ANÄMIE Jörg Halter Klinik für Hämatologie Universitätsspital Basel - medArt basel
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
ANÄMIE Jörg Halter Klinik für Hämatologie Universitätsspital Basel
Anämie – Definition in Praxis:
Verminderte Hämoglobinkonzentration
- Häufig einhergehend mit verminderter Erythrozytenzahl und -masse
162.0
Hb g/l Männer Frauen Ø Residential
Altitude (masl)
160.0
Mean Hb (g/l)
Hb ≦ Hb ≦ (1500,2000] (4)
(1200,1500] (14)
(900,1200] (35)
158.0
156.0
(600,900] (134)
WHO 130/140 120/120 (300,600] (491)
[200,300] (27) 154.0
Ø Hemoglobin (g/l) 152.0
1 140 120 (152.1-154.2] (34)
(154.2-155.2] (98)
(155.2-156.0] (163)
0 500 1000 1500
Altitude (masl)
2000
(156.0-156.6] (139)
2 135 121 (156.6-157.4] (132)
(157.4-159.0] (102)
(159.0-162.1] (37)
3 134 117
4 140 120
5 135 120
6 127 115
®Wohnort? Figure 1. Hemoglobinography: Hb concentrations mirror the topography of Switzerland. Map of 705 MedStat regions that represents the official geographical region
allowing an anonymous indication of a place of residence for each person hospitalized in Switzerland. The map shows the conscripts’ average residential altitude, as well
®Hinweise für Expansion Plasmavolumen average Hb level (circle size proportional to sample size, Nmin 5 12, Nn , 30 5 12, Nmax 5 335, Nmean 5 102). The numbers in parentheses following the altitudes in the legend ke
indicate the number of MedStat regions in that particular category. The scatterplot (inset) shows the same MedStat data (altitude vs Hb). The solid red line indicates a smoothe
local polynomial trend (bandwidth 5 100 masl), the yellow dashed line is a linear fit, and the size of the circle is proportional to sample size.
(Schwangerschaft, andere)
® Hypovolämie?
Ferritin increased significantly with altitude (Figure 2D), whereas linear increase of 3 g/L for every 500-meter increase in altitud
the odds ratios for elevated CRP did not (Figure 2C). This is between 1 and 2000 masl.5 The differences may be due to th
important because systemic inflammation has a profound impact narrower study population in our case (only young men i
® Raucher? on hematopoiesis, gastrointestinal iron absorption, and ferritin
plasma levels. To assess whether increased ferritin serum
8,9
Switzerland), decreasing sample size at altitudes $1500 mas
and the fine-grained modeling.
® Individueller Hb-Verlauf/Trend? levels, a marker for body iron stores, directly depend on a
concomitant increase in Hb concentrations, we analyzed the Because Hb concentrations are primarily regulated by the ce
interrelationship among altitude, Hb, ferritin, CRP, and BMI. lular oxygen sensor mechanism involving the prolyl-hydroxylase
Analysis of conscripts with normal Hb concentrations (,175 g/L), 2–hypoxia-inducible factor-2 (HIF-2)–erythropoietin (Epo) axis,
normal CRP (,5.0 mg/L), and normal BMI (18.5-24.9 kg/m2) Staub K et al. Blood 2020;135:1066-1069
our observation implies that the oxygen sensor is very precise
revealed that ferritin levels still increased significantly with alti- enabling detection of even subtle changes in oxygen at low t
tude (Figure 2E). We further plotted average ferritin levels within moderate altitude. We hypothesize that the oxygen-sensinErythropoiese
Erythropoietin EPO
TSH Für Kompensation
Androgene Abbau/Verlust:
+
Substrate Produktion von ca.
- Eisen 50‘000 Retikulozyten/ul,
- Vitamin B12 bzw. 5x1010/L
- Folsäure
+ Falls genügend Substrate
„gesundes“ und adäquater EPO-Anstieg:
Knochenmark Erythropoiese kann ca. 5fach
(Gene, Nische) gesteigert werden –350‘000
Retikulozyten/ul, bzw.
