Einsatzmöglichkeiten von Cannabispräparaten in der Medizin im Alter
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Einsatzmöglichkeiten von
Cannabispräparaten in der Medizin im Alter
Univ. Prof. Dr. Rudolf Likar, MSc
Vorstand der Abteilung für Anästhesiologie,
allgemeine Intensivmedizin, Notfallmedizin,
interdisziplinäre Schmerztherapie und Palliativmedizin
Klinikum Klagenfurt am Wörthersee
LKH Wolfsberg
Lehrabteilung der Medizinischen Universität
Graz, Innsbruck, Wien
Lehrstuhl für Palliativmedizin SFU
Update: Cannabinoide in der Schmerzmedizin
Aktuelle Diskussion und Begriffsklärung
Wirkmechanismen
Cannabinoide in der Schmerztherapie
Wichtige Nebenwirkungen
Cannabinoide im Alter
Hanf (Cannabis sativa)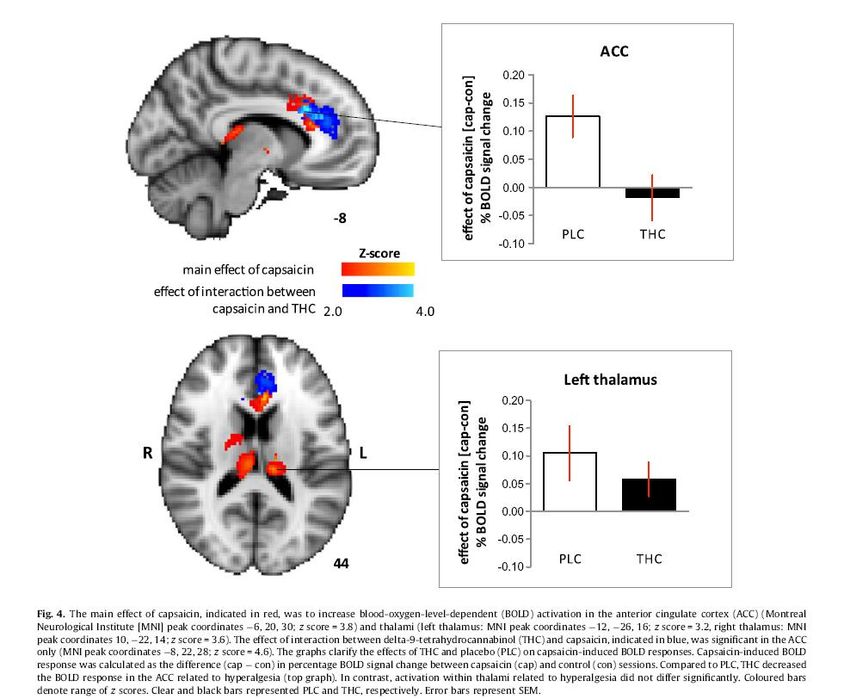
Cannabinoids in the management of chronic pain: a
front line clinical perspective.
Lynch ME.:Basic Clin Physiol Pharmacol. 2015 Nov 18.
Cannabinoide zeigen einen analgetischen Effekt und sind sicher
in der Anwendung bei chronischem Schmerz
25 von 30 randomisiert-kontrollierten Studien zeigten einen
signifikanten analgetischen Effekt
Unserer Patienten verdienen zusätzliche Mittel zur
Schmerzkontrolle mit einem neuen Wirkmechanismus
Cannabinoide sind neue Vorreiter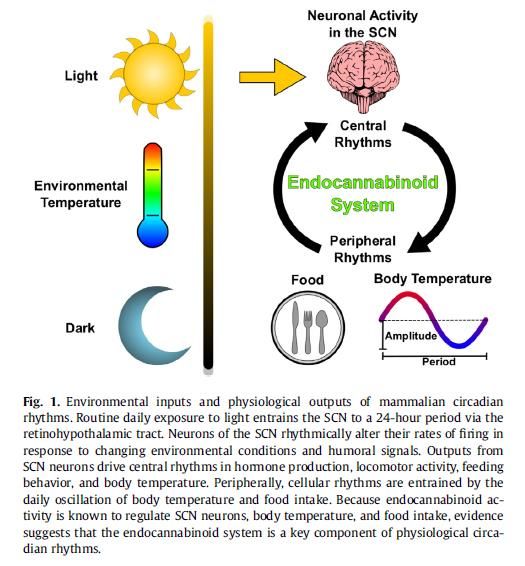
Cannabinoid- Rezeptoren1
CB1: ZNS, peripheres Nervensystem
Auch in Leber, Dünndarm, Hoden, Fettzellen
CB2: Immunsystem, Mikroglia, Hirnstamm, Milz
G-protein-gekoppelter
Rezeptor
CB1 Rezeptoren haben Einfluss auf:
Koordination
Schmerzverarbeitung
Wahrnehmung, Gedächtnis
Emotionen
Appetit
1Woods, 2005, Mackie 2008,
Karst M.; Cannabinoide in der Schmerzmedizin; Schmerz 2018; 32:381-396.
13MaejimaT, Ohno-shosakuT, KanoM (2001)Endogenous cannabinoidas
a retrogrademessenger frompostsynaptic neurons to presynaptic
terminals. NeurosciRes 40:205–210;.
Karst M.; Cannabinoide in der Schmerzmedizin; Schmerz 2018; 32:381-396.
Endocannabinoide: Regulierender
Rückkopplungseffekt
Intensive Erregung durch Glutamat aus dem präsynaptischen
Neuron führt zu Synthese von postsynaptischen Endocannabinoiden
Retrograde Freisetzung in den synaptischen Spalt
Aktivierung präsynaptischer CB Rezeptoren
Freisetzung von Glutamat unterdrückt
Aber: Retrograde Hemmung kann auch gegen Freisetzung
inhibitorische Transmitter (z.B. GABA) gerichtet sein1
EC-CB System moduliert die neuronale Erregung im Sinne
einer Filterfunktion gegen zu starke synaptische Prozesse
(Exzitation wie Inhibition)
Science 7 August 20091 Spinal Endocannabinoids and CB1 Receptors Mediate C-Fiber–Induced Heterosynaptic Pain
Sensitization; Alejandro J…. Hans Ulrich Zeilhofer 1,9
Cannabis Cannabinoids Cannabis Cannabinoide Pflanzliches Material oder (Semi-)synthetisch oder Extrakte, die ca. 63 aus der Pflanze verschiedene Cannabinoide, gewonnene einzelne Terpene oder Flavonoide chemisch definierte etc. enthalten. Verbindungen

„Medizinische“ Cannabinoide
Definitionen und Medikamente I
THC (Delta-9-Tetrahydrocannabinol)– ist wenn nicht anders kenntlich
gemacht – das in der Hanfpflanze (Cannabis sativa) vorkommende natürliche
(-)-trans-Isomer des Delta-9-Tetrahydrocannabinol gemeint
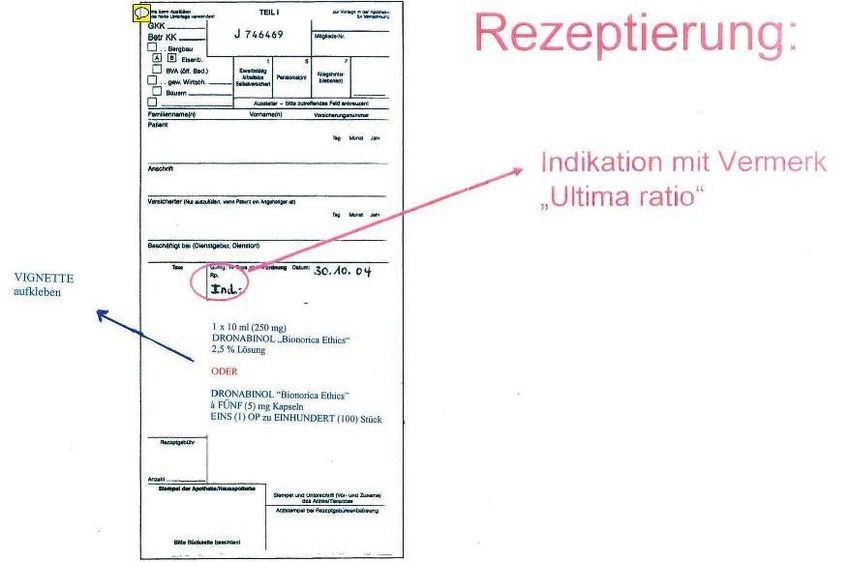
Dronabinol = Delta-9-tetrahydrocannabinol (THC): Internationaler
Freiname (INN) für THC. Wirkstoff hergestellt aus Nutzhanf von Binorica
Ethics und THC-Pharm. In Apotheken in Form von Kapseln oder Lösung
zubereitet (kein Fertigarzneimittel)
Marinol® ist Dronabinol als Kapsel (Fertigarznei) in USA im Handel
(importierbar) (2.5mg)
*Insgesamt in Cannabis sativa über 60 CannabinoideMedizinische Cannabinoide
Definitionen und Medikamente
Nabilone® (UK and Europe): Synthetisches Derivat von Dronabinol
= Als Cesamet® von der FDA zur chemotherapie-induzierten Übelkeit
zugelassen,Canemes ®
CBD oder Cannabidiol ist das wichtigste nicht psychotrope
Cannabinoid der Hanfpflanze – kein Arzneimittel
Sativex®, Nabiximols® (Dronabinol (THC)+ Cannabidiol (CBD):
Sublingual - Spray (zugelassen in Kanada 2005, UK, Spanien 2010;
Deutschland, Dänemark usw. 2011) Indikation: MS, Spastizität
Epidiolex Cannabidiol zugelassen spez. Formen Epilepsie
1Die Rolle des nicht psychoaktiven Cannabidiol im Bereich
der Schmerztherapie ist nicht ausreichend untersuchtExogene Cannabinioide
9 Tetrahydrocannabinol (THC)
Partialagonist CB1/2
analgetisch
antispastisch
antiemetisch
appetitsteigernd
sedierend
Cannabidiol
Agonist/Antagonist CB 1 / 2,
Hemmung FAAH-System
entzündungshemmend
antipsychotisch
anxiolytisch
antikonvulsivDronabinol = Delta-9-tetrahydrocannabinol
