Notfallmedizin Gerinnungsmanagement in der - Clemens Feistritzer
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Gerinnungsmanagement in der
Notfallmedizin
Clemens Feistritzer
Medizinische Universität Innsbruck
Klinik für Innere Medizin V - Hämatologie & Onkologie
Hall - 28. September 2018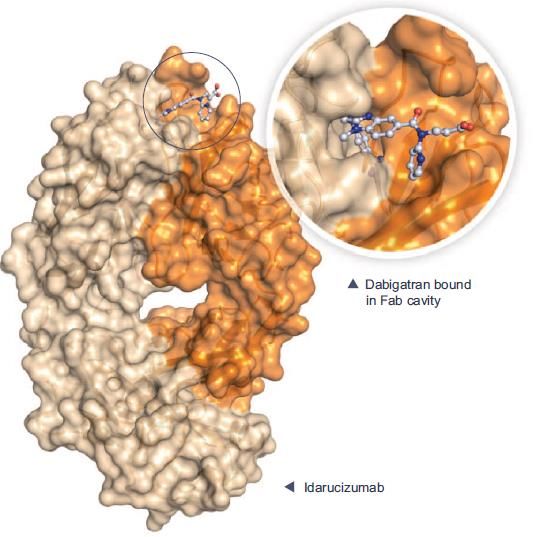
Gerinnungsmanagement in der Notfallmedizin • Transfusion-Management und Gerinnungsstörungen • Blutungen unter oraler AK-Therapie • Leberzirrhose und Blutungen
Pathogenese von Gerinnungsstörungen bei
Patienten nach Polytrauma
Rossaint et al. Critical Care (2016) 20:100.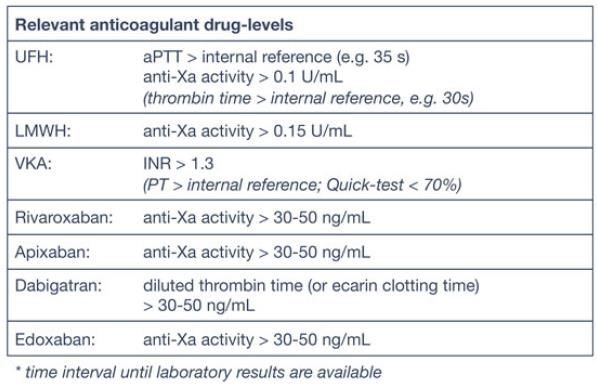
Prähospitale Volumengabe vs. Häufigkeit
von Gerinnungsstörungen
Daten: Retrospektive Analyse Deutsches Trauma Register DGU 2002 -2014.
Maegele M et al. Eur J Trauma Emerg Surg. 2017 Aug;43(4):439-443.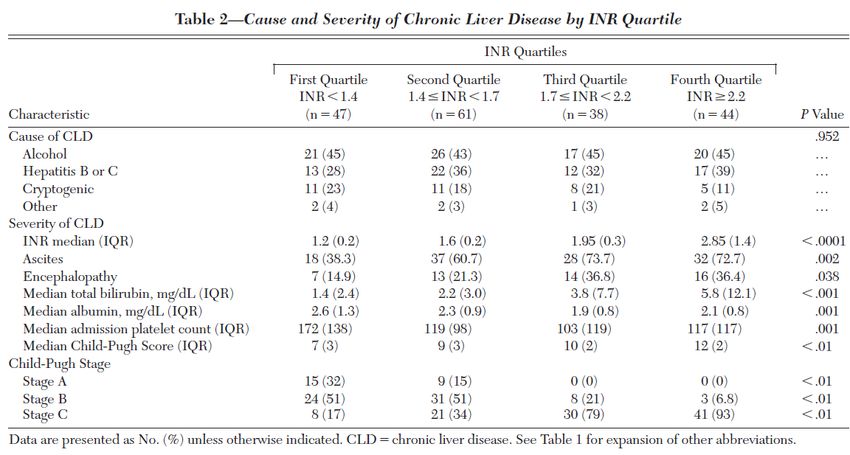
Tissue Oxygenation
We recommend a target systolic blood pressure of
80–90 mmHg until major bleeding has been stopped
in the initial phase following trauma without brain
injury. (Grade 1C)
