Presented / commented by Arnold von Eckardstein, Institut für Klinische Chemie, Unispital Zürich - colada
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Presented / commented by Arnold von Eckardstein, Institut für Klinische Chemie, Unispital Zürich
Conflicts of Interest by Arnold von Eckardstein
Honoraria (consulting): Amgen
Sanofi-Aventis
Research funding: University of Zurich
European Commission
Hartmann-Müller-Foundation
Novartis Foundation
Swiss National Science Foundation
Swiss Heart Foundation
Engagement in scientific bodies: European Atherosclerosis Society
(Secretary, Editor-in-Chief Atherosclerosis)
Swiss Atherosclerosis Society
(Executive Committee Member, Past President)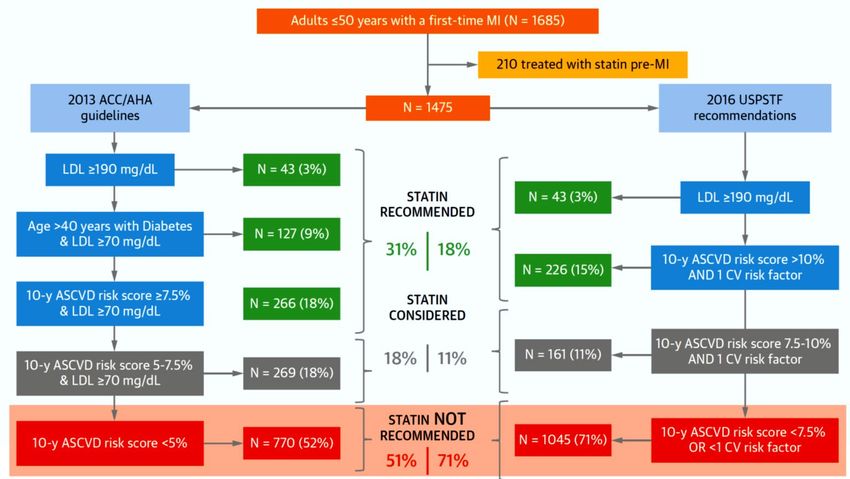
ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention andere Lipid-Risikofaktoren
Rationale der Dyslipidemia Guidelines:
Kausalität zwischen Lipoproteinen und Atherosklerose
Risikofaktoren/ Beobachtungs- Interventionstudien Genetische Tiermodelle
