Multimodale Kopfschmerzrehabilitation - INTERPROFESSIONELLE REHABILITATION SGNR-Symposium
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
SGNR-Symposium
INTERPROFESSIONELLE
REHABILITATION
Zürich, 03.11.18
Multimodale
Kopfschmerzrehabilitation
lic. phil. Monika Zemp PD Dr. med. Andreas Gantenbein
Leitende Neuropsychologin Chefarzt Neurologie
m.zemp@rehaclinic.ch a.gantenbein@rehaclinic.ch
Anna
Berta
Cristina
Spannungstypkopfweh
10
8
Intensität
6
• dumpf
• beidseitig diffus
4 • leicht-mittel
• keine Begleitsymptome
2
0
1 2 3 4 5 6 7 8
Zeit (Wochen)
Intensität
Episodische Migräne
• pulsierend
• einseitig
• Übelkeit/Erbrechen
• Photo-/Phonophobie
• Bewegung verstärkt
• 4-72 Stunden
• Trigger (Auslöser)
Zeit(w)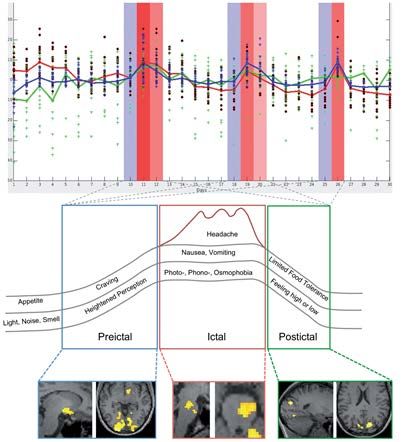
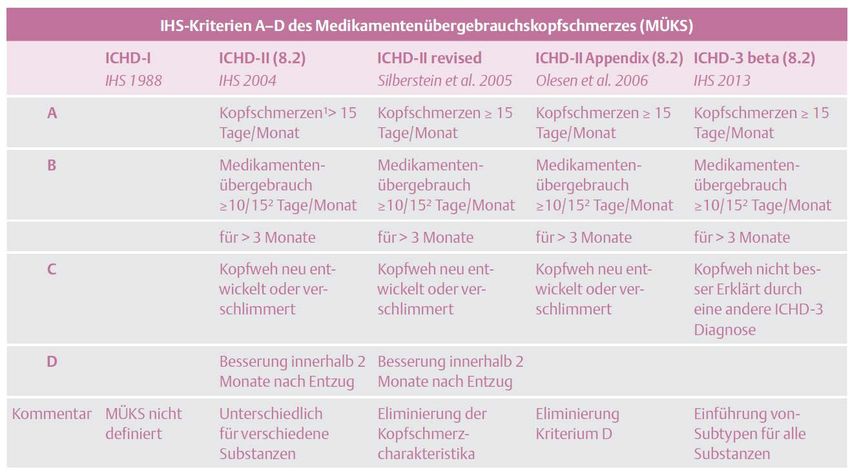
Medikamentenübergebrauchskopfschmerz
10
8
Intensität
6
• nahezu täglich
• eher dumpf-drückend
4 • attackenweise stark
• migräneartig
2
• Schmerzmittel >10 Tage
0 • 1% der Bevölkerung
4 8 12 16 20
Zeit(w)
Gantenbein in Agosti et al. 2015

MÜKs-Prävalenz bei
chronischen Schmerzpatienten
Wanner et al. J Headache and Pain 2013
Fallbeispiel
Anna
RehaClinic 7
Therapie

Migränetrigger
1207 Patienten
Kelman et al. Cephalalgia 2007n=1
Schulte et al. Brain 2016Aus: “ Migraine Headache Diseease” C.W. Theisler, 1990.
Martin studie …
Fallbeispiel
Berta
RehaClinic 13Entzug/Pause
Ambulant Stationär
• STOPP Kopfwehmittel am 1. Tag
• „cold turkey“
• Prednison 100mg/d über 5 Tage
• NSAR (z.B. Naproxen)
• aerobes Ausdauertraining
• Steroide (1mg/kg KG)
• Topiramat? • Beginn mit Prophylaxe
• anschl. Rehabilitation?Wann stationärer Entzug empfohlen?
• Nach erfolglosem ambulantem Entzug
• Bei langjährigem MÜKS
• Zusätzliche psychotrope Substanzen
(Barbiturate, Opioide, Schlafmittel, Anxiolytika)
• Bei ungünstigem sozialem Umfeld („Schwierige Umstände“)
• Komorbiditäten: Depression oder Angsterkrankung
• Bei posttraumatischen Kopfschmerzen, HWS-Distorsion?
Gantenbein & Sandor, Entzug und Therapie bei Medikamenten-Übergebrauchskopfschmerz (MÜKS). SAR 2009Entzug Rehabilitation
Zurzacher Kopfschmerzprogramm
(ZKP)
Entspannungs-
therapie
Physiotherapie Schmerz-
coaching
Ausdauer-
training Massage
TCMFallbeispiel
Cristina
RehaClinic 18Veränderungen vor und nach Medikamentenentzug
0.06
R T1 R T2 NR T1 NR T2
0.05
6 0.04
5 0.03
4 0.02
3 0.01
2 0
1 -0.01
0 -0.02
Riederer et al. WJBP 2012. -0.03
-0.04
05 1 15 2 25 3 35 4 45
x=-5 y=-35
midbrain
PAG
z=-8 6
T-score
5
4
3
2
1
0
Weiller et al. Nature Medicine 1995. Riederer et al. J Neurosci 2013.Demographie
(n=51)
Benz T, Gantenbein AR, Sándor PS et al. Medicine 2017Lebensqualität Benz T et al. Medicine 2017; Zebenholzer K et al. Clin J of Pain 2012
Outcome
Ansprechrate (Responderrate)
30
(n=51)
25
20 40
Kopfschmerztage vorher
35
15
30
Häufigkeit [%]
10 25
20
5
Kopfschmerztage nachher 15
0 10
1 6 11 16 21 26 31 36 41 46 51
5
0
75%
Kopfschmerzreduktion
Romano SK, Dissertation in prepAkupunktur
Kopfschmerzreduktion
ohne oder mit Akupunktur
0
ohne TCM mit TCM
-10
Kopfschmerzreduktion [%]
(n=27) (n=24)
-20
-30
-40
-50
-60
-70
-80 *
-90
* p = 0.015
-100
Romano SK, Dissertation in prepVergleich stationär vs. ambulant
de Goffau MJ et al. J of Pain 2017Anna
Prophylaxe mit
Candersartan
und Cipralex
Rückkehr in
Berta
privaten Prophylaxe mit
u beruflichen Valproat und Inderal
Alltag
neurol. u psychol
Einbau von Weiterbetreuung
Entspannung
(Yoga, Massage, stufenweiser
Zeichnen) Wiedereinstieg Beruf
Cristina
Akutmedikation Ibuprofen
Überweisung KJPD
Lösung der Wohnsituation
Rückkehr SchuleSie können auch lesen