Ablation von Lebertumoren: technische Möglichkeiten - Lukas Hechelhammer Interventionelle Radiologie KSSG St.Gallen - Euregio Bodensee Kongress
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Ablation von Lebertumoren: technische Möglichkeiten Lukas Hechelhammer Interventionelle Radiologie KSSG St.Gallen
∙ Überblick verschiedene Ablationsmodalitäten ∙ Radiofrequenzablation ∙ Mikrowellenablation ∙ Irreversible Elektroporation ∙ Techniken ∙ Evidenz ∙ HCC ∙ CRC ∙ Zukunft ∙ Radioablation ∙ Immunotherapie
∙ Überblick verschiedene Ablationsmodalitäten ∙ Radiofrequenzablation ∙ Mikrowellenablation ∙ Irreversible Elektroporation ∙ Techniken ∙ Evidenz ∙ HCC ∙ CRC ∙ Zukunft ∙ Radioablation ∙ Immunotherapie

RFA – MWA CryoA
IRE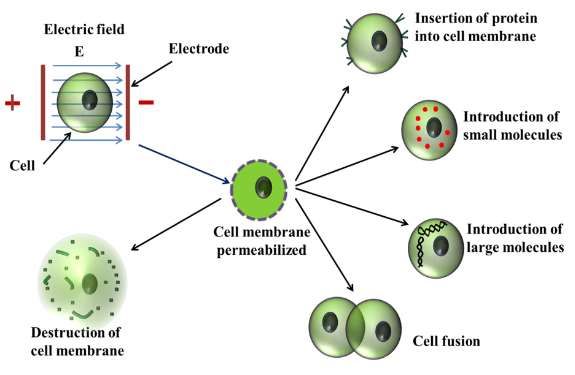
Radiofrequenzablation
420-500 kHz sinusoidaler Strom
Ionenbewegung
Reibungsenergie
Koagulationsnekrose
Hepatic ablation using Radiofrequency electrocautery
McGahan JP et al. Invest Radiol. 1990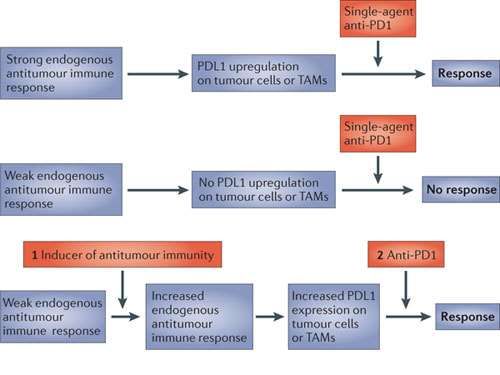
Mikrowellenzablation
Aufgrund des DIPOLS von H2O Molekülen beginnen diese im
Feld zu oszillieren
Reibungsenergie
Koagulationsnekrose
Microwave ablation: Principles and Applications
Simon C et al. Radiographics 2005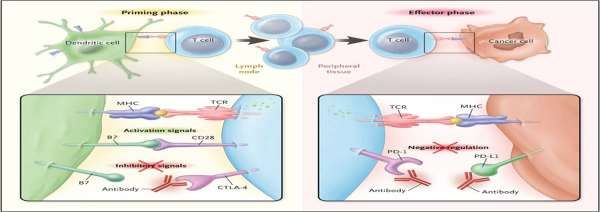
RFA MWA
RFA MWA

RFA MWA
+
∙ Generatoren weit verbreitet ∙ «aktives» Feld der Antenne
∙ Prediktive Ablationsgrösse ∙ Höhere Ablationstemperaturen
∙ Datenlage ∙ Sehr schnell
∙ Keine Neutralelektrode
∙
∙
Schmerzhaft
Darstellung des
Ablationsvolumens
_ ∙
∙
Schmerzhaft
Darstellung des
Ablationsvolumens
∙ Heat Sink ∙ Isolation der AntenneMWA oder RFA
∙ 76 MWA; 76 RFA
∙ Bis 3 HCC; max. 4cm Durchmesser
∙ Lokale Progression nach 2 Jahren
Efficacy of microwave ablation vs radiofrequency ablation: a randomised controlled phase 2 trial
Violi NK et al. Lancet 2018RFA vs. MW bei Lebertumoren
Metaanalyse
=
∙ Gesamtüberleben (1-5 Jahre)
∙ Lokale Rezidivraten
∙ Komplikationen
∙ MW kürzere Ablationszeiten – RCT beide gleich lange
Microwave Ablation Compared to Radiofrequency Ablation for Hepatic Lesions: A Meta Analysis
YR Hua et al. JVIR 2015Reversible Electroporation
Electroporation erhöht die Permeabilität der Zellmembranen
durch Änderung des transmembranen Potentials und ermöglicht
durch «Nano-Poren» den transmembranären Transport von
Molekülen
Electroporation based drug delivery
Santra T et al. Advances in Micro/Nano Electromechanical Systems 2013Irreversible Electroporation
Irreversible Electroporation führt durch die Applikation von
Hochspannungsfeldern zur irreversiblen Zellmembranschädigung
mit nachfolgender Apoptose der Zellen
Electroporation based drug delivery