Kaske S et al. Unfallchirurg 2017;120:85–90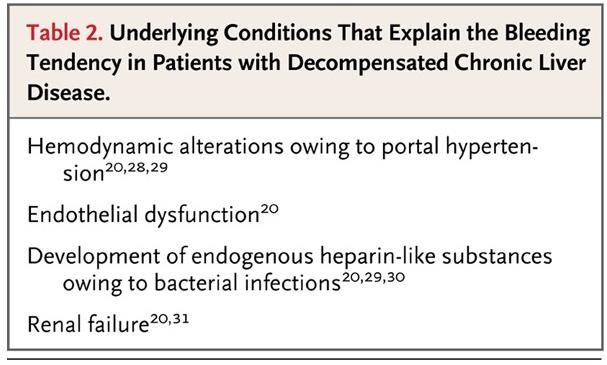
Volumengabe: Perfusion vs. Steigerung des
Blutverlusts
Restricted volume replacement
We recommend use of a restricted volume replacement
strategy to achieve target blood pressure until bleeding
can be controlled. (Grade 1B)
In patients with severe Traumatic Brain Injury (GCS ≤8),
we recommend that a mean arterial pressure ≥80 mmHg
be maintained. (Grade 1C)
Kaske S et al. Unfallchirurg 2017;120:85–90
Type of fluid
We recommend that fluid therapy using isotonic
crystalloid solutions be initiated in the hypotensive
bleeding trauma patient. (Grade 1A)
We suggest that excessive use of 0.9 % NaCl solution
be avoided. (Grade 2C)
Bollinger D et al. Br J Anaesth 2010 104:318–325
Fries D et al. British Journal of Anaesthesia 2005 95 (2): 172–7
Kaske S et al. Unfallchirurg 2017;120:85–90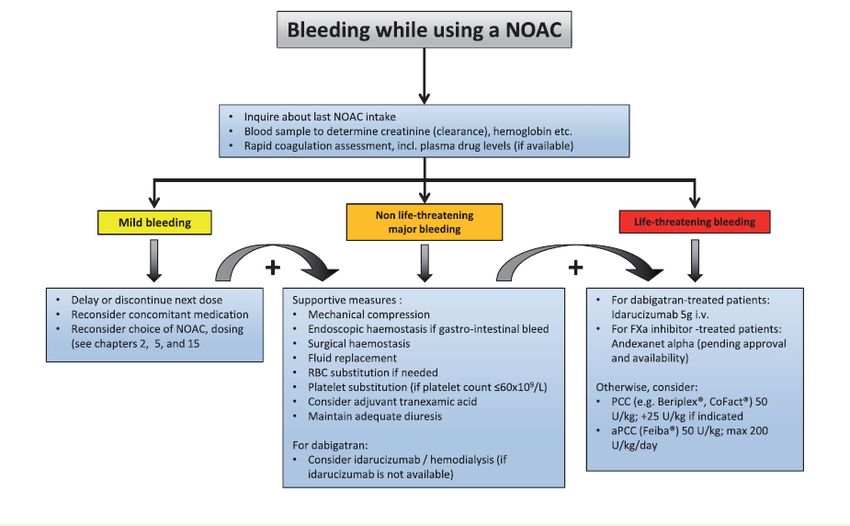
Temperature management
We recommend early application of measures to
reduce heat loss and warm the hypothermic patient
in order to achieve and maintain normothermia.
(Grade 1C) Rossaint et al. Critical Care (2016) 20:100.