Risikomarker studien Studien
ja
LDL-Cholesterin ja (Statine, Ezitimibe, ja ja
PCSK9-Hemmer)
Nein
(CETP-Hemmer)
oder Subgruppen Abhänig vom
HDL-Cholesterin ja
(Niacin, wenn ohne Statine; veränderten
nein
Fibrate, wenn HDL-C niedrig Gen
& Triglyzeride erhöht)
Ja: (Eicosapentaensäure
hochdosiert)
Nein (Omega-3-Fettsäuren
allgemein) Abhänig vom
Triglyzeride ja
oder Subgruppen ja veränderten
(Niacin, wenn ohne Statine; Gen
Fibrate, wenn HDL-C niedrig
& Triglyzeride erhöht)
Lipoprotein(a) ja Nicht untersucht ja ja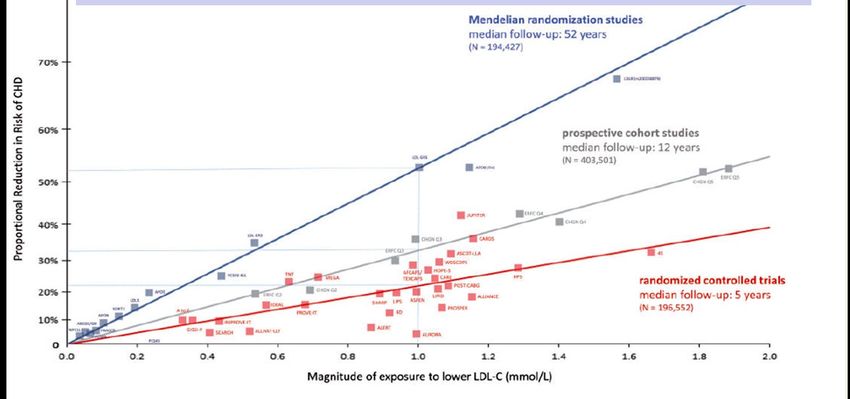
LDL-Cholesterin ist kausaler Risikofaktor für Atherosklerotische kardiovaskuläre Krankheiten Eur Heart J 2017;38:2459
Grundsatzprinzip der Dyslipidemia Guidelines
Die absolute Risikoreduktion
hängt ab vom ASCVD-
Risiko des Patienten und der
absoluten LDL-C Senkung:
Adaptiere
Behandlungsintensität ans
Risiko
Intensiviere Behandlung bei
steigendem Risiko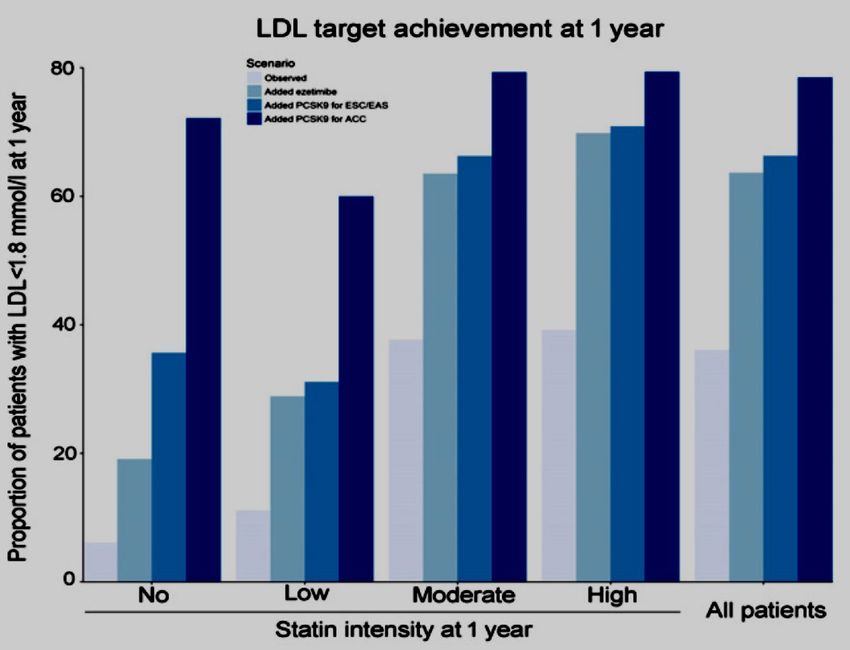
Kardiovaskuläre Risikokategorien