(THC): Pharmakokinetik
65%
Oral: 20%
Bioverfügbarkeit: 6-20%,
Wegen Lipophilie Resorption schwierig zu steuern,
Fetthaltige Nahrung verbessert Resorption, 15%
Spitzenkonzentration: 2-5 Stunden, Wirkungseintritt 1/2-2h;
Wirkdauer bis 6-8 h, Effekt auf Appetitsteigerung bis 24h
Inhalativ:
Wirkeintritt in Sekunden
Spitzenkonzentration in 15 Minuten
Wirkdauer kürzer (2-4h)
Vollständige Elimination des Metaboliten 11-OH-THC und THC-
COOH: bis zu Wochen
Huestis MA. Human cannabinoid pharmacokinetics. Chem Biodivers 2007; 4: 1770-804.In clinical trials and research studies, CBD is generally administered orally as either a capsule, or dissolved in an oil solution (e.g. olive or sesame oil). It can also be administered through sublingual or intranasal routes. A wide range of oral doses have been reported in the literature, with most from 100-800mg/day. B. Pharmacokinetics Oral delivery of an oil-based capsule formulation of CBD has been assessed in humans. Probably due to its poor aqueous solubility, the absorption of CBD from the gastrointestinal tract is erratic, and the resulting pharmacokinetic profile is variable. Bioavailability from oral delivery was estimated to be 6% due to significant first-pass metabolism. In healthy male volunteers, the mean±SD whole blood levels of CBD at 1, 2 and 3 hours after administration of 600mg oral CBD were reported to be 0.36 (0.64) ng/mL, 1.62 (2.98) ng/mL and 3.4 (6.42) ng/mL, respectively. Aerosolized CBD has been reported to yield rapid peak plasma concentrations in 5–10 minutes and higher bioavailability than oral administration. Fasinu, P.S., et al., Current Status and Prospects for Cannabidiol Preparations as New Therapeutic Agents. Pharmacotherapy, 2016. 36(7): p. 781-96. Martin-Santos, R., et al., Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Curr Pharm Des, 2012. 18(32): p. 4966-79.
Prescription (Dronabinol – narcotic)
Cannabis:
Zusammenfassung Teil I
Cannabis hat einen festen Platz in der Medizingeschichte
Delta-9-Tetrahydrocannabinol (THC) ist das wichtigste Cannabinoid
THC wirkt an zentralen und peripheren CB-Rezeptoren
Cannabidiol wirkt hat wenig psychotrope Wirkungen und kann
unerwünschte psychologische Effekte von THC vermindern
Endocannabinoide und Cannabinoide haben eine Filterfunktion an
nozizeptiven und inhibitorischen Neuronen und können
Akutschmerzen verstärken
Die Pharmakokinetik von oralen, sublingualen und inhalatativen
Formulierungen ist unterschiedlich und muss berücksichtigt werdenTherapeutische Optionen
Schmerz z.B. Fibromyalgie,
Phantomschmerzen, Neurodegenerative Erkrankungen z.B.
schmerzhafte Muskel-Skelett- Alzheimer-Krankheit, Multiple
Erkrankungen, diabetische und Sklerose, Amyotrophe Lateralsklerose,
andere Neuropathien Schlaganfall (ischämisch),
Zusatzmedikation für Opioide Rückenmarksverletzung
Psychiatrische Erkrankungen, Angstzustände z.B. Alpträume,
Depressionen, posttraumatische Belastungsstörungen, Burn-Out-
Syndrom, ADHS, Tourette-Syndrom, TICS
Palliativ: Appetitkontrolle - Übelkeit, Erbrechen
Cannabinoids in AustriaCannabinoide bei chronischen
neuropathischen Schmerzen –
Systematischer Review
J Oral Facial Pain Headache. 2015;29(1):7-14.The effectiveness of cannabinoids in the management of
chronic nonmalignant neuropathic pain: a systematic review. Boychuk DG, Goddard G, Mauro G, Orellana MF.
13 RCT-Studien erfüllten die strengen Qualitätskriterien
Cannabinoide können bei sonst therapieresisten Schmerzen effektive
Schmerzlinderung bringen
Weitere hochqualitative Studien sind notwendig um Informationen zur
Therapiedauer und zur besten Form der Applikation zu bekommen
Br J Clin Pharmacol. 2011 Nov; 72(5): 735–744. Cannabinoids for treatment of chronic non-
cancer pain; a systematic review of randomized trials
Mary E Lynch and Fiona Campbell
18 RCT-Studien erfüllten die Qualitätskriterien
Dieser systematische Review zeigte dass Cannabinoide bescheiden wirksam sind aber
eine sichere Behandlung bei vor allem neuropahischen Schmerzen darstellenJuly 2015 JAMA Mehrere der 18 randomisierten klinischen Studien zum Schmerz (6 bei neuropathischen Schmerzen, 12 bei Muskelschmerzen bei MS) zeigten zum Teil positive Ergebnisse, was “andeutete “ dass Cannabis wirksam sein könnte!
THC/CBD Spray bei peripheren schmerzhaften
Neuropathien
Eur J Pain. 2014 Aug;18(7): A double-blind, randomized, placebo-controlled, parallel group study of THC/CBD
spray in peripheral neuropathic pain treatment.
Serpell M1, Ratcliffe S, Hovorka J, Schofield M, Taylor L, Lauder H, Ehler E.