• Pro Grad C Körpertemperaturreduktion Verminderung der plasmatische Gerinnung um
5%
• Ab einer Körpertemperatur von 30 °C findet bei 75 % der Menschen keine Interaktion
zwischen von-Willebandt-Faktor und Glykoproteinen zur Thrombozytenaktivierung mehr
statt Kermode JC et al. Blood 1999 94:199–207
• Thrombozytenadhäsion respektive -aggregation bei einer Körpertemperatur von 33–
37 °C signifikant reduziert
• Köpertemperatur> 33 °C -> Abnahme der enzymatischen Aktivität der plasmatischen
Gerinnung mit erhöhter fibrinolytischer Aktivität Wollberg AS et al. J Trauma 2004 56:1221–1228
Retrospektive Analyse - 38.520 schwerverletzten Patienten - Körpertemperatur von 3-fach erhöhten Mortalität assoziiert ist
Wang HE et al. Crit Care Med 205 33:1296–1301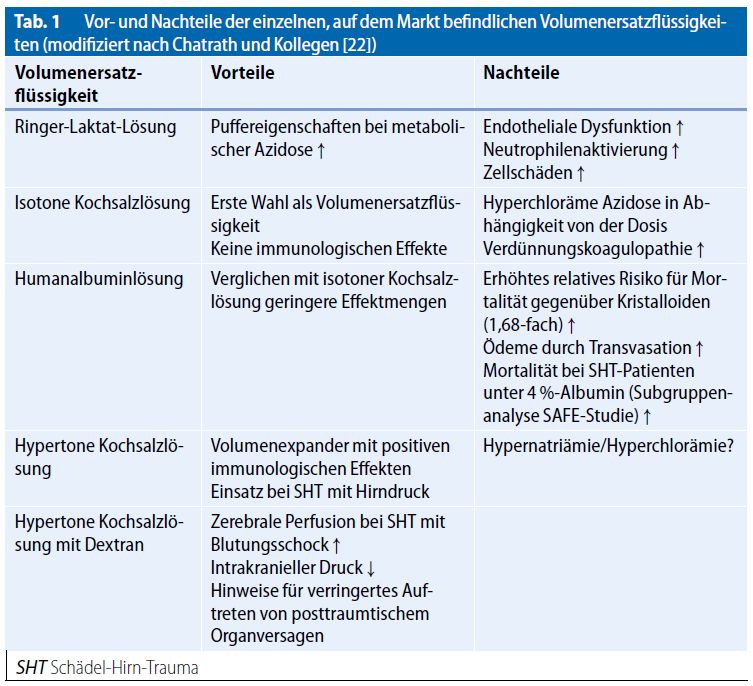
Gerinnungsmanagement des Trauma-Patienten
Rossaint et al. Critical Care (2016) 20:100.Gerinnungsmanagement in der Notfallmedizin • Transfusion-Management und Gerinnungsstörungen • Blutungen unter oraler AK-Therapie • Leberzirrhose und Blutungen
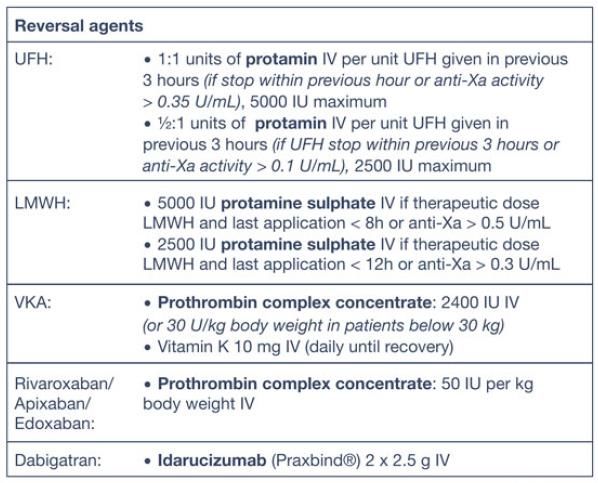
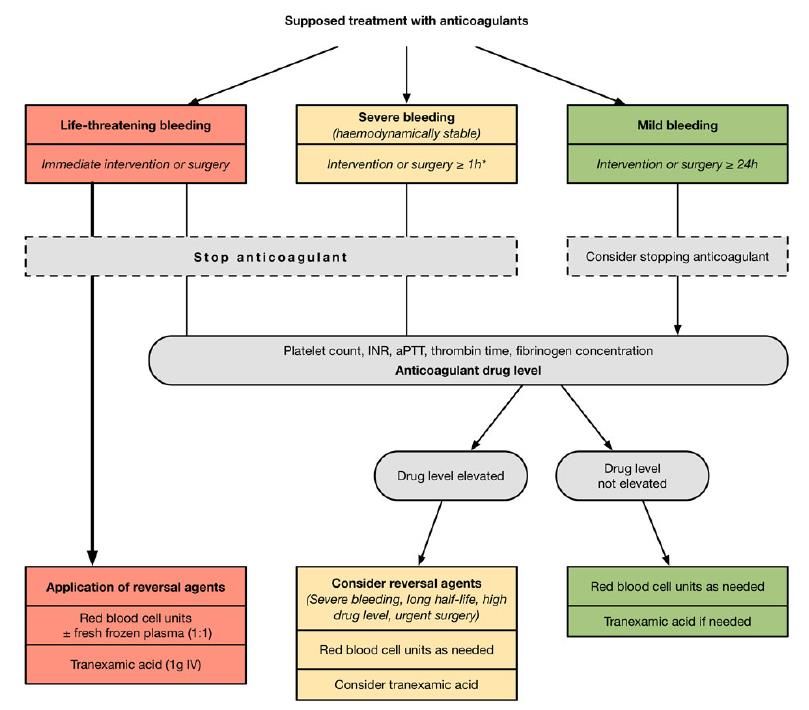
Procedere bei Blutungen unter Antikoagulation
PCC als Antidot für VKA-assoziierte intracerebrale
Blutungen
• Prospektive multizentrische
Studie 2008-2010
• 141 Patienten
• Mittl. Alter 78a
• 59.6% Männl
• Rankin Score bei Aufnahme 1 –
42% bei Entlassung 5
• In-hospital - Mortalität: 42.3%
• In 45% der Fälle Hämatom-
Zunahme trotz PCC Gabe
Dowlatshahi D et al; Stroke 2012, 1812-17Risiko für thromboembolische Ereignisse nach
Reversal von Blutungen unter Vit K Antagonisten
• Meta-Analyse – 27 Studien (1032 Pat)
Dentali F et al, Thromb Haemost 2011, 106; 429-38Blutungen unter NOACs