Normales Hämoglobin 3.5x1011/LAbklärung Anämie - erste Schritte ¨ Anamnese, Herkunft ¨ Komplettes Blutbild inkl. Handdifferenzierung ¨ Retikulozyten
Komplettes Blutbild, Retikulozytenzahl, MCV
MCV Retikulozytenzahl Retikulozytenzahl
tief oder normal erhöht
Mikrozytär Eisenmangel Thalassämie
MCV < 80 fl Entzündungsanämie (anemia of chronic Hämolyse
disease/inflammation)
Sideroblastische Anämie
Kupfermangel, Zinküberdosis
Normozytär Akute Blutung Blutung
MCV 80-100 fl Eisenmangel Hämolyse
Entzündungsanämie KM-Erholung nach
KM-Insuffizienz (Infiltration, aplastische Anämie, - Infekt
Infekt) - Vit.B12 oder
Chronische Niereninsuffizienz Folsäuresubstitution
Hypothyreose - Eisensubstitution
Hypopituitarismus
Alkohol
Makrozytär Vitamin B12 oder Folsäuremangel Hämolyse
MCV > 100 fl Alkohol KM-Erholung nach
Myelodysplastisches Syndrom - Infekt
Hepatopathie - Vit.B12 oder
Hypothyreose Folsäuresubstitution
HIV - Eisensubstitution
Medikamente (Hydroxyurea, MTX, etc.)Differentialdiagnose Anämie
Verminderte Produktion Vermehrter Verbrauch
Substratmangel Verlust
- Eisen
- Vitamin B12
- Folsäure Extravasal – Blutung
Entzündungsanämie
(anemia of chronic Intravasal/extravaskulär - Hämolyse
disease/inflammation) Korpuskulär/hereditär:
Hormonmangel - Sphärozytose
- Erythropoietin - Sichelzellanämie/Thalassämie
- Hypothyreose - Enzymdefekte
Ineffektive Erythropoiese Extrakorpuskulär/erworben:
- Thalassämie - AIHA, Kälteagglutinin-Krankheit
- MDS - Mikroangiopath.hämolytische A.
- Seltene kongenitale/ (MAHA)
erworbene Formen - PNH
Aplastische Anämie/PRCA - Hypersplenismus
Verdrängung/KM-Infiltration - Medikamentös
MedikamentösErste Schritte ¨ Anamnese, Herkunft ¨ Komplettes Blutbild inkl. Handdifferenzierung ¨ Retikulozyten ¨ Eisenstatus, Vitamin B12, Folsäure im Ec ¨ Coombstest, Haptoglobin, Bilirubin, LDH ¨ (Hb-Elektrophorese) ¨ CRP, Kreatinin, Leberwerte ¨ Erythropoietin, TSH ¨ Serum-Eiweisselektrophorese ¨ Hämatologisches Konsilium
Blutbild 18-jährige Frau
Resultat Referenz Diagnose:
Hämoglobin 65 120-160 g/l Eisenmangelanämie
Erythrozyten 1.9 4.2-6.3x1012/l
MCV 59 79-95 fl weitere Diagnostik:
MCHC 271 320-360 g/l Junge gesunde Frau: keine
Retikulozyten 17 10-28 %o
Postmenopausale Frauen
72 40-140x109/l und alle Männer: nach
Ursache suchen
Ferritin 5 10-200 ug/l
Transferrin 4.2 2.0-3.6 g/l
Transferrin-Sättigung 2 16-45%
Löslicher 5.5 1.9-4.4 mg/l
Transferrinrezeptor
sTfRTherapie Eisenmangelanämie
Ursachenbehandlung → Beginn Eisensubstitution schon vor workup möglich
EK-Transfusionen nur wenn klinisch rasche Hb-Korrektur notwendig
Eisensubstitution:
- In der Regel oral vor parenteral
- Orale Eisensubstitution:
- Mehrere Präparate, keines dem anderen wirklich überlegen
- Kalziumreiche Diät vermeiden (leerer Magen)
- Vitamin C kann Eisenabsorption steigern
- Dosis: 80-100mg
- Dauer: ca. 6 Monate (Korrektur Anämie und Auffüllen der Speicher)
Parenterale Eisensubstitution
- Eisen-Saccharose (Venofer): 100mg 1-3x/Woche, max. 200mg/Dosis
- Eisen-Carbomaltose (Ferinject): 500-1000mg/Woche
- Gesamtdosis Eisen i.v. (mg)
