A 73-year-old woman presented to the dermatology clinic with an 11-month history of an evolving pruritic, erythematous rash on her thighs and ...
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
A 73-year-old woman presented to the
dermatology clinic with an 11-month history of
an evolving pruritic, erythematous rash on her
thighs and buttocks. On physical examination
she was noted to have polycyclic erythematous
plaques. What is the most likely diagnosis?
Dermatomyositis
Subacute lupus erythematosus
Erythema gyratum repens
Tinea versicolor
Necrolytic migratory erythema
The patient received a clinical diagnosis of erythema gyratum repens, which is a rare
paraneoplastic rash associated with breast, lung, or esophageal cancer. She underwent
imaging and colonoscopy before being diagnosed with anal squamous cell carcinoma. The
patient was treated with topical glucocorticoids and gabapentin for pruritus. The rash
improved after initiation of chemotherapy and radiation.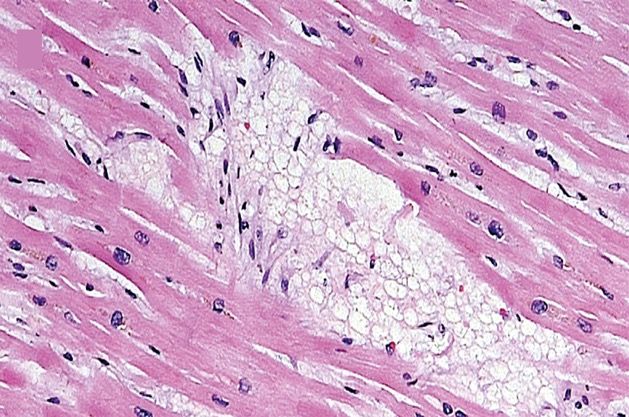
Die Dermatomyositis (DM, auch Lilakrankheit, Wagner- Unverricht-Syndrom) ist eine idiopathische Myopathie (=Muskelerkrankung) bzw. Myositis (=Muskelentzündung) mit Hautbeteiligung und gehört zu der Gruppe der Kollagenosen. Ist nur die Muskulatur betroffen, so spricht man in der Regel von einer Polymyositis (PM). Aktuelle Studien zur Pathogenese der DM und PM widersprechen sich. Da noch nicht gesichert ist, ob DM und PM die gleiche Pathogenese haben, wird im Folgenden die Dermatomyositis getrennt besprochen und auf die Polymyositis sei nur verwiesen. Die Erkrankung ist selten und kann in jedem Lebensalter auftreten. Das Häufigkeitsmaximum ist das 50. Lebensjahr, Frauen sind öfter betroffen als Männer (Gynäkotropie 2:1). Bei Kindern liegt das Altersmaximum bei vier bis zwölf Jahren. Bei Haushunden tritt die Dermatomyositis nahezu ausschließlich bei Welpen und Junghunden auf. Sie wurde von Ernst Leberecht Wagner (1821–1888) 1863 beschrieben und weiter von Heinrich Unverricht untersucht. Ungefähr 50 % der Dermatomyositiden sind mit Tumoren assoziiert. Besonders hervorzuheben sind dabei Ovarialkarzinome. Es ist deswegen nötig, bei neu aufgetretener Dermatomyositis nach Tumoren zu suchen. Allerdings ist der zeitliche Bezug zum Auftreten der Dermatomyositis zu dem des Tumors extrem variabel – die Haut- und Muskelerkrankung kann dem Tumor sowohl vorausgehen, als auch nachfolgen oder sich zeitgleich manifestieren. In manchen Fällen kann das Wiederauftreten einer Dermatomyositis nach zwischenzeitlicher Heilung von einem Tumor dessen Rezidiv, d. h. Wiederkehr, anzeigen. