activator inhibitor-1 NET neutrophil extracellular trap O‘Sullivan et al. Lancet Hematol 2020; 7: e553-5
Pleiotrope Effekte von (niedermolekularem) Heparin
Proliferation
Antithrombotische
- Endothel- und Epithelzellen
Immunabwehr Wirkung
- Fibroblasten
- NK-Zellaktivität - Gefäßmuskelzellen
Antiinflammatorische
Angiogenese Wirkung ?
Adhäsion
- Thrombin + Fibrin
- Hemmung von VEGF + bFGF
Heparin - Hemmung von P- und L-Selektin
- TF-Expression
Apoptose + Migration + Invasion Antivirale
Differenzierung - Hemmung von Heparinase
Wirkung ?
- Blockierung von ECM-ProteinenIntensitäten der parenteralen und oralen Antikoagulation
Beispiel Enoxaparin (z.B. Clexane®) Beispiel Apixaban (Eliquis®) Beispiel Rivaroxaban (Xarelto®)
Therapeutische Dosis Therapeutische Dosis Therapeutische Dosis
• 2 x 1,0 mg/kg s.c./Tag (z.B. 2 x 80 mg • 2 x 10 mg/Tag • 2 x 15 mg/Tag
bei 80 kg)
Halbtherapeutische/intermediäre Dosis Halbtherapeutische/intermediäre Dosis Halbtherapeutische/intermediäre Dosis
• 2 x 0,5 mg/kg s.c./Tag (z.B. 2 x 40 mg • 2 x 5 mg/Tag • 1 x 20 mg/Tag (1 x 15 mg/Tag)
bei 80 kg)
• 1 x 1,0 mg/kg s.c./Tag (z.B. 1 x 80 mg
bei 80 kg)
Prophylaktische Dosis Prophylaktische Dosis Prophylaktische Dosis
• Niedriges-intermediäres Risiko: 0,2 ml • 2 x 2,5 mg/Tag • 1 x 10 mg/Tag
= 20 mg = 2.000 IE Anti-Xa s.c./Tag
• Hohes Risiko: 0,4 ml = 40 mg = 4.000 IE
Anti-Xa s.c./TagStellenwert der prophylaktischen Antikoagulation bei COVID-19
• 449 Patienten mit schwerem
COVID-19 Verlauf aus Wuhan,
China
• Ausschlusskriterien:
Blutungsneigung, Hospitalisierung
< 7 Tage, Alter < 18 Jahre etc.
• 99 Patienten (22,0 %) mit Heparin
≥ 7 Tage:
- n=94 Enoxaparin 40 – 60 mg/Tag
- n=5 UFH 10.000 – 15.000 IE/Tag
• 97 Patienten (21,6 %) mit SIC
• Primärer Endpunkt: 28-Tages-
Mortalität
SIC Sepsis-induzierte Koagulopathie Tang et al. J Thromb Haemost 2020; 18: 1094-9Definition: Sepsis-induzierte Koagulopathie (SIC) vs. DIC DIC Disseminierte intravasale Gerinnung Iba et al. J Thromb Haemost 2019; 17: 1989-94
Stellenwert der prophylaktischen Antikoagulation bei COVID-19
a P < 0.05
D-D D-Dimere
ULN Oberer Referenzbereich Tang et al. J Thromb Haemost 2020; 18: 1094-9Medikamentöse VTE-Prophylaxe bei hospitalisierten Patienten mit COVID-19
P = 0,002
P = 0,009
60 P = 0,007
1 Tiefe Venenthrombose (TVT)
50
(95 %-Konfidenzintervall)
VTE-Inzidenzrate
Migration
40
Embolus
P = 0,18
P = 0,32
30
20
Thrombus
10
2 Lungenarterienembolie (LAE)
0
Keine Standard Intermediäre Therapeutische
Prophylaxe Prophylaxe Dosis Dosis
Patell et al. Thromb Haemost 2021; 121: 76-85Ist die therapeutische Antikoagulation bei hospitalisierten COVID-19
Patienten mit einem Überlebensvorteil assoziiert?