N= 128 (Verum), 118 (Placebo), Krankheit: PNP mit Allodynie
THC/CBD Spray zusätzlich zur bisherigen Therapie,
Reduktion des Schmerzwertes
(aber statistische Signifikanz knapp verfehlt)
THC/CBD Spray wurde gut toleriertLangzeitdaten von THC/Cannabidiol
bei Spastik
Paolicelli D.: Long-Term Data of Efficacy, Safety and
Tolerability in a Real Life Setting of THC/CBD Oromucosal
Spray-Treated Multiple Sclerosis Patients. J Clin Pharmacol.
2015 Nov 26.
N=102 MS Patienten ; Verbrauch : 6.5±1.6 Sprühstöße/d.
Der Spastizitätsscore reduzierte sich im Mittel um 2.5±1.2
(pCannabis bei Multipler Sklerose
There is evidence for the use of cannabinoids for symptomatic
treatment of multiple sclerosis.
Bazinski H, Jensen HB, Stenager E. Ugeskr Laeger. 2015 May 11;177(20):956-60.Meta-analysis of efficacy: intensity of pain by visual analog scale (VAS). * Parallel design. SD = standard deviation; r = within-patients coefficient; SMD = standardized mean differences; CI = confidence interval. Martín-Sánchez E, Furukawa TA, Taylor J, Martin JLR. Systematic Review and Meta-analysis of Cannabis Treatment for Chronic Pain. Pain Medicine 2009; 10(8):1353-1368
Meta-analysis of events related to mood disturbances. * Parallel design. OR = odds ratio; SE = standard error; CI = confidence interval; r = within-patients coefficient; BB = Becker Balagtas method. Martín-Sánchez E, Furukawa TA, Taylor J, Martin JLR. Systematic Review and Meta- analysis of Cannabis Treatment for Chronic Pain. Pain Medicine 2009; 10(8):1353-1368
Meta-analysis of events affecting motor function. * Parallel design. OR = odds ratio; SE = standard error; CI = confidence interval; r = within-patients coefficient; BB = Becker Balagtas method. Martín-Sánchez E, Furukawa TA, Taylor J, Martin JLR. Systematic Review and Meta- analysis of Cannabis Treatment for Chronic Pain. Pain Medicine 2009; 10(8):1353-1368
Meta-analysis of events that altered cognitive function. * Parallel design. OR = odds ratio; SE = standard error; CI = confidence interval; r = within-patients coefficient; BB = Becker Balagtas method. Martín-Sánchez E, Furukawa TA, Taylor J, Martin JLR. Systematic Review and Meta- analysis of Cannabis Treatment for Chronic Pain. Pain Medicine 2009; 10(8):1353-1368
Fazit für die Praxis
• Die aktuelle Datenlage kann einen Einsatz von Cannabisprodukten bei
sorgfaltig ausgewählten Patienten mit therapierefraktären chronischen
neuropathischen Schmerzen als Drittlinientherapie begründen, sofern
relevante psychiatrische Vorerkrankungen, die insbesondere mit der Gefahr
von Substanzmissbrauch einhergehen, ausgeschlossen bzw. behandelt
wurden und alternative Therapieoptionen ausgeschöpft worden sind.
• Idealerweise sollte eine mögliche Anwendung aufgrund der eingeschränkten
Datenlage zur Sicherheit und Effektivitat der Langzeittherapie von einer Art Register zur
Gewinnung standardisierter Versorgungsdaten begleitet werden. Eine Betreuung durch
schmerzmedizinisch erfahrene Behandler ist zu empfehlen.
Petzke F, Enax-Krumova EK, Häuser W. Wirksamkeit, Vertraglichkeit und Sicherheit von Cannabinoiden bei neuropathischen
Schmerzsyndromen Eine systematische Ubersichtsarbeit von randomisierten, kontrollierten Studien. Schmerz 2016 ・ 30:62–88• Es sind keine Daten für den Einsatz von Cannabisprodukten bei Kindern und Jugendlichen oder Patienten mit relevanten körperlichen Begleiterkrankungen, Epilepsie und seelischen Storungen inklusive früherer und aktueller Substanzabhängigkeit verfügbar. • Im Falle des Einsatzes von Cannabisprodukten könnten die aktualisierten Empfehlungen zur Langzeitanwendung von Opioiden bei nicht tumorbedingten Schmerzen (LONTS;) analog verwendet werden (vor Therapiebeginn festgelegte Ziele der Schmerzreduktion und/ oder Verbesserung der körperlichen Funktionsfahigkeit; sorgfaltige Uberwachung der Wirkung und möglicher Komplikationen;) Petzke F, Enax-Krumova EK, Häuser W. Wirksamkeit, Vertraglichkeit und Sicherheit von Cannabinoiden bei neuropathischen Schmerzsyndromen Eine systematische Ubersichtsarbeit von randomisierten, kontrollierten Studien. Schmerz 2016 ・ 30:62–88 Hauser W, Bock F, Engeser P et al (2015) Empfehlungen der aktualisierten Leitlinie LONTS. Schmerz 29:109–130
Volz MS, Siegmund B, Häuser W. Wirksamkeit, Vertraglichkeit und Sicherheit von Cannabinoiden in der Gastroenterologie Eine systematische Ubersichtsarbeit. Schmerz 2016 30:37–46
FAZIT für die Praxis • Insgesamt müssen für eine valide Empfehlung von Cannabinoiden für bestimmte gastroenterologische Erkrankungen mehr RCT mit einer ausreichenden Patientenzahl angestrebt werden. • Auf der Basis der aktuellen Datenlage kann ein individueller Heilversuch mit synthetischen Cannabinoiden bei gastroenterologischen Erkrankungen bislang nur beim Morbus Crohn zur krankheitsspezifischen Symptommilderung und nur nach Versagen aller etablierten medikamentösen Therapien erwogen werden. • Da die neuropsychiatrischen Nebenwirkungen und Langzeitfolgen eines regelmäßigen Cannabiskonsums bei medizinischen Indikationen nicht abgeschätzt werden konnen (da keine validen Daten hierzu vorliegen), ist die Indikationsstellung eines individuellen Heilversuchs in jedem Falle kritisch und unter einer individuellen Nutzen-Risiko-Abwägung zu diskutieren. Volz MS, Siegmund B, Häuser W. Wirksamkeit, Vertraglichkeit und Sicherheit von Cannabinoiden in der Gastroenterologie Eine systematische Ubersichtsarbeit. Schmerz 2016 30:37–46
• In Israel ist die Verordnung von Medizinalhanf für Patienten mit CED (chronisch entzündliche Darmerkrankungen) möglich, die auf eine immunsuppressive Therapie inklusive TNF- α-Antikörper nicht angesprochen haben und bei denen chirurgisch behebbare Ursachen der Beschwerden ausgeschlossen wurden. Kontraindikationen sind Herzinsuffizienz, frühere oder aktuelle Psychosen,Angststörungen, erstgradige Verwandte mit psychischen Störungen und eine Vorgeschichte von Drogenabhängigkeit. • Ob diese Indikationen und Kontraindikationen auch auf Deutschland anwendbar sind, bedarf weiterer Diskussionen und der Konsensbildung der medizinischen Fachgesellschaften. Volz MS, Siegmund B, Häuser W. Wirksamkeit, Vertraglichkeit und Sicherheit von Cannabinoiden in der Gastroenterologie Eine systematische Ubersichtsarbeit. Schmerz 2016 30:37–46 Ablin J, St.-Marie PA et al (2015) Medical cannabis – lessons to be learned from Israel and Canada. Schmerz.
Schlussfolgerung
Nabilone verbessert effektiv den Schlaf von Patienten
mit Fibromyalgie und wird gut toleriert.