The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and
European Atherosclerosis Society (EAS) Mach et al. Eur. Heart J 2019 or Atherosclerosis 2019; übersetzt in SMF 2020 in press )
• ASCVD (klinisch manifest oder durch Bildgebung nachgewiesen)
• SCORE ≥10%
• FH mit einem grossen Risikofaktor
sehr hohes Risiko
• Schwere NI (eGFR 20 Jahre)
• SCORE ≥5% und 8 mmol/l
oder LDL-C >4.9 mmol/l oder BD ≥180/110 mmHg
hohes Risiko • FH ohne weitere Risikofaktoren
• Moderate NI (eGFR 30-59 ml/min)
• DM ohne Endorganschaden, aber Dauer 10-20 Jahre oder Vorhandensein
eines zusätzlichen Risikofaktors
• SCORE ≥1% und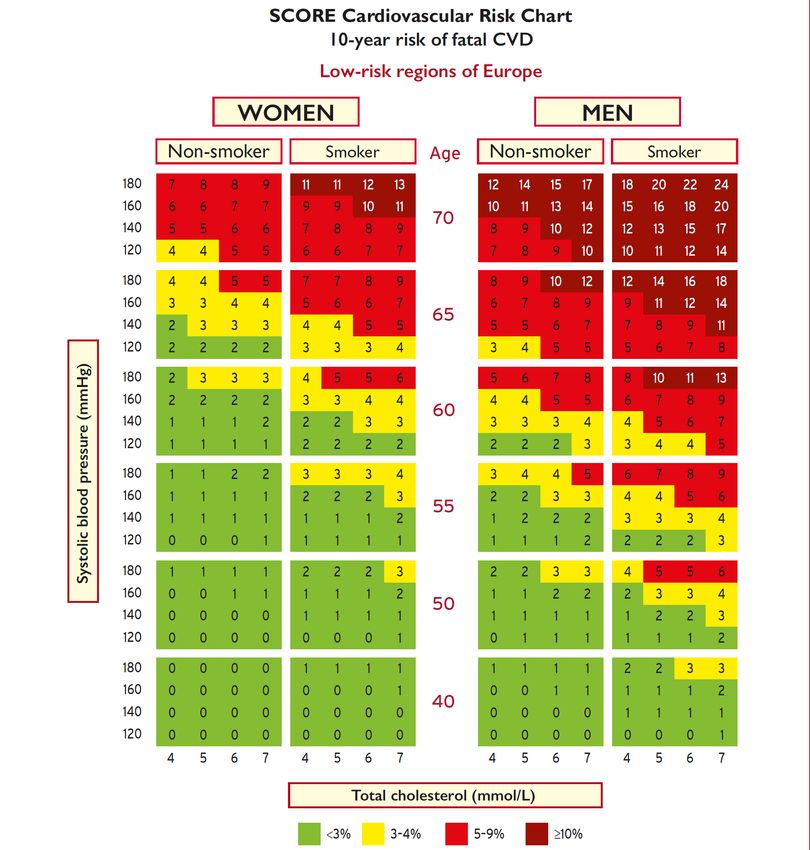
Empfohlene Behandlungsziele für LDL-Cholesterin:
wichtigste Änderungen 2019 vs. 2016
LDL—C-Zielwerte (Start mit unbehandeltem LDL-C)
Risiko-Kategorie
2016 2019
50%↓,
sehr hoch 50%↓
falls LDL-C 1.8-3.5 mmol/l
50%↓,
hoch 50%↓
falls LDL-C 2.6-5.2 mmol/l
moderat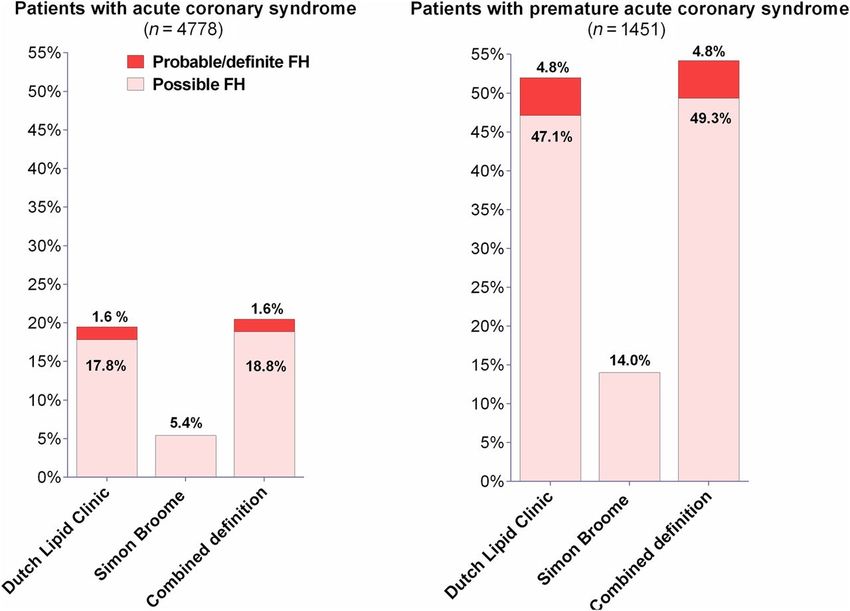
Intensification of LDL-C treatment goals:
Evidence from outcome trials
.
