Clemens Wendtner COVID-19: Therapien und Behandlungsoptionen
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
COVID-19: Therapien und Behandlungsoptionen
Clemens Wendtner
Chefarzt
München Klinik Schwabing
Klinik für Hämatologie, Onkologie, Immunologie,
Palliativmedizin,Infektiologie und Tropenmedizin
Akad. Lehrkrankenhaus
Ludwig-Maximilians-Universität (LMU)
München
BMG, Fachgespräch zur Vorbereitung etwaiger Maßnahmen zur Bekämpfung einer 4. Coronawelle, 19.07.2021
Zulassung: COVID-19-Pneumonie mit O2-Pflichtigkeit
bei Patienten >12 Jahre und >40 kg KG über 5-10 Tage
Remdesivir
Benefit: Frühestmögliche Gabe nach Eintritt
O2-Pflichtigkeit und nicht über virale Phase hinaus
Zulassung: Schwere COVID-19 Infektionen mit Sauerstoff-
Therapie bei Patienten >12 Jahre und >40 kg
Dexa-
Benefit [RECOVERY-Studie]: Beginn erwägen bei dynamischer
methason Verschlechterung; Benefit bei invasiver Beatmung größer als
bei O2-Gabe/nicht-invasiver Beatmung
High-Flow-O2-
Keine
Gabe (ggf. nicht Invasive
respiratorische O2-Gabe ECMO
–invasive Beatmung
Unterstützung
Beatmung)
Benefit:
- asymptomatische/
oligosymptomatische Pat. mit
Risikofaktoren und ≤ 7 Tage seit
mAB Symptombeginn/ max. 72h seit
pos. Test
- Seronegative hospitalisierte Pat.
mit max. Low-Flow-O2
Benefit bei
dynamischer
Verschlechterung
trotz
Tocilizumab* Dexamethason
mit ausgeprägter
pulmonaler * Gabe nur in Kombination mit
Hyperinflammation Dexamethason
Stand 15.07.2021
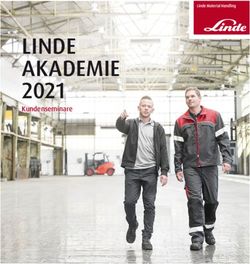
Tabelle 2: Übersicht zu möglicher Indikationsstellung und
Einschränkungen der Therapie mit Remdesivir
Indikationsstellung
Nicht empfohlen4 Kontraindikationen4
(alle Kriterien erfüllt)
Patienten ohne
COVID-19-Pneumonie Sauerstoffbedarf, Niereninsuffizienz
Erwachsene und Sauerstoffpflichtigkeit CAVE: AF > 30/min3 (GFR < 30ml/min)
Jugendliche (> 12 Symptomdauer 30/min können trotz noch ausreichender SpO 2 bereits sauerstoffpflichtig sein
4Bei Erwägung einer Therapie unbedingt vorab infektiologische Beratung über das Infektiologie-Beratungsnetzwerk des STAKOB
gemeinsam mit der DGI (www.rki.de/stakob-ibn)
Stand 15.07.2021
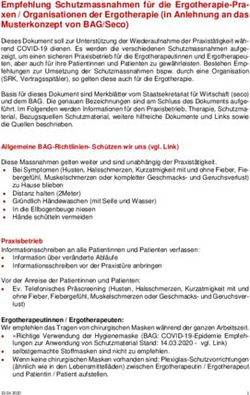
RECOVERY trial: Casirivimab & Imdevimab in hospitalized patients (Phase 3)
Main randomisation
Trial Design* Baseline Characteristics
Part A: dimethyl fumarate, Well balanced between treatment arms
Cas/im 8,000 mg IV +
corticosteroids or IV Ig • Adults and
adolescents (>40 kg)
usual care Seronegative All patients
Part B: nAbs R
• SARS-CoV-2 infection 1:1
or N=3,153 (34%) N=9,785
Follow-
Part C: aspirin • Hospitalized patients Usual care§† up period Median age 62 years
• No serious risk factors** 6 months
Part D: baricitinib vs • No IV Ig during current >90% of all patients
infliximab admission Primary endpoint received corticosteroids
Part E: high dose All-cause mortality within 28 days of randomization Days since symptom onset:
corticosteroids ○ In seronegative patients (hierarchy #1) 63% male
Second randomization ○ In all patients (hierarchy #2)
Patients with clinical
Tocilizumab vs usual care
7 9
progression
(until Jan 2021)
Results
Reduced risk of death by 20% in seronegative patients Reduction of hospital stay duration Reduction in risk of ventilation
– (absolute benefit 24% vs 30%) in seronegative patients in seronegative patients
35 Seronegative patients
Use of ventilation
Rate ratio, 0.80 (0.70–0.91) Usual care
Cas/im +
Duration of hospitalisation
30