Eine niedrige Dosis von Nabilone (0,5 – 1 mg) 1 x tgl.
vor dem Schlafengehen verabreicht kommt als
Alternative zu Amitryptilin in Betracht (10 – 20 mg).
Weitere Studien sind notwendig, um den Effekt in der
Langzeitanwendung und in der Langzeit-Sicherheit zu
beurteilen.
Ware MA, Fitzcharles MA, Joseph L, Shir Y. The Effects of Nabilone on Sleep in Fibromyalgia: Results of a Randomized Controlled Trial.
Pain Medicine 2010; 110(2):604-610Fitzcharles MS, Baerwald C, Ablin J et al. Efficacy, tolerability and safety of cannabinoids in chronic pain associated with rheumatic diseases (fibromyalgia syndrome, back pain, osteoarthritis, rheumatoid arthritis) A systematic review of randomized controlled trials. Schmerz DOI 10.1007/s00482-015-0084-3
Fitzcharles MS, Baerwald C, Ablin J et al. Efficacy, tolerability and safety of cannabinoids in chronic pain associated with rheumatic diseases (fibromyalgia syndrome, back pain, osteoarthritis, rheumatoid arthritis) A systematic review of randomized controlled trials. Schmerz DOI 10.1007/s00482-015-0084-3
Schlussfolgerungen. Aktuell besteht keine ausreichende Evidenz, eine symptomatische Behandlung von Patienten mit chronischen Schmerzen bei rheumatischen Erkrankungen mit Cannabispräparaten zu empfehlen. Fitzcharles MS, Baerwald C, Ablin J et al. Efficacy, tolerability and safety of cannabinoids in chronic pain associated with rheumatic diseases (fibromyalgia syndrome, back pain, osteoarthritis, rheumatoid arthritis) A systematic review of randomized controlled trials. Schmerz DOI 10.1007/s00482-015-0084-3
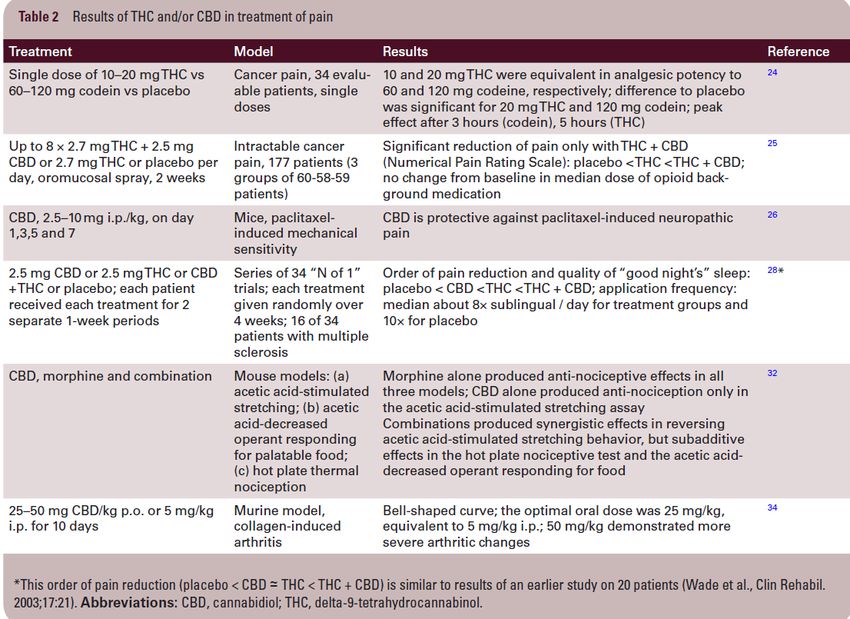
24. Noyes R Jr, Brunk SF, Avery DA, et al. The analgesic properties of delta-9-tetrahydrocannabinol and codeine. Clin Pharmacol Ther. 1975;18(1):84–89. 25. Johnson JR, Burnell-Nugent M, Lossignol D et al. Multicenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety, and tolerability of THC:CBD extract and THC extract in patients with intractable cancer-related pain. J Pain Symptom Manage. 2010;39(2):167–179. 26. Ward SJ, McAllister SD, Kawamura R, et al. Cannabidiol inhibits paclitaxel-induced neuropathic pain through 5-HT(1A) receptors without diminishing nervous system function or chemotherapy efficacy. Br J Pharmacol. 2014;171(3):636–645. 28. Notcutt W, Price M, Miller R, et al. Initial experiences with medicinal extracts of cannabis for chronic pain: results from 34 ‘N of 1’ studies. Anaesthesia. 2004;59(5):440–452. 32. Neelakantan H, Tallarida RJ, Reichenbach ZW, et al. Distinct interactions of cannabidiol and morphine in three nociceptive behavioral models in mice. Behav Pharmacol. 2015;26(3):304–314. 34. Malfait AM, Gallily R, Sumariwalla PF, et al. The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen- induced arthritis. Proc Natl Acad Sci U S A. 2000;97(17):9561–9566. Likar R, Nahler G, The use of cannabis in supportive care and treatment of brain tumor. Neuro-Oncology Practice. 2017.
59. Guzmán M, Duarte MJ, Blázquez C, et al. A pilot clinical study of Delta9-tetrahydrocannabinol in patients with recurrent
glioblastoma multiforme. Br J Cancer. 2006;95(2):197–203.
61. Solinas M, Massi P, Cinquina V, et al. Cannabidiol, a non-psychoactive cannabinoid compound, inhibits proliferation and
invasion in U87-MG and T98G glioma cells through a multitarget effect. PLoS ONE. 2013;8(10):e76918.
66. Fisher Z, Golan H, Schiby G, et al. In vitro and in vivo efficacy of nonpsychoactive cannabidiol in neuroblastoma. Curr Oncol.
2016;23(suppl 2):15–22.
67. Carracedo A, Lorente M, Egia A, et al. The stress-regulated protein p8 mediates cannabinoid-induced apoptosis of tumor cells.
Cancer Cell. 2006;9(4):301–312.
68. Salazar M, Carracedo A, Salanueva IJ, et al. Cannabinoid action induces autophagy-mediated cell death through stimulation of
ER stress in human glioma cells. J Clin Invest. 2009;119(5):1359–1372.
70. Torres S, Lorente M, Rodríguez-Fornés F, et al. A combined preclinical therapy of cannabinoids and temozolomide against
glioma. Mol Cancer Ther. 2011;10(1):90–103.
71. Galve-Roperh I, Sánchez C, Cortés ML, et al. Anti-tumoral action of cannabinoids: involvement of sustained ceramide
accumulation and extracellular signal-regulated kinase activation. Nat Med. 2000;6(3):313–319.
72. Scott KA, Dalgleish AG, Liu WM. The combination of cannabidiol and Δ9-tetrahydrocannabinol enhances the anticancer effects
of radiation in an orthotopic murine glioma model. Mol Cancer Ther. 2014;13(12):2955–2967.
Likar R, Nahler G, The use of cannabis in supportive care and treatment of brain tumor.
Neuro-Oncology Practice. 2017.59. Guzmán M, Duarte MJ, Blázquez C, et al. A pilot clinical study of Delta9-tetrahydrocannabinol in patients with recurrent
glioblastoma multiforme. Br J Cancer. 2006;95(2):197–203.
61. Solinas M, Massi P, Cinquina V, et al. Cannabidiol, a non-psychoactive cannabinoid compound, inhibits proliferation and
invasion in U87-MG and T98G glioma cells through a multitarget effect. PLoS ONE. 2013;8(10):e76918.
66. Fisher Z, Golan H, Schiby G, et al. In vitro and in vivo efficacy of nonpsychoactive cannabidiol in neuroblastoma. Curr Oncol.
2016;23(suppl 2):15–22.
67. Carracedo A, Lorente M, Egia A, et al. The stress-regulated protein p8 mediates cannabinoid-induced apoptosis of tumor cells.