Steffel J. et al. European Heart Journal (2018) 39, 1330–1393In Notfallsituationen: Kurze Halbwertszeit von Vorteil
Heidbuchel et al. Europace 2015 Oct;17(10):1467-507Kein Einfluss von PCC auf NOAC-assoziierte
intracerebrale Blutungen
• Prospective multizentrische Studie
– 38 Zentren/Deutschland
• 61 Patienten – 41% Frauen
• Alter (mean) 71.1a
• Mortalität: 28%
• Schlechtes neurologisches
Outcome (Rankin – Skala 3-6: 65%)
• 57% PCC (mean dose 2390IU) –
Physicians choice
Purrucker JC et al JAMA Neurol. 2015 Dec 14:1-10Spezifische Antidot für NOAKs – Entwicklungsstatus
Phase III
IDARUCIZUMAB 1 Patienten mit EMA11/2015
Praxbind® Phase I Phase II FDA10/2015
Akutsituation (Blutung,
Angriffspunkt: Zulassung
Noteingriff)
Dabigatran
abgeschlossen
2. Clinicaltrials.gov: NCT02104947; 3. Pollack CV et al NEJM 2015, 373: 511-20
Andexanet alfa Phase III
(PRT064445) 1 Patienten mit FDA 2018
Phase I Phase II EMA ?
Angriffspunkt: Blutung;
FXa inhibitoren Jan 20154
4. ClinicalTrials.gov Identifier: NCT02329327
Ciraparantag
(PER977) 1 Phase II
Phase I
Angriffspunkt: Ongoing 5
universal
5. ClinicalTrials.gov Identifier: NCT02207257
Adapted from Greinacher et al. Thromb Haemost 2015, 113; 921-42Idarucizumab (Praxbind®) - Eigenschaften
Fully humanized
Wiederherstellung der Gerinnung antibody fragment (Fab)
Hohe Bindungsaffinität: ~350 Mal höher als von
Dabigatran zu Thrombin;
Keinen pro- oder antithrombotischen Effekt
i.v. Applikation als Kurzinfusion
Rascher Anstieg („peak post infusion“)
Kurze Halbwertszeit (Initiale HWZ ~45 Minuten)
Geringes Risiko für (milde)
Nebenwirkungen
Elimination
vorwiegend renaler Katabolismus
Glund S et al; Lancet 2015, 386; 680-90; Glund S et al. Thromb Haemost 2015, 113; 943-51Idarucizumab – Wirksamkeit auch nach