P=0.0010 by log-rank test usual care 28%
25 13% reduction
Mortality, %
Cas/im + 355/1,267 RR 0.87 (0.77, 0.98)
13 days
20 usual care
Cas/im + Usual care 32%
15 usual care N=1,633 Reduction 370/1,14
by 4 days
Non-invasive
10 3
ventilation
27%
Usual care 17 days 15% reduction
5 341/1,267
RR 0.85 (0.75, 0.97)
0 N=1,520 31%
0 7 14 21 28 360/1,143
Days since randomisation
mechanical
ventilation
7%
Invasive
• Benefit of cas/im in seronegative patients seen across all patient subgroups, • No difference in risk of death, hospital duration or ventilation 89/1,267 33% reduction
including those with respiratory support within the overall study population RR 0.67 (0.52, 0.88)
• If treated with usual care only, seronegative patients had twice the risk of 10%
death of seropositive patients (30% vs 15% mortality)
119/1143
• No significant difference in 28-day mortality seen in all and seropositive patients
*Patients with clinical progression in Parts A, B and C could be considered for a second randomisation to tocilizumab until Jan 2021. A single participant could be randomised at
most to 1 arm from each of part A, B, C, D and E of the factorial randomisations (depending on location), and thus receive between 0 and 4 treatments on top of usual standard
of care; **Defined as medical history that might put the patient at significant risk. §Until 15 Jan 2021, patients were also randomised to receive convalescent plasma + usual
care, however, recruitment to this arm was stopped due to lack of efficacy; †As determined by participating hospital; Ig, immunoglobulin; IV, intravenous; RR, rate ratio Horby PW, et al. medRxiv 2021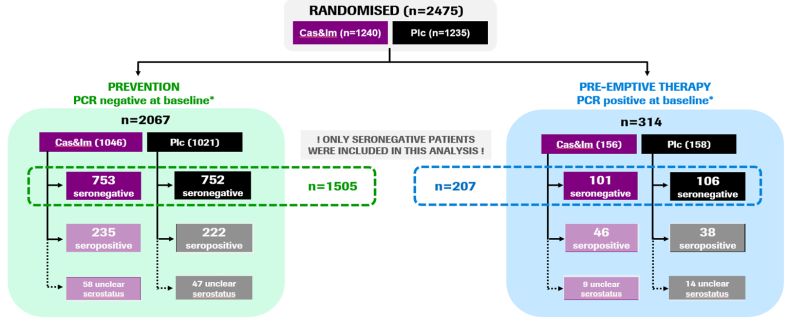
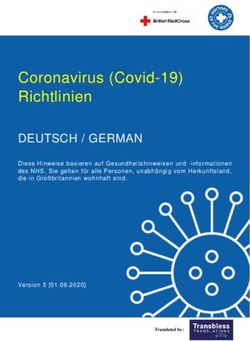
Study 2067: Casirivimab & Imdevimab in ambulatory patients (Phase 3)
Original PhIII protocol Amended PhIII protocol
Study Design Baseline characteristics
▪ Ambulatory patients Cas&Im 2,400 mg IV Cas&Im 2,400 mg IV Baseline characteristics in high-risk patients were well balanced
with COVID-19 or or All patients had at least one risk factor, including:
▪ Aged ≥18 years R Protocol update
Cas&Im 8,000 mg IV Cas&Im 1,200 mg IV
▪ Positive for SARS- 1:1:1
CoV-2 or • Dosing change or
• All patients Mean age
▪ N=4,567 Placebo IV Placebo IV
required to have
Primary endpoint Patients with or 50 years Obesity Cardiovascular Age ≥50 years
≥1 risk factor for 58% 51%
▪ COVID-19-related hospitalisations or without risk Only patients with disease
severe COVID-19 36%
all-cause deaths through Day 29 factors risk factors
Results
Cas&Im reduced the risk of hospitalisation or death by ~70% Reduced duration of symptoms by 4 days compared to placebo Additional results
Time to resolution of COVID-19 symptoms* • Cas&Im reduced viral
Patients with ≥1 COVID-19-related hospitalisation or death through Day 29
load at Day 7 compared
1,200 mg IV Placebo 2,400 mg IV Placebo Placebo 14
to placebo across doses
n=736 n=748 n=1,355 n=1,341 and regardless of
baseline viral load
n (%) 7 (1.0) 24 (3.2) 18 (1.3) 62 (4.6) –4 days
1,200 mg IV 10 p
Therapie-Indikationen und Zeitpunkt für die Therapie mit
neutralisierenden monoklonalen Antikörpern
Zeitpunkt Antikörperstatus bevorzugte mAB
Ambulante Patienten ≤ 7 Tage seit Symptombeginn Innerhalb des genannten 1) Casirivimab 1,2g /
(asymptomatisch bzw. milde bis Zeitfensters ist ein negativer Imdevimab 1,2g i.v.
moderate Symptome) und Max. 72 Stunden nach dem Antikörperperstatus anzunehmen.