Cancer Cell. 2006;9(4):301–312.
68. Salazar M, Carracedo A, Salanueva IJ, et al. Cannabinoid action induces autophagy-mediated cell death through stimulation of
ER stress in human glioma cells. J Clin Invest. 2009;119(5):1359–1372.
70. Torres S, Lorente M, Rodríguez-Fornés F, et al. A combined preclinical therapy of cannabinoids and temozolomide against
glioma. Mol Cancer Ther. 2011;10(1):90–103.
71. Galve-Roperh I, Sánchez C, Cortés ML, et al. Anti-tumoral action of cannabinoids: involvement of sustained ceramide
accumulation and extracellular signal-regulated kinase activation. Nat Med. 2000;6(3):313–319.
72. Scott KA, Dalgleish AG, Liu WM. The combination of cannabidiol and Δ9-tetrahydrocannabinol enhances the anticancer effects
of radiation in an orthotopic murine glioma model. Mol Cancer Ther. 2014;13(12):2955–2967.
Likar R, Nahler G, The use of cannabis in supportive care and treatment of brain tumor.
Neuro-Oncology Practice. 2017.Abstract Cannabinoids are multitarget substances. Currently available are dronabinol (synthetic delta-9-tetrahydrocannabinol, THC), synthetic cannabidiol (CBD) the respective substances isolated and purified from cannabis, a refined extract, nabiximols (THC:CBD = 1.08:1.00); and nabilone, which is also synthetic and has properties that are very similar to those of THC. Cannabinoids have a role in the treatment of cancer as palliative interventions against nausea, vomiting, pain, anxiety, and sleep disturbances. THC and nabilone are also used for anorexia and weight loss, whereas CBD has no orexigenic effect. The psychotropic effects of THC and nabilone, although often undesirable, can improve mood when administered in low doses. CBD has no psychotropic effects; it is anxiolytic and antidepressive. Of particular interest are glioma studies in animals where relatively high doses of CBD and THC demonstrated significant regression of tumor volumes (approximately 50% to 95% and even complete eradication in rare cases). Concomitant treatment with X-rays or temozolomide enhanced activity further. Similarly, a combination of THC with CBD showed synergistic effects. Although many questions, such as on optimized treatment schedules, are still unresolved, today’s scientific results suggest that cannabinoids could play an important role in palliative care of brain tumor patients. Likar R, Nahler G, The use of cannabis in supportive care and treatment of brain tumor. Neuro-Oncology Practice. 2017.
Es gab spezifische Veränderungen, die bei keiner Verbindung einzeln beobachtet wurden, was darauf hinweist, dass die Signaltransduktionswege, die durch die Kombinationsbehandlung beeinflusst wurden, einzigartig waren. Die Forscher kamen zu dem Schluss, dass diese "Ergebnisse darauf hindeuten, dass die Zugabe von Cannabidiol zu Delta-9-THC die Gesamtwirksamkeit von Delta-9-THC bei der Behandlung von Glioblastomen verbessern kann Marcu JP, Christian RT, Lau D, et al; Cannabidiol enhances the inhibitory effects of Delta9-tetrahydrocannabinol on human glioblastoma cell proliferation and survival. Mol Canser Ther 2010.
Frühe Schmerzstudien mit CBD
zeigten limitierten Benefit
CBD unterdosiert:
2.5mg/d - 2w (Oraler Spray, Notcutt et al., 2004);
2.5-120mg/d – 2w (oraler Spray, Wade et al., 2003)
Zu kurz (Schmerzreduktion verdoppelt sich nach 6-
8w)
Confounders in den Studien
Z.B.: Positive Auswahl der Responder nach
Einlaufzeit, Verschleppungseffekte nach Wechsel zu
anderen Behandlungen, Rescue-Medikation,
Verblindung, etc.
Verwendung von CBD-reichen Extrakten (~95%)
Es scheint "CBD-Responder" als Untergruppe zu geben
Das niedrigste beobachtete Effektniveau (LOEL) von
CBD wie es aus klinischen Studien geschätzt wird,
beträgt ungefähr 200 mg p.o./d
Notcutt W, et al: Initial experiences with medicinal extracts of cannabis for chronic pain: results from 34 ‘N of 1’ studies.
Anaesthesia. 2004 May; 59(5):440–452.
Wade DT, et al:. A preliminary controlled study to determine whether whole-plant cannabis extracts can improve intractable
neurogenic symptoms. Clin. Rehabil. 2003, 17, 21–29.Overview of diseases for which CBD may have therapeutic benefits taken from Pisanti et al (2017) Pisanti, S., et al., Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol Ther, 2017. 175: p. 133-150.
Cannabis: Affektive Störungen
1601 weibliche australische 14-15 jährige
Schülerinnen, follow-up 7 Jahre
5.6-faches Risiko für Depression und Angst bei
täglichem Konsum
2-faches Risiko für Depression und Angst bei
mindestens wöchentlichem Konsum
Depression und Angst im Teenageralter jedoch kein
Prädiktor für späteren THC-Konsum
www.seminare-ps.netCannabis: Risikofaktor für Schizophrenie?
Andreasson-Studie
2.4-faches Risiko für gelegentliche THC-
Konsumenten
6.0-faches Risiko für regelmässige THC-
Konsumenten
THC-Konsum als „live-event-stressor“ für Individuen,
die Vulnerabilität für Schizophrenie zeigen
Nach Follow-up von 27 Jahren erneute Analyse mit
gleichem Resultat, auch wenn man nur die Patienten
berücksichtigt, die erst 5-Jahre nach
Studieneinschluss Schizophrenie entwickelten
Zammit et al., 2002Cannabinoide
Nebenwirkungen:
Bei schneller Aufdosierung:
Tachycardie, Hypotonie,
Mundtrockenheit,
Schwindel, Ataxie, Bindehautreizung
Zentralnervöse Panikattacken, Angstsymptome
Erhöhte NW bei psychisch auffälligen Personen
Reduktion der Aufmerksamkeit, Feinmotorik, Kognition
Teerstoffe beim Cannabisrauchen stärker krebserregend (3-4 Joints
schädigen die Lunge wie ca. 20 Zigaretten)
Tipp für die Praxis: langsame Aufdosierung,
Einnahme eine Stunde nach dem EssenKontraindikationen für die Verwendung von Cannabis: • Herzinsuffizienz • Psychose (Vergangenheit oder Gegenwart) • Angststörung • Angehörige ersten Grades, die an psychischen Störungen leiden (insbesondere bei Personen unter 30 Jahren) • Geschichte von Drogenmissbrauch oder Sucht State of Israel Ministry of Health Medical cannabis Unit. http://www.health.gov.il/English/MinistryUnits/ HealthDivision/cannabis/Pages/default. aspx. Accessed 5 Apr 2015
Maida V, Daenick PJ, A user’s guide to cannabinoid therapies in oncology. Current Oncology. Vol. 23, No 6., December 2016.