Santra T et al. Advances in Micro/Nano Electromechanical Systems 2013+
∙ Kein «heat sink»
∙ Kollagengerüst bleibt erhalten
∙ Dünne Nadeln
∙
∙
Teuer
Parallele Ausrichtung der Nadeln _
∙ Vollständige Muskelrelaxation
∙ Thermische Schäden möglichKostenergleich (sFr)
RFA MWA IRE
Generator 45’000.- 45’000.- 400’000.-
Nadel 1500 - 3000.- 1500 - 3000.- 5000 - 6000.-IRE in HCC
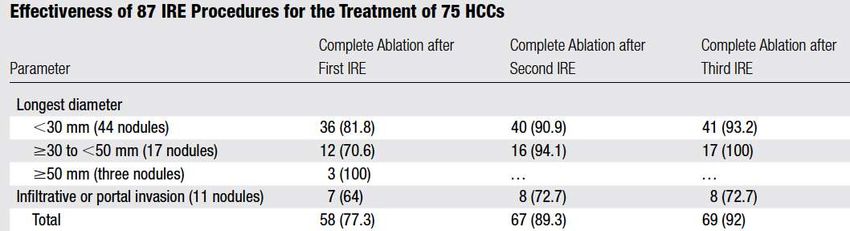
∙ 58 zirrhotische Patienten
∙ 75 HCC; mean 24mm Durchmesser (6-90)
∙ 48 aufgrund der Lokalisation, 10 aufgrund AZ
Safety and Efficacy of Irreversible Electroporation for the Treatment of HCC Not Amenable to Thermal Ablation Techniques
O. Sutter et al. Radiology 2017IRE in prim. und sek. Lebertumoren
∙ 29 Patienten; 43 Tumore
∙ 4 HCC; 4 CCC; 23 CRC; 12 Div.
∙ 6 ± 11.4 ml Tumorvolumen (˜2cm Durchmesser)
∙ Nähe < 5mm von PV, LV oder GW; N≤ 3; ≤ 4cm ∅
∙ 93% Komplette Ablation
∙ 11(33%) intrahep. Rezidiv: 2 Ablationsvolumen, 9 Nadeltrakt
∙ 25% der Ablation an PV → GW-Stenosen
Midterm Safety and Efficacy of IRE of Malignant Liver Tumors Located Close to Major Portal or Hepatic Veins
M.Distelmaier et al. Radiology 2017∙ Überblick verschiedene Ablationsmodalitäten ∙ Radiofrequenzablation ∙ Mikrowellenablation ∙ Irreversible Elektroporation ∙ Techniken ∙ Evidenz ∙ HCC ∙ CRC ∙ Zukunft ∙ Radioablation ∙ Immunotherapie
Ballonokklusion
RFA during percutaneous vein occlusion
De Baère T et al.; Radiology 2008Artifizeller Aszites
Percutaneous radiofrequency ablation of HCC with the use of artificial ascites. I.Song et al. Eur Radiol 2009
Artificial Ascites for Pain Relief During Microwave Ablation. A.Hakime et al. CVIR 2015Artifizeller Pneumothorax
18 Mt post RFA
Artificially Induced Pneumothorax for Percutaneous Transthoracic Radiofrequency Ablation of Tumors in the Hepatic Dome
De Baère T et al, Radiology 2005Coil-assistierte RFA
Coil-assisted RFA of poorly visible liver tumors. Farouil G et al.; CVIR 2014
RFA during percutaneous vein occlusion. De Baère T et al.; Radiology 2008Coil-assistierte RFA
8 Mt post RFA
Coil-assisted RFA of poorly visible liver tumors. Farouil G et al.; CVIR 2014
RFA during percutaneous vein occlusion. De Baère T et al.; Radiology 2008CEUS gesteuerte Ablation
∙ 55 Patienten
∙ 60 Tumore; 48 HCC, 12 Metastasen
∙ B-Bild nicht sichtbar (2 Radiologen)
∙ Follow-up 1 Jahr: 1 inkomplette Ablation
Radiofrequency ablation with CEUS
Dong Y. et al. Clin Radiol 2014∙ Überblick verschiedene Ablationsmodalitäten ∙ Radiofrequenzablation ∙ Mikrowellenablation ∙ Irreversible Elektroporation ∙ Techniken ∙ Evidenz ∙ HCC ∙ CRC ∙ Zukunft ∙ Radioablation ∙ Immunotherapie
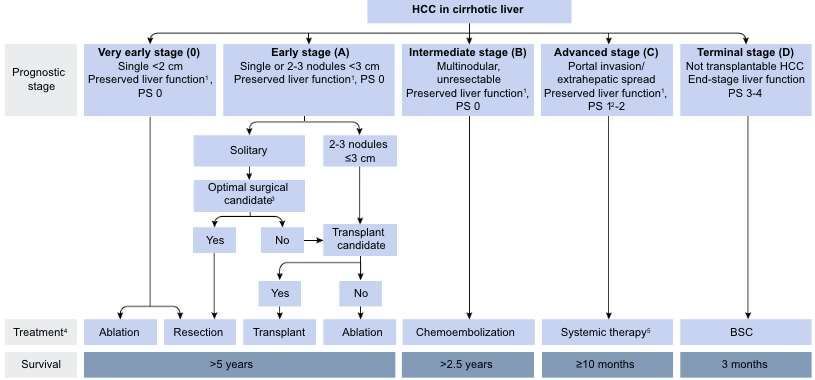