Paranjpe et al. J Am Coll Cardiol 2020; 76: 122-4Therapeutische Antikoagulation mit (niedermolekularem) Heparin bei COVID-19 • 2219 patients with moderate disease activity • 1098 critically ill patients • Therapeutic anticoagulation vs. usual care • Therapeutic anticoagulation vs. usual care thromboprophylaxis (27 % intermediate dose) thromboprophylaxis (51 % intermediate dose) • Primary outcome: organ support-free days up to • Primary outcome: organ support-free days up to day 21 (reflecting ICU-level care and survival) day 21 (reflecting ICU-level care and survival)
Therapeutische Antikoagulation mit (niedermolekularem) Heparin bei
moderat kranken COVID-19-Patienten: Primärer Endpunkt
Proportion of patients surviving
without organ support
80.2 % 77.9 % 81.2 %
76.4 % 72.2 % 79.8 %
OR 1.27 OR 1.31 OR 1.27
(1.03–1.58) (1.00–1.76) (0.93–1.57)
Overall High Low
group D-dimer D-dimer
(≥ 2 mg/L) (< 2 mg/L)
OR adjusted odds ratio The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. N Engl J Med 2021 (Epub ahead of print)Therapeutische Antikoagulation mit (niedermolekularem) Heparin bei
moderat kranken COVID-19-Patienten: Sekundäre Endpunkte
Outcome Therapeutic-Dose Usual-Care Adjusted
Anticoagulation Thromboprophylaxis Odds Ratio (95% CI)
Survival until hospital
92.7 % 91.8 % 1.21 (0.87 – 1.68)
discharge
Survival without organ
79.3 % 75.4 % 1.30 (1.05 – 1.61)
support at 28 days
Progression to intubation
10.9 % 12.1 % 0.82 (0.63 – 1.07)
or death
Major thrombotic event or
8.0 % 9.9 % 0.72 (0.53 – 0.98)
Death
Major thrombotic event 1.1 % 2.1 %
Death in hospital 7.3 % 8.2 %
Major bleeding 1.9 % 0.9 % 1.80 (0.90 – 3.74)
CI credible interval The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. N Engl J Med 2021 (Epub ahead of print)Therapeutische Antikoagulation mit (niedermolekularem) Heparin bei
kritisch kranken COVID-19-Patienten: Primärer Endpunkt
Organ support-free days
median no. (IQR)
1 (-1–16)
4 (-1– 6)
OR 0.83
(0.67–1.03)
OR adjusted odds ratio The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. N Engl J Med 2021 (Epub ahead of print)Therapeutische Antikoagulation mit (niedermolekularem) Heparin bei
kritisch kranken COVID-19-Patienten: Sekundäre Endpunkte
Outcome Therapeutic-Dose Usual-Care Adjusted
Anticoagulation Thromboprophylaxis Odds Ratio (95% CI)
Survival to hospital
62.7 % 64.5 % 0.84 (0.64 – 1.11)
discharge
Major thrombotic events or
40.1 % 41.1 % 1.04 (0.79 – 1.35)
Death
Major thrombotic events 6.4 % 10.4 %
Death in hospital 37.3 % 35.5 %
Any thrombotic events or
40.9 % 41.4 % 1.04 (0.79 – 1.35)
Death
Any thrombotic events 7.2 % 11.1 %
Death in hospital 37.3 % 35.5 %
Major bleeding 3.8 % 2.3 % 1.48 (0.75 – 3.04)
CI credible interval The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. N Engl J Med 2021 (Epub ahead of print)Wann ist eine therapeutische Antikoagulation mit NMH am ehesten sinnvoll? NMH Niedermolekulares Heparin Pfeifer & Hamer. Internist 2020; 61: 793-803
Halbtherapeutische Antikoagulation mit NMH bei COVID-19 auf der ICU (INSPIRATION)
Kombinierter primärer Endpunkt
• Venöse oder arterielle Thromboembolie
• ECMO-Therapie
• 30-Tages-Mortalität
Sekundäre Endpunkte
• 30-Tages-Mortalität
• Venöse Thromboembolie