Cannabis: Zusammenfassung II und persönliche Empfehlungen Persönliche Vorurteile (in jeder Richtung) ablegen Bedeutende Risikofaktoren (Schizophrenie, Psychosen, instabile ischämische Herzerkrankungen) in der Familienanamnese beachten Sorgfältiges Screening der Risikofaktoren für Substanzmissbrauch Genaue Erklärung der Medikamentenklasse (Substanz, Applikationsformen, Wirkweise, Nebenwirkungen) Mitbehandler und Familienmitglieder aktiv einbeziehen „Non Smoking“ Applikationsformen auswählen
Cannabis: Zusammenfassung II und persönliche Empfehlungen Alle Standardtherapien vor dem Einsatz von Cannabis evaluieren Einsatz bei Spastikschmerzen bei MS (und therapieresistenten Nervenschmerzen) Verwendung von qualitäts-kontrollierten Produkten Genauen Therapieplan (schriftlich) und Follow-up Strategien erstellen Bei fehlendem Therapieerfolg Beendigung der Therapie Cannabis Missbrauch mit extremer Dosissteigerung werden gehäuft gesehen – diese Patienten bedürfen einer Vorstellung beim Suchtspezialisten
THC; Auswirkungen auf Schmerzintensität und
„Unpleasantness“ (Unangenehmheit) im
Capsaicin-Modell
Lee MC, Ploner M, Wiech K et al: Amygdala activity contributes to the dissociative effect of cannabis on
pain perception Pain 154 (2013)
N=15, 24-34J, THC naiv, randomisiert, placebo-kontrolliert………
• THC reduced, the reported
unpleasantness, but not
the intensity of ongoing
pain and hyperalgesia:
• the specific analgesic effect
on hyperalgesia was
substantiated by diminished
activity in the anterior mid
cingulate cortex.
• In individuals, the drug-
induced reduction in the
un-pleasantness of
hyperalgesia was
positively correlated with
right amygdala activityKey Points
Evidence for the efficacy of medical cannabis for the treatment of various
symptoms, including pain, sleep disturbances, mood disorders and neurological
symptoms, in older adults is scanty.
Older adults have an increased risk of side effects from cannabinoids
because of their impaired metabolism, decreased reserves and the
potential for drug–drug interactions and comorbidities.
Despite the lack of high-quality supporting evidence, medical cannabis may
provide some benefits in selected older patients.
Any use of medical cannabis in older patients should be individualized and
account for the unique characteristics of each patient, including the symptoms
requiring treatment, symptom severity, comorbid conditions and possible
adverse effects. Patients and families should participate in clinical decisions
regarding medical cannabis only after an open and informative dialogue with
the treating healthcare team.
Minerbi A. et al.; Medical Cannabis for Older Patients: Drugs & Aging (2019) 36:39-51.Table 1 Possible indications for the use of cannabinoids in older individuals, and the level of evidence
supporting their use
Level of available evidence Indication
Low-quality evidence Neuropathic pain [54–56]; insomnia [53]; anxiety [69]
Non-statistically significant Cancer pain group [60, 61]; spasticity associated with
trend toward efficacy neurological diseases [53, 64, 66]
No evidence of efficacy Cancer-related anorexia, nausea and vomiting [71]; chronic non-
cancer pain (other than
neuropathic) [54–56]
Minerbi A. et al.; Medical Cannabis for Older Patients: Drugs & Aging (2019) 36:39-51.Table 2 Major adverse effects of cannabinoids pertinent to older patients
Domain Adverse effects pertinent to older patients
Psychomotor Impairment in gait and stability predisposes older patients to an
increased risk of falls and injuries and impairs their driving
skills [75, 77, 78]
Cognitive Impairment in short-term memory and emotional processing, which
may be particularly harmful in patients with pre-existing
cognitive impairment [75]
Cardiovascular Increased risk for myocardial infarction, sudden cardiac death,
arrhythmia, stroke and transient ischemic attacks [79–82]
Mental health Increased risk of psychotic episodes (arguably more pertinent to young
patients) and suicidality [84–86, 88, 90]
Minerbi A. et al.; Medical Cannabis for Older Patients: Drugs & Aging (2019) 36:39-51.Minerbi A. et al.; Medical Cannabis for Older Patients: Drugs & Aging (2019) 36:39-51.
Methods:
A prospective study that included all patients above 65 years of age who received medical
cannabis from January 2015 to October 2017 in a specialized medical cannabis clinic and were
willing to answer the initial questionnaire. Outcomes were pain intensity, quality of life and
adverse events at six months.
Results:
During the study period, 2736 patients above 65 years of age began cannabis treatment and
answered the initial questionnaire. The mean age was 74.5 ± 7.5 years.
The most common indications for cannabis treatment were pain (66.6%) and cancer
(60.8%). After six months of treatment, 93.7% of the respondents reported improvement in
their condition and the reported pain level was reduced from a median of 8 on a scale
of 0–10 to a median of 4. Most common adverse events were: dizziness (9.7%) and dry
mouth (7.1%). After six months, 18.1% stopped using opioid analgesics or reduced their
dose.
Conclusion:
Our study finds that the therapeutic use of cannabis is safe and efficacious in the elderly
population. Cannabis use may decrease the use of other prescription medicines,
including opioids. Gathering more evidencebased data, including data from double-blind
randomized-controlled trials, in this special population is imperative.
Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly:
European Journal of Internal Medicine 49 (2018) 44-50.Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly: European Journal of Internal Medicine 49 (2018) 44-50.
Table 1 Baseline characteristics of the patients at treatment initiation.
Variable Number of patients (N=2736)
Age (years) 65–74 – 1525 (55.7%)
75–84 – 885 (32.3%)
≥85 – 326 (11.9%)
Male 1273 (46.5%)
BMI 25.2 ± 5.0
Driving a car 986 (36.0%)
Approved monthly dosage of cannabis 28.8 ± 14.9
(grams)
Approved route of administration Oil - 737 (26.9%)
Inflorescence - 640 (23.4%)
Oil + Inflorescence – 1331 (48.6%)
Previous experience with cannabis 694 (25.4%)
Cigarettes smokers 424 (15.5%)
Number of regularly used medications 6 (3,9)
Number of days hospitalized in the past six 0 (0,9)
months
Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly:
European Journal of Internal Medicine 49 (2018) 44-50.Table 2 Indications for receiving cannabis prescription.
Indication Number of patients (N=2736)
Cancer associated pain 1001 (36.6%)
Nonspecific pain 821 (30.0%)
Cancer – chemotherapy treatment 661 (24.2%)
Parkinson's disease 146 (5.3%)
Others 49 (1.8%)
Post-traumatic stress disorder 21 (0.8%)
Crohn's disease 10 (0.4%)
Amyotrophic lateral sclerosis 9 (0.3%)
Compassion treatment 7 (0.3%)
Ulcerative colitis 5 (0.2%)
Alzheimer's disease 4 (0.1%)
Multiple sclerosis 2 (0.1%)
Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly:
European Journal of Internal Medicine 49 (2018) 44-50.Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly: European Journal of Internal Medicine 49 (2018) 44-50.
Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly: European Journal of Internal Medicine 49 (2018) 44-50.
Abuhasira R. et al.; Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly: European Journal of Internal Medicine 49 (2018) 44-50.
Table 3
Adverse events after six months of treatment with cannabis.
Adverse event Number of patients (N = 901)
Dizziness 87 (9,7%)
Dry mouth 64 (7,1%)
Somnolence 35 (3,9%)
Weakness 21 (2,3%)
Nausea 20 (2,2%)
Confusion and disorientation 17 (1,9%)
Drop in sugar levels 16 (1,8%)
Cough 13 (1,4%)
Headache 10 (1,1%)
Vomiting 10 (1,1%)
Sore throat 9 (1,0%)
Restlessness 8 (0,9%)
Hallucinations 7 (0,8 %)
Abuhasira R. et al.; Epidemiological characteristics, saftey and efficacy of medical cannabis in the elderly:
European Journal of Internal Medicine; 49 (2018) 44-50.THC:Dronabinol 3x2,5mg,Nabilone,Canemes 0,25-0,5mg CBD 2x100mg(max600-800mg) --- start low,go slow,
Zusammenfassung Cannabinoide sind bei Akutschmerz nicht wirksame Analgetika !! Cannabinoide zeigen analgetische Wirkung bei MS-assoziierten zentralen Schmerzen und anderen neurologischen Erkrankungen Cannabinoide beeinflussen die affektive Schmerzkomponente Cannabinoide - Coanalgetika bei chronischen(neuropathischen) Schmerzen! Cannabinioide in der Palliativmedizin zur Behandlung von Übelkeit,Erbrechen(CINV) und Appetitlosigkeit
Vielen Dank!