200
WOSCOPS
LDL cholesterol (mg/dl)
4S
150
LIPID AFCAPS
CARE
FOURIER HOPE-3
HPS
100
IDEAL
JUPITER
TNT
IMPROVE-IT
Outcomes
ODYSSEY
50
0
1995 2000 2005 2010 2015 2020
Year
Packard, EAS 2019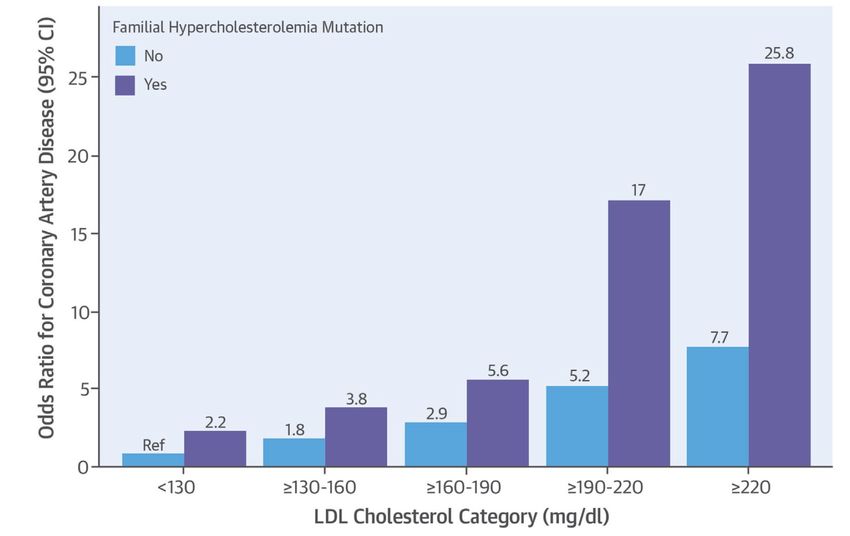
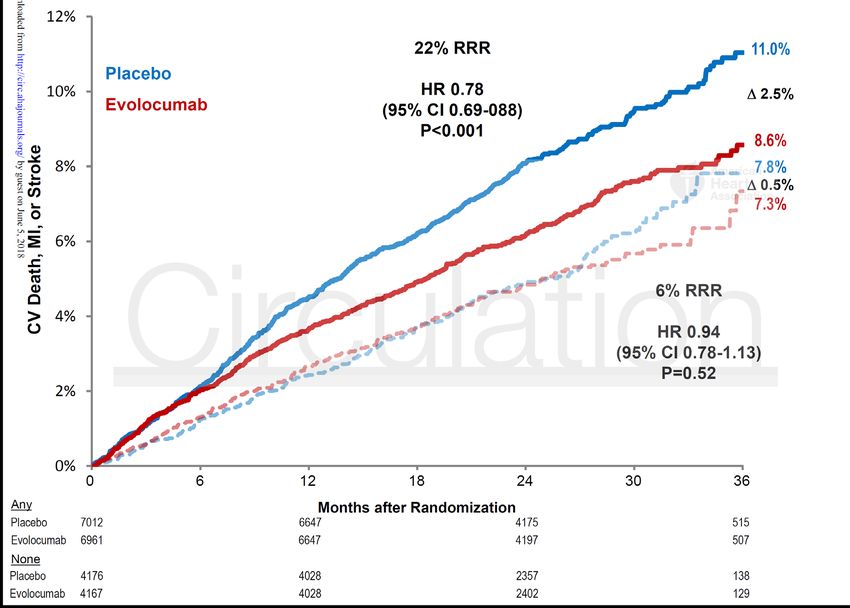
Risk reduction continues even at very low levels without threshold : No J curve FOURIER: Evolucumab 10 ODYSSEY trials: Alirocumab Lancet. 2017;390:1962-1971 Circulation. 2016;134:1931
Intervention strategies as a function of total cardio- vascular risk and untreated LDL- cholesterol levels Mach, Baigent, Catapano et al. European Heart Journal (2019)
Treatment algorithm for pharmacological lowering of LDL-cholesterol Mach, Baigent, Catapano et al. European Heart Journal (2019)
ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention
ESC/EAS 2019 Recommendations for treatment
goals for LDL cholesterol in secondary prevention
Mach, Baigent, Catapano et al. European Heart Journal (2019)ESC/EAS 2019 Recommendations for treatment
goals for LDL cholesterol in secondary prevention
Mach, Baigent, Catapano et al. European Heart Journal (2019)PCSK9-Inhibitoren in der Sekundärprävention:
Wichtigste Diskrepanzen zwischen ESC/EAS2019
Empfehlungen und BAG-Limitatio in CH
ESC/EAS* BAG Limitatio für CH**
Definition ASCVD klinische manifest Nur klinisch manifeste
Sekundärprävention oder durch imaging ASCVD
für PCSK9i Indikation nachgewiesen
Indikationsschwelle > 1.4 mmol/L (> 1.0 mmol/L) > 2.6 mmol/L trotz maximal
LDL-Cholesterin trotz Statine + Ezitimibe tolerierter Statine
Testung von Ezitimibe empfohlen fakultativ
*: Mach, Baigent, Catapano et al.