• Tage ohne invasive Beatmung
NMH Niedermolekulares Heparin
ECMO Extrakorporale Membranoxygenierung Sadeghipour et al. JAMA 2021; 325: 1620-30Intensivierte Antikoagulation mit Rivaroxaban bei COVID-19 (ACTION) • Hospitalisierte Patienten mit erhöhten D-Dimeren • Moderater Verlauf bei etwa 80 % • Rivaroxaban 1 x 20 mg/Tag vs. NMH-Prophylaxe NMH Niedermolekulares Heparin Lopes et al. Lancet 2021; 397: 12-8
Therapeutische Antikoagulation auf der ICU bei manifester VTE
200
Ursachen einer "Heparin-Resistenz"
TZ (=Thrombinzeit)
• Antithrombin-Mangel
• Faktor VIII ↑
Gerinnungszeit (sec)
150
• Fibrinogen ↑
100 • Plä chenfaktor 4 ↑
APTT • …
50
"Spontane" APTT-Verlängerung
0
UFH-Konzentration im Plasma
• Faktor XII ↓
• Faktor XI ↓
ICU Intensivstation
VTE Venöse Thromboembolie
UFH Unfraktioniertes Heparin
APTT Aktivierte partielle ThromboplastinzeitThromboembolische Ereignisse und Gesamtmortalität nach Krankenhausentlassung
IMPROVE-DD Risk Score for VTE
Previous VTE 3 points
Known thrombophilia 2 points
Current lower-limb
paralysis 2 points
Current cancer 2 points
Immobilization ≥ 7 days 1 point
ICU/CCU admission 1 point
Age > 60 years 1 point
D-dimer ≥ 2 × ULN 2 points
ACM all-cause mortality
CV cardiovascular
CKD chronic kidney disease Giannis et a. Blood 2021; 137: 2838-47Poststationäre VTE-Prophylaxe mit Rivaroxaban: MICHELLE-Studie
• Rivaroxaban 10 mg/Tag (n=160) vs. Beobachtung
(n=160) über 35 ± 4 Tage nach 20
Krankenhausentlassung
Incidence of combined
efficacy outcome* (%)
15 HR 0.33
• COVID-19-Pneumoinie und zusätzliche VTE-
(95 % CI 0.13 – 0.90)
Risikofaktoren (modifizierter IMPROVE-Score ≥ 4) P = 0.03
• Obligatorische Ultraschalldiagnostik der 10
Beinvenen und thorakale CT-Angiographie nach 9.4 %
35 ± 4 Tagen 5
• Primärer Wirksamkeitsendpunkt: VTE und VTE-
3.1 %
bedingter Tod
0
• Primärer Sicherheitsendpunkt: Schwere Control Rivaroxaban
Blutungen nach ISTH-Kriterien *Symptomatic and asymptomatic VTE, VTE-related death,
symptomatic ATE, myocardial infarction, non-hemorrhagic stroke,
• In beiden Gruppen keine schwere Blutung major adverse limb events, cardiovascular death
Ramacciotti et al. ESC 2021 (Late Breaking Science)
https://clinicaltrials.gov/ct2/show/NCT04662684Empfehlungen zur VTE-Prophylaxe und Antikoagulation bei COVID-19
Empfehlungen zur VTE-Prophylaxe und Antikoagulation bei COVID-19
Kluge et al. AWMF S3-Leitlinie. AWMF-Register-Nr. 113/001. Stand 17.05.2021Empfehlungen zur VTE-Prophylaxe und Antikoagulation bei COVID-19
Kluge et al. AWMF S3-Leitlinie. AWMF-Register-Nr. 113/001. Stand 17.05.2021Empfehlungen zur VTE-Prophylaxe und Antikoagulation bei COVID-19
• Bei massiver Entzündungsreaktion mit Ausbildung einer "Heparin-Resistenz" wird ein
zusätzliches Monitoring der Anti-Xa-Aktivität für UFH (Zielbereich: 0,3–0,7 IE/ml)
empfohlen.
• Als alternatives Antikoagulanz bei "Heparin-Resistenz" kann Argatroban zur Anwendung
kommen.
• Bei fortbestehender Immobilität, hoher entzündlicher Aktivität und/oder zusätzlichen
Risikofaktoren (z.B. BMI > 30 kg/m2, stattgehabte VTE, Thrombophilie, aktive
Krebserkrankung) ist nach Entlassung aus der stationären Behandlung eine prolongierte
ambulante NMH-Prophylaxe sinnvoll und dann im Arztbrief entsprechend zu
kommunizieren.