EASL Guidelines HCC J Hepatol 2018
Ablation beim frühen, resezierbaren HCC
∙ 4 RCT
∙ Kein Survivalbenfit nach max. Follow-up
∙ Mehr intrahepatische Rezidive nach Ablation
∙ AE und SAE mehr bei den chirurgischen Patienten
∙ Kürzere Hospitalisationszeiten nach Ablation
Management of people with early- or very early-stage hepatocellular carcinoma
Majumdar A et. al. Cochrane Database Syst Rev 2017RFA vs. RFA +TACE: HCC
Bridge to Transplant
Neoadjuvante Behandlung in Patienten welche schon für eine
TPL nach den akzeptieren Kriterien qualifizieren
∙ Vermindert „ dropouts“
∙ Verbessert Überleben nach OLT
∙ Prävention der Progression/Metastasen
∙ Exklusion von Patienten mit Progression
Is the treatment of HCC on the waiting list necessary? Majno P et al.
Liver Transplantation 2011Bridge to Transplant
TACE Ablation
Complete necrosis 27-50% 46-74%
Drop out rates 9-14% 0-21%
Survival benefits Limited evidence Limited evidence
Larger lesions Higher complete necrosis
Advantage
Multiple lesions rate
Lower complete necrosis
Disadvantage Seeding risk
rate
Cescon et al. J Hepatology 2013; Belghiti et al. Ann Surg Oncol 2008; Lencioni et al.
Hepatology 2010; Maddala et al. Liver Transpl 2004; Millonig et at. Liver Transpl 2007Erfahrung des Operateurs
∙ 2827 Patienten mit HCC
∙ RFA mit kurativer Intention
∙ Matched Pair Analyse
∙ je 406 Patienten ≤ 10 oder ≥ 79 RFA
Evaluation of the Effect of cumulative operator experience on hepatocellular carcinoma after RFA
Lee T et al Radiology 2015Kosteneffizienz: Resektion vs. RFA
Metaanalysis von 17 Studien
3996 Patienten Resektion
4424 Patienten RFA
1 Herd < 3cm RFA > Resektion
1 Herd >3-5cm Resektion > RFA
2-3 Herde < 3cm RFA > Resektion
Cost-effectiveness of hepatic resection versus percutaneous radiofrequency ablation for early hepatocellular carcinoma
Cucchetti A et al. J Hepatol. 2013Resektion vs. Ablation: CRC Metastasen:
RCT
Liver resection surgery versus thermal ablation for colorectal LiVer MetAstases
Gurusamy K et. al. Trials 2018Resektion vs. Ablation: CRC Metastasen
∙ Lokalrezidivraten nach WR oder RFA
∙ 103 Patienten; 221 Metastasen
∙ 43 WR; 60 RFA
∙ 23 bzw. 18.5 Mt follow up
∙ Lokalrezidive: WR 19% - RFA 10% p= 0.06
∙ WR: mehr Rezidive bei tiefen Tumoren, Kontakt zu
Gefässen
Local recurrence rate in patients with colorectal cancer liver metastasis after wedge resection or percutaneous RFA
Violi NV et al. Int.J Hyperthermia 2017RFA mit CX für nicht resezierbare CRC
Metastasen : Midterm survival (CLOCC)
overall survival
RFA (±Resektion) CX
n= 60 n=59
30 Mt Überleben 61.7% 57.6% ns
30 Mt tumorfreies Überleben 27.6% 10.6% p=0.025
RFA verlängert tumorfreies Überleben!