European Heart Journal (2019) or Atherosclerosis (2019) **: Spezialitätenliste des
www.escardio.org/guidelines or Bundesamt für Gesundheit,
https://www.eas-society.org/page/dyslipidemia_guide_2019 http://www.spezilitätenliste.chFOURIER: Clinical Benefit of Evolocumab by Severity and Extent of
Coronary Artery Disease:
Cumulative incidence curves in patients stratified by presence or
absence of at least one high-risk feature*
*: having one of the
following: High risk
- Previous MI < 2 years group
- >2MI’s in history
- Multivessel disease low risk group
Sabatine et al. 2018
Circulation in pressHigher Baseline LDL-Cholesterol Associated with
Greater Alirocumab Benefit on Total Events
• 255 fewer total events with
alirocumab among 5,629
patients with LDL-C ≥100
mg/dL at baseline
• 130 fewer total events with
alirocumab among 13,295
patients with LDL-CAverage LDL cholesterol lowering reached by
different pharmacological regimens
Untreated Untreated
LDL-C to LDL-C to
reach reach
LDL-C LDL-C
< 1.4 < 2.6
mmol/L mmol/L
< 2.0 < 3.7
< 2.8 < 5.2
< 4.0 < 7.4
< 3.5
< 5.6
< 9.3
Mach, Baigent, Catapano et al. European Heart Journal (2019)SPUM-ACS: Proportion of Swiss CHD patients
reaching recommended LDL-C targets (1.8 mmol/L)
1 year after ACS
2024 patients,
94.3% with statin,
5.8% with ezetimibe
Gencer et al.
J Am Heart Assoc. 2017;6:e006537ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention Familiäre Hypercholesterinämie Risikoschätzung ältere Menschen junge Menschen
Kardiovaskuläre Risikokategorien
The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and
European Atherosclerosis Society (EAS) Mach et al. Eur. Heart J 2019 or Atherosclerosis 2019; übersetzt in SMF 2020 in press )
• ASCVD (klinisch manifest oder durch Bildgebung nachgewiesen)
• SCORE ≥10%
• FH mit einem grossen Risikofaktor
sehr hohes Risiko
• Schwere NI (eGFR 20 Jahre)
• SCORE ≥5% und 8 mmol/l
oder LDL-C >4.9 mmol/l oder BD ≥180/110 mmHg
hohes Risiko • FH ohne weitere Risikofaktoren
• Moderate NI (eGFR 30-59 ml/min)
• DM ohne Endorganschaden, aber Dauer 10-20 Jahre oder Vorhandensein
eines zusätzlichen Risikofaktors
• SCORE ≥1% undRecommendations for the detection of
patients with heterozygous familial hypercholesterolemia
Recommendations Class Level
It is recommended to consider the diagnosis of FH in patients with CHD
aged 190 mg/dL], in children >4 mmol/L [>150 mg/dL]), and
in first-degree relatives of FH patients.
©ESC
It is recommended that FH should be diagnosed using clinical criteria and
confirm, when available, with DNA analysis. Family cascade screening once I C
index case is diagnosed is recommended.