wiederholter Gabe
80 / 45–64 yr, DE 220 mg
/ 45–64 yr, DE 220 mg
75 + idarucizumab 5 g 1. Dabigatran bewirkt 24h
nach Idarucizumab Gabe
70
effektive
65
Peak
Gerinnungshemmung
60
2. Idarucizumab auch bei 2.
dTT (s)
55 Anwendung wirksames
50
Antidot gegen Dabigatran
Trough
45
40
35
30
−2
-2
0 0 20 4 0
6 8 10
0 12 14
0 16 18
0 20 22
0 24 26 36
28 48
30 32 34 74
60 72 36
Restart DE
Time after end of infusion (h)
N=6-8/group, mean ± SE
Glund et al. ASH 2014; Glund et al. Lancet 2015; Glund S et al. Thromb Haemost 2015RE-VERSE AD™ Studien - Design
einarmig, offen; Einschluss von 503 Patienten (Alter >18a)
173 Zentren – 39 Länder
5 g Idarucizumab
Gruppe A (2 separate Infusionen zu 2.5 g)
(n=301):
Schwere
Blutung*
(*Lebensbedrohlich, nicht kontrollierbar)
5 g Idarucizumab
(2 separate Infusionen zu 2.5 g)
Gruppe B
(n=202):
Akuteingriff*
(*innerhalb von 8h)
0–15 Minuten 90 Tage Follow-Up
0–24 Stunden
Blut Proben
Ankunft Spital Vor der 1. Dosis Vor der 2. Dosis ~20 min 1 h 2 h 4 h 12 h 24 h 30 d 90 d
Primärer Endpunkt Verschiedene
Reversierung der Dabigatran Wirkung Sicherheitsendpunkte
Pollack CV et al. Thromb Haemost 2015; 114, 198-205RE-VERSE AD™: Patienten-Charakteristika
Pollack CV et al NEJM 2015, 373: 511-20; Pollack CV et al NEJM 2017, 377: 431-41RE-VERSE AD™: Indikation zur Gabe
von Idarucizumab
Pollack CV et al NEJM 2015, 373: 511-20; Pollack CV et al NEJM 2017, 377: 431-41RE-VERSE AD™: Idarucizumab vs. Dabigatran Spiegel
Pollack CV et al NEJM 2015, 373: 511-20; Pollack CV et al NEJM 2017, 377: 431-41RE-VERSE AD™: Wirkungen /
Nebenwirkungen
Gruppe A: Mediane Zeit bis Blutungsstopp: 2.5h
Gruppe B: Mediane Zeit bis OP 1.6h
93.6 % der OPs mit unauffälliger Blutungsneigung, 5.1% Milde
Blutungsneigung, 1.5 % „Moderate“ Abnormal
Nebenwirkungen:
3 mögliche Allergische Reaktionen (Erythem, Erbrechen, 1x Kollaps – Anaphylaxie?)RE-VERSE AD™: Thromboembolischer
Ereignisse / Mortalität
Bis zum Tag 90:
Gruppe A:
Thromboembolische
Ereignisse 6.3%;
Mortalität 18.8%
Gruppe B: Thrombo-
embolische Ereignisse
7.4%%; Mortalität
18.9%
Pollack CV et al NEJM 2015, 373: 511-20; Pollack CV et al NEJM 2017, 377: 431-41Antidot FXa-Antagonisten: Andexanet alfa
(Annexa®)
• PRT064445 – katalytisch inaktives rXa/fehlende Gla-Domäne 39kD; Portola
Pharmaceuticals
• Hohe (subnanomolare) Affinität zu Xa-Antagonisten = Ki ~ pdFXa – FXa-Antagonist
Lu G et et al. Nature Med 2013, 19: 446-51Andexanet: Reversal von Faktor Xa Antagonisten
Siegel DM et al NEJM 2015Andexanet: ANNEXA-4 Trial
Interims-Analyse –
multicenter, prospective, open-label, single-
group study
• 67 Patienten (Date Completed 17.6.16)
• 20 Zentren USA,1 UK, 1 Kanada
• “Acute major bleeding” innerhalb 18h
nach Einnahme von Xa Inhibitor
Conolly SJ et al N Engl J Med. 2016 Sep 22;375(12):1131-41.Andexanet: ANNEXA-4 Trial
Andexanet - Rivaroxaban
800mg Bolus-Injektion - 800mg Bolus + 120 Minuten
Infusion 8mg/min
Andexanet - Apixaban
400mg Bolus-Injektion - 400mg Bolus + 120 Minuten Infusion
4mg/min
Conolly SJ et al N Engl J Med. 2016 Sep 22;375(12):1131-41.Outcome: ANNEXA-4 Trial
Conolly SJ et al N Engl J Med. 2016 Sep 22;375(12):1131-41.Ciraparantag - PER977, aripazine
Phase of development: 1/21
Dab PT Structure: small, synthetic, water-soluble,
cationic molecule1
Mechanism of action:
– Competitive binding to target anticoagulant
FXa-I through hydrogen bonding and charge-charge
interactions, restoring activity of blocked
coagulation factors1
Ciraparantag Preclinical and PK/PD data:
– Complete reversal of anti-FXa activity of
Xa Va
rivaroxaban and apixaban in human plasma2
– Decreased rivaroxaban-, apixaban- and
dabigatran-induced bleeding by >90% in animal
Competitively binds to FXa and FIIa inhibitors via models2
hydrogen bond formation
– Absence of binding to plasma proteins including
albumin3
– No interaction with several cardiovascular,
antiepileptic and anesthetic drugs3
– No evidence of procoagulant activity2,3
Enriquez A et al. Europace. 2015. [Epub ahead of print]; 2. Laulicht B et al. Circulation.