ABSTRACT
Numerous aspects of mammalian physiology exhibit cyclic daily patterns known as
circadian rhythms. However, studies in aged humans and animals indicate that these
physiological rhythms are not consistent throughout the life span. The simultaneous
development of disrupted circadian rhythms and age-related impairments suggests a
shared mechanism, which may be amenable to therapeutic intervention.
Recently, the endocannabinoid system has emerged as a complex signaling
network, which regulates numerous aspects of circadian physiology relevant to the
neurobiology of aging. Agonists of cannabinoid receptor-1 (CB1) have consistently
been shown to decrease neuronal activity, core body temperature, locomotion, and
cognitive function. Paradoxically, several lines of evidence now suggest
that very low doses of cannabinoids are beneficial in advanced age.
Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.One potential explanation for this phenomenon is that these drugs exhibit hormesisda
biphasic dose-response wherein low doses produce the opposite effects of higher
doses. Therefore, it is important to determine the dose-, age-, and timedependent
effects of these substances on the regulation of circadian rhythms and other processes
dysregulated in aging. This review highlights 3 fieldsdbiological aging, circadian
rhythms, and endocannabinoid signalingdto critically assess the therapeutic potential of
endocannabinoid modulation in aged individuals. If the hormetic properties of
exogenous cannabinoids are confirmed, we conclude that precise administration of
these compounds may bidirectionally entrain central and peripheral circadian clocks
and benefit multiple aspects of aging physiology.
Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.
Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.
Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.
Conclusions
Taken together, the findings discussed here suggest that altered circadian rhythms are a
potential biomarker of aging, and restoration or preservation of these rhythms in aged
individuals might benefit certain age-related pathologies. The endocannabinoid system is
a promising target in the treatment of age-related disease, given the diverse physiological
processes it regulates. Centrally, modulation of SCN activity by cannabinoids supports
their classification as a chronobiotics, and careful, therapeutic application use
of these compounds may serve to restore abnormal behavioral rhythms in aged subjects.
Moreover, the biphasic effects of cannabinoids on body temperature may allow for the
“tuning” of peripheral molecular clocks. Many additional experiments are necessary to
fully characterize the hormetic dose-response of exogenous cannabinoids such as THC
and examine their potential efficacy in the amelioration of age-related circadian
dysfunction. As societal opinions of "aging as a disease" and "cannabinoids as
medicine" shift, further inquiry of these previously intractable topics may prove greatly
beneficial to human health.
Hodges E. et al.; Aging circadian rhythms and cannabinoids: Neurobiology of Aging 79 (2019) 110-118.Table 1 An overview of randomized controlled trials (RCTs) involving medical cannabis for cancer pain
Reference Year Type of study Total subjects Treatment arms and doses Duration Outcome measure Pain response
Noyes et al. 1975 RCT 10 advanced cancer patients (I) THC: 5, 10, 15, and 20 mg in oil 6 hours Self-reported pain Correlation between higher
(13) capsules; (II) placebo severity, pain relief, side doses of THC and increased pain
effects, subjective relief (PAbstract:
The endocannabinoids system (ECS) has garnered considerable interest as a
potential therapeutic target in various carcinomas and cancer-related conditions
alongside neurodegenerative diseases. Cannabinoids are implemented in several
physiological processes such as appetite stimulation, energy balance, pain modulation
and the control of chemotherapy-induced nausea and vomiting (CINV). However,
pharmacokinetics and pharmacodynamics interactions could be
perceived in drug combinations, so in this short review we tried to shed light on the
potential drug interactions of medicinal cannabis. Hitherto, few data have been
provided to the healthcare practitioners about the drug–drug interactions of
cannabinoids with other prescription medications. In general, cannabinoids are usually
well tolerated, but bidirectional effects may be expected with
concomitant administered agents via affected membrane transporters (Glycoprotein p,
breast cancer resistance proteins, and multidrug resistance proteins) and metabolizing
enzymes (Cytochrome P450 and UDP-glucuronosyltransferases). Caution should be
undertaken to closely monitor the responses of cannabis users with certain drugs to
guard their safety, especially for the elderly and people with chronic diseases or kidney
and liver conditions.
Alsherbiny M. et al.; Medicinal Cannabis – Potential Drug Interactions: Medicines 2019, 6, 3.Table 1. Recent clinical studies of cannabinoids in oncology patients.
Cannabis Based Treatment Study Type/Location/n Dosage/Administration Efficacy, Tolerability and Notes References
Chemotherapy Induced Nausea and Vomiting (CINV)
Dronabinol [Marinol®; Interventional (Placebo Both were effective in CINV and well
(-) trans D9-THC) alone or in combination controlled). Capsule (2.5–20 mg). tolerated while dronabinol was [23]
with ondansetron (8–15 mg IV] n = 64. Oral. more effective.
USA. Combination is not more effective.
Dronabinol [Marinol®; Interventional (retrospective). Solution administered orally Positive response were reported for 60%
(-) trans D9-THC] Children with malignancy. (2.5–5 mg/m2 body surface of patients.
every 6 h as needed). Prospective trial would be needed to [24]
confirm the dronabinol effect in
CINV therapy.
Nabilone with 5HT3 antagonist Interventional (retrospective) Adverse effect was reported with minor
n = 110 with median age 14 Oral clinical significance.
years with malignancy. Poor nausea control in nabilone
treated group.
Cancer Pain
Sativex® Interventional (Double Blind, Oromucodal spray with Compared with the placebo, the Sativex
(D9-THC: CBD at a ratio of 27:25 mg/mL) Randomized, Parallel Group, maximum D9-THC: CBD treated group showed significant pain
THC (27 mg/mL) Placebo Controlled), n = 177. (130:120 mg/day) or 130 relief unlike the D9-THC which was
Phase 3. mg/day D9-THC alone non-significant.
UK. Each actuation is 100 L. Reported adverse effects including
dizziness, gastrointestinal disorders
and confusion.
Sativex® Interventional (single group Oromucodal spray with The long-term use is well tolerated
(D9-THC: CBD at a ratio of 27:25 mg/mL) assignment) maximum 130:120 mg/day of without losing pain-relieving effects in
Phase 3. D9-THC: CBD. terminal cancer-related pain refectory
UK. to opioids.
Adverse effects and tolerability assessed
at the RCT withdrawal visit, 7–10 days
later, then monthly, and at the
withdrawal or completion of the study.
Alsherbiny M. et al.; Medicinal Cannabis – Potential Drug Interactions: Medicines 2019, 6, 3.Table 1. Cont.
Cannabis Based Treatment Study Type/Location/n Dosage/Administration Efficacy, Tolerability and Notes References
Cancer Pain
No significant difference was reported in
advanced cancer patients with chronic
pain (unalleviated with opioids).
Interventional (Double Blind, Oromucodal spray (100 L per Nabiximol still beneficial to secondary [28]
Sativex® Randomized, Parallel Group, actuation twice daily in the endpoints.
(D9-THC: CBD at a ratio of 27:25 mg/mL) Placebo Controlled). morning and evening with a No evidence of abuse or misuse
Phase 3. maximum of 10 sprays for was reported.
Multicentric. 5 weeks). No significant difference was reported in
n = 399. advanced cancer patients with chronic [29]
uncontrolled pain.
Interventional (Double Blind,
Randomized, Parallel Group, Oromucodal spray in low Efficacy and safety were reported at low
Placebo Controlled). (1–4 sprays/day), medium and medium doses against advanced [30]
Nabiximols (Sativex®; D9-THC: CBD at Phase 2. (6–10 sprays/day) and high cancer pain.
a ratio of 27:25 mg/mL) USA. (11–16 sprays/day) doses. The adverse effects at high doses.
n = 360.