2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce
www.escardio.org/guidelines
cardiovascular risk (European Heart Journal 2019 -doi: 10.1093/eurheartj/ehz455)http://www.agla.ch/familiare-hypercholesterinamie/diagnostik-bei-erwachsenen
1
1
2
2
2
2
1
6
4
8
5
3
1
Mutationsnachweis in LDLR, APOB1, PCSK: 8
https://www.fhscore.eu/#/landing
Eur Heart J 2013; 34, 3478–3490;
Eur Heart J 2013; 34, 962–971
>8 Punkte: definitive FH; 3-5 Punkte: mögliche FH;
6-8 Punkte: wahrscheinliche FH < 3 Punkte: keine FHPrevalence of clinical familial hypercholesterolaemia
among Swiss patients with acute coronary syndrome
David Nanchen et al. Eur Heart J 2015;36:2438-2445Impact of Familial Hypercholesterolemia mutation status on CHD risk according to levels of LDL cholesterol Khera, A.V. et al. J Am Coll Cardiol. 2016;67(22):2578–89
ESC/EAS 2019 Recommendations on
the management of familial hypercholesterolemia
Mach, Baigent, Catapano et al. European Heart Journal (2019)PCSK9-Inhibitoren bei Familiärer Hypercholesterinämie:
Wichtigste Diskrepanzen zwischen ESC/EAS2019
Empfehlungen und BAG-Limitatio in CH
ESC/EAS* BAG Limitatio für CH**
Indikationen FH mit ASCVD oder FH, bei der trotz Statine
weiterem schweren definierte Behandlungsziele
Risikofaktor, bei der trotz nicht erreicht werden
Statine + Ezitimibe
definierte
Behandlungsziele nicht
erreicht werden
Indikationsschwellen > 1.4 mmol/L FH mit ASCVD: > 2.6 mmol/L
LDL-Cholesterin (> 1.0 mmol/L) FH mit RF: > 4.5 mmol/L
FH sonst: > 5.0 mmol/L
Testung von Ezitimibe empfohlen fakultativ
*: Mach, Baigent, Catapano et al.
**: Spezialitätenliste des
European Heart Journal (2019) or Atherosclerosis (2019)
Bundesamt für Gesundheit,
www.escardio.org/guidelines or
http://www.spezilitätenliste.ch
https://www.eas-society.org/page/dyslipidemia_guide_2019ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention Familiäre Hypercholesterinämie Risikoschätzung
Joint European Guidelines on CVD prevention: 10-Jahres-Risiken für ein tödliches kardiovaskuläres Ereignis bei Frauen und Männern in der Schweiz (sehr) hohes Risiko, wenn - Arteriosklerose vorhanden - oder Diab. Mell. mit Endorganschaden oder >3 Risikofaktoren - Oder Diab. mell. Typ 1 nach langer Dauer - Oder CKD mit eGFR < 30 ml/min - Oder multiple Risikofaktoren (RF), die ein fatales CVD Risiko > 10% in 10 Jahren ergeben - oder Cholesterin > 8 mmol/L - oder LDL-C > 6 mmol/L - oder Blutdruck > 180/110 mm Hg - Oder Diabetes > 10 Jahre Dauer ohne Endorganschaden oder zusätzliche RF - Oder familiäre Hypercholesterinämie - Oder CLD mit eGFR 30 – 60 ml/min - oder multiple Risikofaktoren, die ein fatales www.heartscore.org CVD Risiko 5 - 10% in 10 Jahren ergeben
Risk function with high-density lipoprotein cholesterol for women
in populations at high cardiovascular disease risk
www.heartscore.orgRisk modifiers
Mach, Baigent, Catapano et al. European Heart Journal (2019)Recommendations for cardiovascular imaging
for risk assessment of
atherosclerotic cardiovascular disease
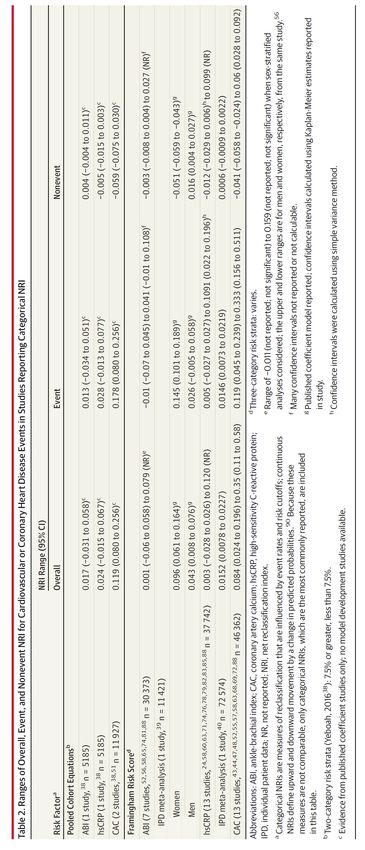
Mach, Baigent, Catapano et al. European Heart Journal (2019)Nontraditional Risk Factors in CVD Risk Assessment:
Systematic Review for the US Preventive Services Task Force
43 studies with N = 267’244 participants.