NMH Niedermolekulares Heparin
UFH Unfraktioniertes Heparin Modifiziert nach Langer et al. Hamostaseologie 2020; 40: 264-9Antikoagulation bei COVID-19 – Zusammenfassung
• Erhöhtes Risiko für thromboembolische Ereignisse (VTE > ATE) bei symptomatischer SARS-CoV-2
Infektion (COVID-19)
• Endothelzellaktivierung/-schädigung als wichtige Ursache der Hyperkoagulabilität
• Prophylaktische Antikoagulation nicht für alle Patienten ausreichend wirksam
• Therapeutische Antikoagulation mit NMH bei moderater Krankheitsaktivität von Nutzen
• Aktuelle Studienkonzepte zur Antikoagulation:
Normalstation
Ambulante Versorgung Normalstation ICU Poststationäre Versorgung
ICU
Prophylaxe vs. Prophylaxe vs. intensivierte Prophylaxe vs.
Placebo/Beobachtung Antikoagulation Placebo/BeobachtungHeparininduzierte Thrombozytopenie: Pathophysiologie + Diagnostik
PF4 + Heparin
Thrombozyt
Immunologischer Funktioneller
Nachweis (EIA) Nachweis
Screeningtest Bestätigungstest
IgG, IgA, IgM SRA
PF4 Plättchenfaktor 4
EIA Enzymimmunoassay
Stärke der Reaktion HIPA
SRA serotonin release assay
HIPA Heparininduzierte PlättchenaktivierungVakzin-induzierte immunthrombotische Thrombozytopenie (VITT)
Klinische Patientencharakteristika
Greinacher et al. N Engl J Med 2021; 384: 2092-101Labordiagnostik
Immunologischer Nachweis der VITT-Antikörper Funktioneller Nachweis der VITT-Antikörper
PF4 Plättchenfaktor 4
UFH Unfraktioniertes Heparin Greinacher et al. N Engl J Med 2021; 384: 2092-101Diagnostischer Algorithmus bei Verdacht auf VIPIT/VITT VIPIT Vakzin-induzierte prothrombotische Immunthrombozytopenie VITT Vakzin-induzierte immunthrombotische Thrombozytopenie
Diagnostischer Algorithmus bei Verdacht auf VIPIT/VITT
Falldefinition
• COVID-19-Impfung 4–42 Tage vor
Symptombeginn
• Jede venöse oder arterielle Thrombose
(häufig zerebral oder abdominell)
• Thrombozytopenie (< 150 × 109/l)
• Positiver PF4 "HIT" ELISA
• Deutlich erhöhte D-Dimere (> 2 mg/l)
Therapie
• Antikoagulation mit Verzicht auf
Heparin (z.B. Argatroban)
• IVIG (z.B. 1 g/kg über 2 Tage), ggf.
Kortikosteroide
• Vermeidung einer TK-Transfusion
• Ggf. Verlegung in spezialisiertes
Zentrum
https://www.hematology.org
https://www.isth.org
Oldenburg et al. Hamostaseologie 2021; 41: 184-9Zusammenhang zwischen klassischer HIT, Autoimmun-HIT und spontanen HIT-Syndromen
aHIT-Syndrome
• Ohne vorherige Heparin-
Exposition
• Antigen: PF4
- Spontaneous HIT syndrome
(z.B. nach Knie-TEP-OP, viraler
Klassische HIT oder bakterieller Infektion)
- Vaccine-induced immune
• Mit vorheriger Heparin-
thrombotic thrombocytopenia
Exposition
• Antigen: PF4/Heparin
- Typical-onset HIT Autoimmun-HIT (aHIT)
- Rapid-onset HIT • Mit vorheriger Heparin-
Exposition
• Antigen: PF4/Heparin & PF4
- Delayed-onset HIT
- Persisting (refractory) HIT
- Heparin "flush" HIT
- Fondaparinux-associated
HIT
HIT Heparininduzierte Thrombozytopenie
PF4 Plättchenfaktor 4
TEP Totalendoprothese Modifiziert nach Warkentin & Greinacher. Thromb Res 2021; 204: 40-51Vielen Dank für Ihre Aufmerksamkeit!
Sie können auch lesen

















