RFA combined with systemic treatment vs. systemic treatment alone in patients with non resectable colorectal liver metastases
Ruers T et al.; Ann Oncol. 2012RFA mit CX für nicht resezierbare CRC
Metastasen : Longterm survival (CLOCC)
RFA (±Resektion) CX
n= 60 n=59
Gesamtüberleben 45.6 Mt 40.5 Mt p=0.01
30 Mt Überleben 61.7 % 57.6 % ns
RFA verlängert Gesamtüberleben!
RFA combined with systemic treatment vs. systemic treatment alone in patients with non resectable colorectal liver metastases
Ruers T et al.; JCO 2015Rezidive nach Ablation
∙ Metastasen grösser 3 cm
∙ Periläsionärer Ablationssaum > 5mm bzw. > 10mm (A0)
∙ MWA oder RFA
∙ RAS Status; LR nach 3 Jahren
∙ Mutiert 39%
∙ Wild-Typ 14%
Local tumour progression after percutaneous ablation of colorectal liver metastases according to RAS mutation status
Odisio BC et al. Br J Surg 2017
Percutaneous Microwave versus RFA of Colorectal Liver Metastases: Ablation with Clear Margins (A0)
Shady W. et al. JVIR 2018
Percutaneous Radiofrequency Ablation of Colorectal Cancer Liver Metastases- Factors Affecting Outcomes
Shady W. et al. Radiology 2016∙ Überblick verschiedene Ablationsmodalitäten ∙ Radiofrequenzablation ∙ Mikrowellenablation ∙ Irreversible Elektroporation ∙ Techniken ∙ Evidenz ∙ HCC ∙ CRC ∙ Zukunft ∙ Radioablation ∙ Immunotherapie
TARE (transarterielle Radioembolisation)
∙ Sehr kleine Beads (30 µm)
∙ β- Strahler; 2mm Eindringtiefe im Gewebe; HWZ: 2.5Tg
∙ Portalvenenthrombose keine Kontraindikation
∙ rel. teuer (Dosis Leber ca. 15-20‘000 sFr)
∙ Meist milde AE (1/2)
GI-Ulzerationen 3.5%
Leberversagen REILD 0.5-1%
Bauchschmerzen 30-40%
Übelkeit 25-30%
Multicenter evaluation of the safety and efficacy of radioembolization in patients with unresectable colorectal liver metastases
Kennedy A et al. J Gastrointest. Oncol. 2015Radiation Segementektomie ∙ Segmentale Applikation der Sphären ∙ Sehr hohe lokale Dosis: «ablative Dosis»
Radiation Segementectomie: HCC
∙ 101 Patienten
∙ Nicht resezierbare solitäre HCC bis 5cm; keine RFA
∙ 47% CR, 39% SD