Lin et al. JAMA. 2018;320(3):281-297.ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention Familiäre Hypercholesterinämie Risikoschätzung ältere Menschen
SCORE chart for European populations at low
cardiovascular disease risk (aged 65-70 years)
Mach, Baigent, Catapano et al. European Heart Journal (2019)SCORE chart for European populations at low
cardiovascular disease risk (aged 70-75 years)
Mach, Baigent, Catapano et al. European Heart Journal (2019)Short-Term Global Cardiovascular Disease Risk Prediction in Older Adults: Comparisons of Biomarkers With the Pooled Cohort Equation (PCE) and Other Models ARIC study participants without CVD including HF (n = 4,760; age 75.4 +/- 5.1 years). median follow-up of 4 years, incident HF: n = 193; CHD: N = 118; Stroke: N = 81 Saeed, A. et al. J Am Coll Cardiol. 2018;71(22):2527–36.
Age Considerations for
Global Cardiovascular Disease Risk Assessment
Saeed, A. et al. J Am Coll Cardiol. 2018;71(22):2527–36.ESC/EAS 2019 Recommendations for the treatment
of dyslipidaemias in older people (aged >65 years)
Mach, Baigent, Catapano et al. European Heart Journal (2019)Never too old for Statins? Effects on major vascular events per mmol/L reduction in LDL cholesterol by age at randomisation Cholesterol Treatment Trialists’ Collaboration: Lancet 2019; 393: 407–15
Never too old for Statins? Effects on major vascular events per mmol/L reduction in LDL-Cholesterol, subdivided by age at randomisation and by previous vascular disease Cholesterol Treatment Trialists’ Collaboration: Lancet 2019; 393: 407–15
Never too old for Statins? Effects on vascular death per mmol/L reduction in LDL cholesterol in all studies, by age at randomisation Cholesterol Treatment Trialists’ Collaboration: Lancet 2019; 393: 407–15
Statins for primary prevention of cardiovascular events and mortality
in old and very old adults with and without type 2 diabetes:
retrospective
cohort study:
46’864 participants
(mean age 77 yrs;
63% women;
median follow-up
5.6 years).
Ramos et al. BMJ 2018;362:k3359ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention Familiäre Hypercholesterinämie Risikoschätzung ältere Menschen junge Menschen
SCORE chart for European populations at low
cardiovascular disease risk (aged 40-49 years)
Mach, Baigent, Catapano et al. European Heart Journal (2019)Guideline-Based Statin Eligibility of Young Adults Prior to a
Myocardial Infarction
Singh, A. et al. J Am Coll Cardiol. 2018;71(3):292–302.Proportion of patients with high lifetime cardiovascular risk (> 40%)
among young adults with myocardial infarction.
Singh, A. et al. J Am Coll Cardiol. 2018;71(3):292–302.Chart for estimating the relative risk for 10-year
cardiovascular mortality in young people
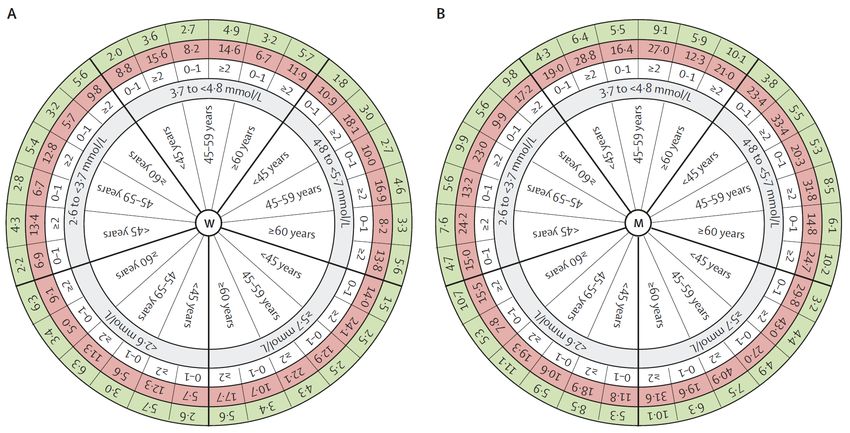
Mach, Baigent, Catapano et al. European Heart Journal (2019)Model of long-term cardiovascular disease risk
prediction and the benefit of lipid reduction
women men
White Circle: number of additional cardiovascular risk factors (daily smoking, arterial hypertension, diabetes, and obesity)
The red circle: probability (%) of cardiovascular disease by the age of 75 years.