Vorliegen von Risikofaktoren für positiven PCR-Test Die Antikörper (Anti-Spike)
einen schweren Verlauf können abgenommen werden, 2) Bamlanivimab 700mg /
das Ergebnis soll aber nicht Etesevimab 1,4 g i.v.
abgewartet werden (Zeitfaktor)
Nosokomiale Infektion, Patienten Max. 72 Stunden nach dem Innerhalb des genannten 1) Casirivimab 1,2g /
asymptomatisch bzw. milde bis positiven PCR-Test Zeitfensters ist ein negativer Imdevimab 1,2g i.v.
moderate Symptome und Antikörperperstatus anzunehmen.
Vorliegen von Risikofaktoren für Die Antikörper (Anti-Spike)
einen schweren Verlauf können abgenommen werden, 2) Bamlanivimab 700 mg
das Ergebnis soll aber nicht / Etesevimab 1,4g i.v.
abgewartet werden (Zeitfaktor)
Hospitalisierte Patienten mit ≤ 7 Tage seit Symptombeginn Innerhalb des genannten Casirivimab 4g / Imdevimab
COVID-19-Pneumonie (max. Low- Zeitfensters ist ein negativer 4g i.v.
Flow-Sauerstoffsubstitution) Antikörperperstatus anzunehmen.
Die Antikörper (Anti-Spike) sollen
abgenommen werden, das
Ergebnis soll aber nicht
abgewartet werden (Zeitfaktor)
Hospitalisierte Patienten mit > 7 Tage nach Symptombeginn Antikörper (bevorzugt Anti-Spike- Casirivimab 4g / Imdevimab
COVID-19-Pneumonie (max. Low- IgG) sollen abgenommen werden. 4g i.v.
Flow-Sauerstoffsubstitution) Gabe von mAB nur bei
tagesaktuellem negativem
Antikörperstatus
Hospitalisierte Patienten mit
COVID-19-Pneumonie und High-
Flow-Sauerstoffsubstitution oder Keine Indikation zur Therapie mit monoklonalen Antikörpern
NIV oder IMV Stand 15.07.2021
Anil Gupta et al., medRxiv preprint doi: https://doi.org/10.1101/2021.05.27.21257096
Bei Patienten mit Hochrisikofaktoren, insbesondere Patienten mit B-Zell-depletierender Therapie und
Verdacht auf unzureichende eigene spezifische SARS-CoV-2-Antikörper-Produktion kann ein Einsatz auch in
der späteren Krankheitsphase erwogen werden, insbesondere bei hoher Viruslast. In dieser Situation
sollten die Anti-Spike-Antikörper abgenommen werden, der Befund muss jedoch nicht abgewartet werden.
Zusätzlich sinnvoll könnte eine Anwendung im Rahmen einer Post-Expositionsprophylaxe, z.B. bei
nosokomialen Ausbruchgeschehen, sein. Studienergebnisse hierzu stehen noch aus, daher ist eine
Empfehlung aktuell noch nicht möglich.
Die Möglichkeit allergischer Reaktionen auf die genannten monoklonalen Antikörper ist in Betracht zu
ziehen, so dass ihre Anwendung nur unter engmaschiger klinischer Kontrolle erfolgen sollte.
Die neutralisierenden monoklonalen Antikörper werden als einmalige intravenöse Infusion (Infusionsdauer
≥ 1 h mit Nachbeobachtung ≥ 1 h) mit gleichzeitiger Infusion der 2 Kombinationspartner verabreicht.
Stand 15.07.2021Study 2069: Casirivimab & Imdevimab for post-exposure prophylaxis (Phase 3)
Phase 3 Study 2069: Design Two study cohorts
▪ Adults and adolescents Prevention cohort
Cas&im 1,200 mg SC
▪ Asymptomatic HHCs PCR-negative at baseline
R Follow-up
▪ OwH and living with an IP with or
a SARS-CoV-2 diagnosis 1:1 (7 months)
Pre-emptive therapy cohort
▪ Randomisation within Placebo SC
PCR-positive at baseline
96 hrs of IP’s positive
SARS-CoV-2 test sample Single-dose*
N=2,475 Primary endpoint: efficacy of Cas&imd vs placebo in
EAP (1 month) preventing symptomatic SARS-CoV-2 infections
Results
PREVENTION COHORT PRE-EMPTIVE THERAPY COHORT
81% reduction in 31% reduction in development of Generally well tolerated
symptomatic infections Additional results symptomatic disease in HHCs with no unexpected safety signals
infected at baseline
Prevention cohort
• 66% reduction in all infections
HHCs who developed Infected HHCs who
symptomatic infection (symptomatic and developed symptoms n (%) Placebo (N=1,306) Cas&im (N=1,311)
asymptomatic)
AEs 379 (29) 265 (20)
7.8% • In those HHC who still 42% SAEs 15 (1) 10 (1)
(59/752) became infected, Cas&im (44/104)
prophylaxis resulted in 86% ISRs (grade 1/2) 19 (2) 55 (4)
81% 31%
reduction of patients with high reduction Pre-emptive therapy cohort
reduction
viral load and significantly (p=0.0380)
(pMARMs
Sie können auch lesen