Interventional (Double-Blind, No significant difference was reported
Placebo controlled, Crossover Sublingual spray against chemotherapy-induced
Nabiximols (Sativex®, D9-THC: CBD at Pilot trial). (7.5–30 mg/day). neuropathy. [31]
a ratio of 27:25 mg/mL) n = 16. Two-fold reduction of the pain in the
responder group with adverse effects.
Cannabis cigarettes (3.56% D9-THC) in Interventional (open label). Pulmonary administration for Declined chronic pain around 27% in
combination with opiates chronic pain, including cancer patients receiving oxycodone or [32]
patients. morphine analgesics.
No serious adverse effects were reported.
5HT3; 5-hydroxytryptamine 3 receptors, D9-THC; Delta -9 tetrahydrocannabinol, CBD; Cannabidiol, CINV; Chemotherapy induced Nausea and Vomiting, IV; Intravenous, n; number of
participants, RCT; Randomised controlled trial.
Alsherbiny M. et al.; Medicinal Cannabis – Potential Drug Interactions: Medicines 2019, 6, 3.Table 2. Overview of the recent reviews of the drug–drug interactions with cannabinoids.
Cannabinoid Based Treatment Affected Transporters and/or Experimental Results, Notes and Outcomes References
and Interactions Metabolic Enzymes P-gp, BCRP, and MRP1-4 transporters expression were dysregulated by cannabinoids, but in higher
concentrations than that usually measured in cannabis smokers.
CYP3A was competitively inhibited by THC, CBD and CBN, with CBD being the most potent in a
Membrane transporters ABC super concentration compatible with that in usual cannabis inhalation.
family (glycoprotein P; P-gp, Breast CYP2D6 was inhibited by THC, CBD and CBN, with CBD being the most potent in a higher
cancer-resistance protein; BCRP, and concentration than that in usual cannabis consumption.
Cannabis, THC, CBD, CBN multidrug resistance protein; MRP1, 2, 3 CYP2C9 was inhibited by THC, CBD and CBN, with CBD inhibitory effect being dependent on the [17,50,51]
with either chemotherapies, and 4) used substrates.
abuse drugs or medications Cytochrome P450 (3A, 2D6, 2C9, 1A1, CYP1A1, 1A2, 1B1, 2B6, 2C19, 3A4 and 2C8 were strongly inhibited by CBD.
1A2, 1B1, 2B6 and 2C8) UGT1A9, and 2B7 were inhibited by CBD.
UDP-glucuronosyltransferases (UGTs) UGT1A7, 1A8, and 1A9 were inhibited by CBN.
UGT2B7 was activated by CBN.
Cannabinoids and drugs with inhibitory or stimulatory effects on UGT2B7 will interact.
Clinical studies are warranted to explore the potential interactions with chemotherapy, alcohol,
D9-THC, CBD and marijuana abuse drugs, and prescription medications.
inhalation with Cytochrome P450 CYP2C9 and CYP3A4 were inhibited by D9-THC.
psychotropic agents CYP2C19 and CYP3A4 were inhibited by CBD.
CYP1A1 and CYP1A2 were induced by marijuana inhalation.
Cannabinoids consumption via pyrolysis induced CYP due to aromatic hydrocarbons. [52]
D9-THC, CBD and marijuana The effect of cannabinoids on the CYP activity influenced by the formulation, administration route,
inhalation with and derivation (Plant based or synthetic).
psychotropic agents Cytochrome P450 Clinical studies are warranted to explore the potential drug–drug interactions with cannabinoids.
CYP3A4 inhibitors and stimulators affect the elimination of D9-THC and CBD.
Reviewed the pharmacokinetic interactions between cannabinoids on other drugs.
Limited data on the drug’s effects on the accumulation of cannabinoids and marijuana. More [53]
clinical studies are warranted.
Clinical studies of DDI:
Non-significant increase of the clobazam plasma level administered with CBD (n = 13 children) due to
potent inhibition of CYP2C19.
Significant change of plasma level of N-desmethylclobazam by CBD co-administration while no
significant change in the level of valproate, stiripentol and levetiracetam (n = 24 open label trial).
All patients showed significant changes of the plasma levels of clobazam, N-desmethylclobazam,
CBD with antiepileptic drugs Cytochrome P450 or unknown rufinamide, and topiramate by increasing CBD doses. The mean therapeutic range was exceeded for [47,54]
clobazam and N-desmethylclobazam; the plasma levels of eslicarbazepine and zonisamide were
increased in adults only (n = 39 adults and 42 children).
The purified CBD formula is FDA approved with antiepileptic drugs as a result of the published
randomized clinical trials.
CBD is well tolerated with potential DDI and adverse effects.
The compulsory monitoring drug levels and patients’ liver functions are advised.
Alsherbiny M. et al.; Medicinal Cannabis – Potential Drug Interactions: Medicines 2019, 6, 3.Table 2. Cont.
Cannabinoid Based Treatment Affected Transporters and/or Experimental Results, Notes and Outcomes References
and Interactions Metabolic Enzymes
CYP1A catalysed MROD activity was weakly inhibited by MAM-2201, JWH-019, STS-135, and UR-
144.
CYP2C8 catalysed amodiaquine N-deethylase was strongly inhibited by AM-2201, MAM-2201,
and EAM-2201.
CYP2C9 catalysed diclofenac hydroxylation and CYP3A-catalyzed midazolam 10-hydroxylation
were
inhibited by AM-2201 and MAM-2201.
CYP2C9 catalysed diclofenac 40-hydroxylation, CYP2C19-catalyzed [S] -mephenytoin 40-hydroxylation,
Synthetic and Cytochrome P450 and CYP3A-catalyzed midazolam 10 hydroxylation were strongly inhibited by EAM-2201
Phyto-cannabinoids UGTs (time-dependent inhibition).
CYP2B6 and CYP2C9 were strongly inhibited by THC, CBN and CBD.
CYP2A6 was inhibited by THC and CBN (mechanism-based inhibition).
CYP2D6 was competitively inhibited by CBD.
CYP1A1 mRNA expression was increased by THC in Hepa-1 cells, but EROD activity in CYP1A1 [55,56]
supersomes was inhibited by THC.
CYP1A1, CYP1A2, and CYP1B1 were strongly inhibited by CBD (mechanism-based inhibition).
CYP3A was inhibited by CBD in human liver microsomes.
CYP2C19-catalyzed [S] -mephenytoin hydroxylation was inhibited by (CBD and THC
(Mixed-type inhibition).
UGT1A9- and UGT2B7 catalysed ethanol glucuronidation were non-competitively inhibited by
CBD,
and unlike the inclined ethanol glucuronidation in human liver microsome by CBN (dose dependent).
UGT1A3 catalysed chenodeoxycholic acid 24-acylglucuronidation was strongly competitively inhibited
by AM-2201, MAM-2201, and EAM-2201.
UGT2B7-mediated naloxone 3-D-glucuronidation was competitively inhibited by AM-2201.
Clinical studies of pharmacokinetics mediated drug interactions of synthetic and
phyto-cannabinoids with the CYP and UTGs substrates are warranted.
ABC; ATP-binding cassette, AM-2201, EAM-2201, MAM-2201, JWH-019, STS-135, and UR-144; Synthetic cannabinoids, BCRP; Breast cancer resistance proteins, CBD;
Cannabidiol,
CBN; cannabinol, CYP; Cytochrome P450, DDI; drug–drug interactions, MROD; 7-methoxyresorufin O-demethylation, MRP; Multidrug resistance proteins, P-gp; Glycoprotein P,
THC;
tetrahydrocannabinol, UGTs; UDP-glucuronosyltransferases.
Alsherbiny M. et al.; Medicinal Cannabis – Potential Drug Interactions: Medicines 2019, 6, 3.Sie können auch lesen