Green circle: The hypothetical probability (%) for cardiovascular disease by the age of 75 years after 50% reduction of non-HDL cholesterol.
Brunner et al. on behalf of the Multinational Cardiovascular Risk Consortium. Lancet 2019; 394: 2173–83NNT and RRR by age group and number of comorbid risk factors for non-HDL cholesterol categories Brunner et al. on behalf of the Multinational Cardiovascular Risk Consortium. Lancet 2019; 394: 2173–83
ESC/EAS-Leitlinien zur Dyslipidämie Hintergründe und Prinzipien LDL-Cholesterin in der Sekundärprävention LDL-Cholesterin in der Primärprävention andere Lipid-Risikofaktoren
Primary and secondary treatment targets and goals for
prevention of cardiovascular disease
Primary Secondary
CVD risk LDL-cholesterol nonHDL-cholesterol Apolipoprotein B
mmol/L mg/dL mmol/L mg/dL g/L mg/dL
Very highESC/EAS 2019 Recommendations for drug
treatments of patients with hypertriglyceridaemia
Mach, Baigent, Catapano et al. European Heart Journal (2019)Cardiovascular risk reduction by fibrates
in randomized clinical endpoint trials
Trial fibrate patients ∆ % events ∆ % events in
entire cohort Low HDL/HTG
(P) (P)
HHS1,2 gemfibrozil Primary -34 -65
prevention (Should we use omega -3 fatty acids?
ASCEND: REDUCE-IT:
• 8179 patients on statin with CV event or
• Diabetics age over 40y, no CVD
DM+ one risk factor and high TG
• N=15480 FU 7.4 y • Randomised to 4 gr pure EPA or placebo
• 1 gr omega 3/day • 4.9 year follow up
• Primary end point: CV death,MI,stroke,
revascularization, UA
• TGs reduced 20%, CRP reduced by 40 %
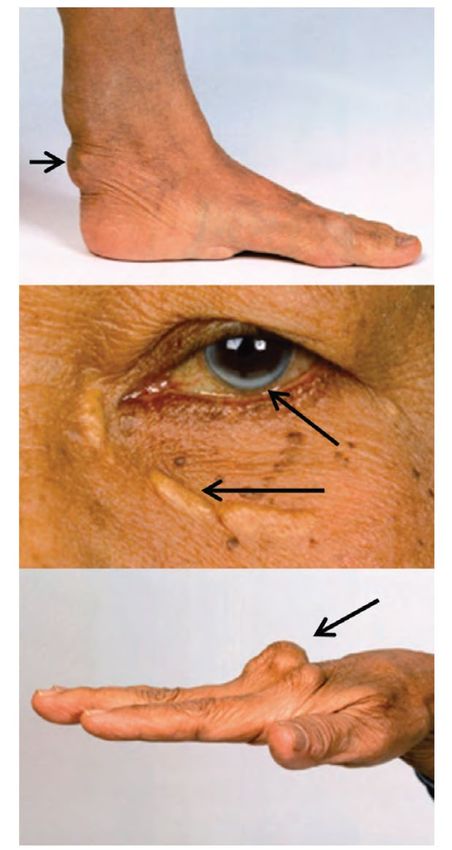
N Engl J Med 2018; 379:1529 N Engl J Med 2019; 380:11Lipoprotein(a) is important in risk determination
Recommendations Class Level
Lp(a) measurement should be considered at least once in each adult
person’s lifetime to identify those with very high inherited Lp(a) levels
>180 mg/dL (>430 nmol/L) who may have a lifetime risk of ASCVD
equivalent to the risk associated with heterozygous familial IIa C
hypercholesterolaemia.
Lp(a) should be considered in selected patients with a family history of
premature CVD, and for reclassification in people who are borderline
©ESC
between moderate and high-risk. IIa CSie können auch lesen