2012;126:11395. [Abstract]; 3. Ansell JE et al. N Engl J Med. 2014;371:2141-2142.Ciraparantag: Phase 1 and 2 Trials
• Five trials: 2 completed with no published results,1a 2 currently ongoing (including an
edoxaban-related trial),1b and 1 with published findings on edoxaban reversal2
In healthy volunteers treated
with edoxaban 60 mg2
– Clotting time decreased to
within 10% of baseline levels
after a single dose of
ciraparantag (100-300 mg)
in ≤10 minutes and was
maintained for 24 hours
– Potentially related AEs of
ciraparantag administration
were transient mild perioral
and facial flushing and
dysgeusia, moderate
headache5
aPhase 1 PK study and Phase 1/2 study on enoxaparin reversal.
bPhase 1/2 study on heparin reversal and Phase 1/2 study on edoxaban reversal and re-anticoagulation.
AE = adverse event; PK = pharmacokinetic.
1. www.clinicaltrials.gov; Ansell JE et al N Engl J Med. 2014 Nov 27;371(22):2141-2Gerinnungsmanagement in der Notfallmedizin • Transfusion-Management und Gerinnungsstörungen • Blutungen unter oraler AK-Therapie • Leberzirrhose und Blutungen
Erhöhtes Thromboembolie – Risiko bei
Patienten mit Leberzirrhose
Eleven studies (15 data-sets) showed a
significantly increased VTE risk in 695,012 cirrhotic patients as compared
with 1,494,660 non-cirrhotic controls (OR: 1.703; 95 %CI: 1.333,
2.175; PSpontane INR Erhöhung bei Leberzirrhose
kein Schutz vor VTE
Retrospektive Analyse – University of Missouri–Columbia
Patienten mit ICD Code: CLD and cirrhosis
Jan. 1, 2000 – Jan. 31, 2007.
Dabbagh O et al. Chest 2010, 137,5, 1145–1149Spontane INR Erhöhung bei Leberzirrhose
kein Schutz vor VTE
Dabbagh O et al. Chest 2010, 137,5, 1145–1149Neues Gleichgewicht der Gerinnung bei
chronischen Lebererkrankungen
Tripodi A et al. NEJM. 2011, 365: 147-156
Tripodi A et al. Am J Gastroenterol. 2017 Feb;112(2):274-281.Ursachen für Blutungen bei Patienten mit
Leberzirrhose
Ambrosino P et al. Thromb Haemost 2017; 117: 139–148Vorgehen bei Blutungen und Leberzirrhose
• Variceal bleeding is a common and potentially life-
threatening complication of liver disease, occurring in 25
to 35 percent of individuals with cirrhosis, and
accounting for the majority of cirrhotic bleeding
episodes
• The major cause of variceal bleeding is thought to be
local vascular deformations and hemodynamic changes
• Hemostatic mechanisms appear to play only a transient
role
Thus, the most important interventions for prevention and
treatment of bleeding involve reducing portal pressure
and ligating bleeding lesions.
The use of prohemostatic agents may be appropriate as rescue agents. However, potential
benefits must be weighed against risks such as increased portal pressure with plasma
transfusions and increased thrombotic risk with coagulation factor concentrates. We are
unaware of studies that have adequately evaluated rFVIIa or PCC in uncontrollable
hemorrhage, although they have occasionally been used to try to temporize an unstable
situation.
UptoDate 2018Vorgehen bei Blutungen und Leberzirrhose
Stravitz RT Hepatol Int. 2018 Jul 31. doi: 10.1007/s12072-018-9886-6.• Transfusion-Management und
Gerinnungsstörungen
• Cave: Nebenwirkungen der
Flüssigkeitssubstitution
• Blutungen unter oraler AK-Therapie
• Spezifisches Antidot
• Leberzirrhose und Blutungen
• Lokale MaßnahmenSie können auch lesen