= [Ziel-Hb (g/dl) – Ist-Hb (g/dl)] × Körpergewicht (kg) × 2.4 + Eisendepot (mg)
= [Ziel-Hb (g/L) – Ist-Hb (g/L)] × Körpergewicht (kg) × 0.24 + Eisendepot (mg)
Depot für Erwachsene ca. 500mg
- AnaphylaxieTherapie Eisenmangelanämie Nach Eisensubstitution: - Retikulozytenkrise nach 7-10 Tagen - Hb-Anstieg nach 2-3 Wochen (ca. 10-20g/l alle 3 Wochen nach oraler Eisensubstitution) - Serum-Ferritin Kontrolle nach (8-)12 Wochen sinnvoll
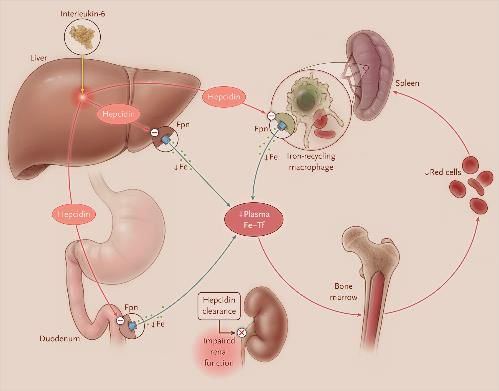
Entzündungsanämie
Anemia of inflammation (anemia of chronic disease)
Assoziiert mit chronisch
entzündlichen Krankheiten:
- (Auto)Immunkrankheiten
- Infekte
- Tumoren
- Chronische Niereninsuffizienz
- Chronische Herzinsuffizienz
- COPD
- Adipositas
IL-6 ® Hepcidin verhindert Eisenexport
® Absorption in Darm¯
® Freisetzung aus Makrophagen¯
® Zusätzlich: Ec-Lebensdauer ca. 25% verkürzt
Ganz T. NEJM 2019;381:1148-1157; Weiss G et al. Blood 2019;133:40-50Entzündungsanämie - Diagnostik
AI Eisenmangel
Hb 70-120 g/l variabel
MCV normal tief
MCH normal tief
…in practice, these markers are
least helpful when they are most
Retikulozyten tief tief
needed…
Ferritin (normal-) tief
hoch ® ca. 20-80% der Patienten
sTfR normal hoch haben eine Kombination von
Transferrin tief hoch Entzündung und Eisenmangel
Transferrin- tief tief
Sättigung
Hepcidin hoch tiefEntzündungsanämie - Therapie
Korrektur der Anämie notwendig/sinnvoll?
→ Suche nach potentiell zugrunde liegenden Krankheiten und okkultem Blutverlust
→ Behandlung Grundkrankheit – z.B. Steroide/Biologica, Antiinfektiva, etc.
Falls notwendig: pragmatischer Ansatz:
Probatorischer Eisenersatz (diagnostisch/therapeutisch) mit/ohne Erythropoietin
- Parenterale Eisensubstitution – berechnen wie wenn Eisenmangel, dann halbe Dosis
substituieren, kleinere Dosen(200mg) möglicherweise effizienter – Hb-Anstieg
innerhalb 4 Wochen zu erwarten
- Orale Eisensubstitution: bei schwerer Entzündung unwirksam
- Erythropoetin (nicht zugelassen für diese Indikation)
- Ziel-Hb 100-110g/L
Evtl. zusätzlich Vitamin B12, Folsäure45-jähriger Patient 24-jährige Patientin
Resultat Referenz Resultat Referenz
Lc 6.9 3.5-10x109/l Lc 6.24 3.5-10x109/l
Hb 80 140-180 g/l Hb 93 120-160 g/l
Ec 2.4 4.5-6.3x1012/l Ec 2.76 4.2-5.4x1012/l
MCV 119 79-95fl MCV 97 79-95fl
Tc 150 150-450x109/l Tc 37 150-450x109/l
Reti 108 10-27%o Reti 122 10-27%o
258 40-140x109/l 338 40-140x109/l
Bilirubin 4745-jähriger Patient 24-jährige Patientin
Resultat Referenz
Fragmentozyten +++ -
ADAMTS-13Take home message
¨ Eisenmangelanämien sind häufig, andere
Anämieursachen kommen vor
¨ Retikulozyten gehören zum Start jeder
Anämieabklärung
¨ Multifaktorielle Ursachen sind häufig
¨ Hämatologische Notfälle:
- Autoimmunhämolytische Anämie
- Coombs-negative hämolytische Anämie mit Thrombopenie
- Anämie mit Protein >100g/l → Hyperviskosität? cave
Erythrozytentransfusionen!Nützliche Literatur und Quellen
¨ www.hematool.ch
¨ Nowak A et al. Swiss Delphi study on iron deficiency. Swiss Med Wkly.
2019 Jul 3;149:w20097
¨ Ganz T. Anemia of Inflammation. N Engl J Med 2019 Sept
19;381(12):1148-1157Sie können auch lesen