∙ TTP: 33 Monate
∙ 33 transplantiert (52% komplette, 48% partielle Nekrose 50-99%)
∙ Nekrose ist abhängig von der applizierten Dosis
Unresectable Solitary Hepatocellular Carcinoma Not Amenable to Ablation: Survival of Radiation Segmentectomy
Vouche M. et al. Hepatology 2014Radiation Segementektomie: HCC
∙ 112 Patienten
∙ Nicht resezierbare solitäre HCC bis 3cm; keine RFA
∙ Matched Kohorten: 38 Patienten je Arm
RECIST CR, PR, SD, PD
∙ RS 81%, 11%, 2%, 6%
∙ TACE 49%, 28%, 14%, 9%
Radiation Segmentectomy versus Selective Chemoembolization in the Treatment of Early-Stage Hepatocellular Carcinoma
Biedermann D. et al. JVIR 2018Radiation Segementektomie: Metastasen
∙ 10 Patienten
∙ Nicht resezierbare, Metastasen max. 2 Segmenten
∙ 7 CRC, 1 Mamma, 1 Leimyosarcom, 1 NEC
∙ 40% CR, 40% SD, 20 PD bzgl. behandelte Läsionen (7 Monate)
Safety and initial efficacy of radiation segmentectomy for the treatment of hepatic metastases
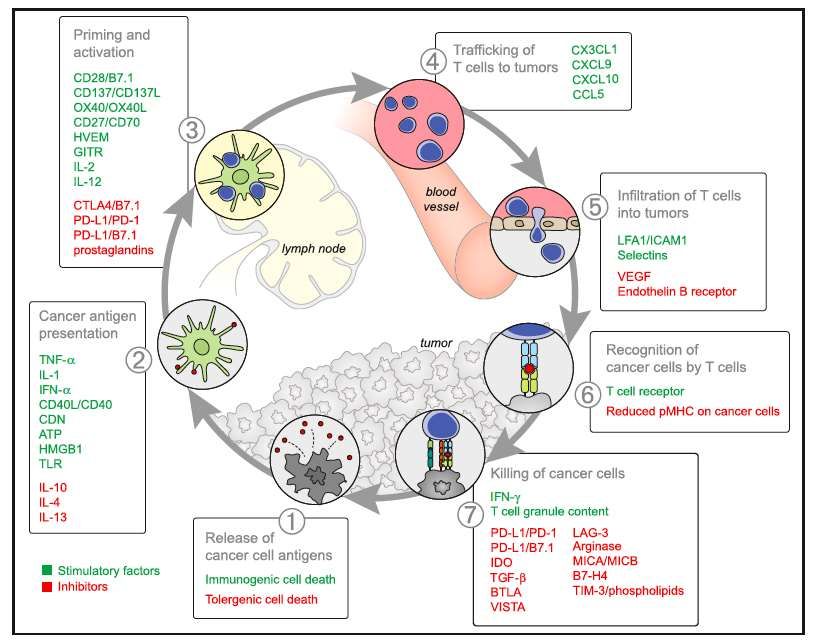
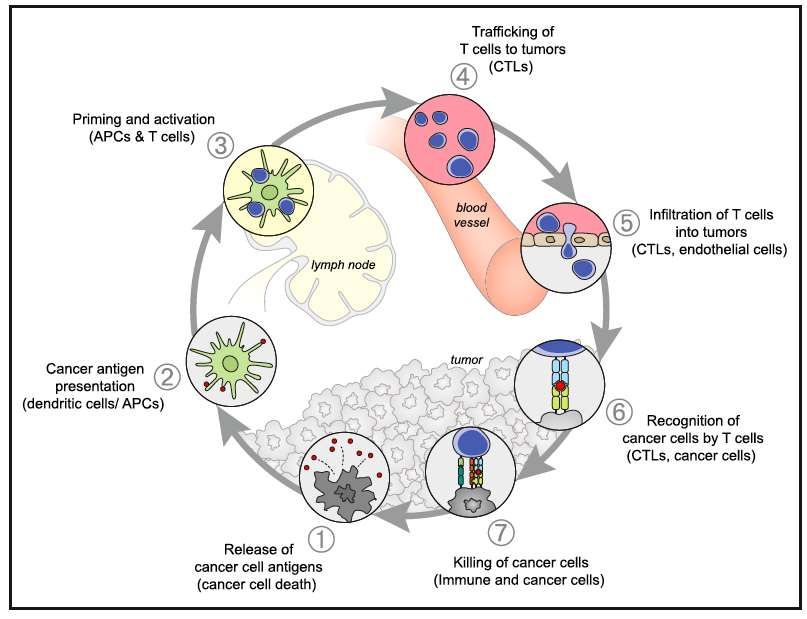
JGO 2018Cancer Immunity Cycle
Oncology meets Immunology: the cancer immunity cycle
Chen DS et al. Immunity 2013Adaptive Immune Resistenz
The blockade of immune checkpoints in cancer immunotherapy
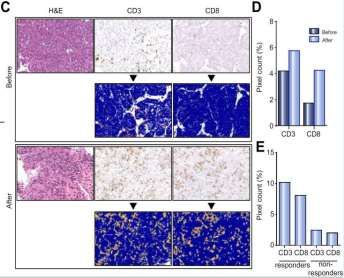
Pardoll DM et al. Nature 2012Ablation + Antikörper gegen CTLA-4
∙ 32 Patienten; 75% BCLC C, multifokal
∙ Inkomplette RFA einer Läsion bzw. C-TACE
∙ 25% PR
∙ 12/14 HCV Virusloadreduktion
∙ TTP 7.4 Monate (beide Gruppen)
Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma
A.G. Duffy et al. J Hepatol 2017Systemische pro-onkogene Effekte
nach Ablation
Targeting STAT3 to Suppress Systemic Pro-Oncogenic Effects from Hepatic Radiofrequency Ablation
Kumar G. et al. Radiology 2018Zusammenfassung RFA = MWA IRE in bestimmten Situationen Verschiedene Techniken erlauben AO Ablationen HCC: etablierte kurative Methode CRC: nicht resezierbare Metastasen Radioablation: Alternative bei „solitären“ Läsionen Immunotherapie in Kombination mit Ablation
DANKE!
Sie können auch lesen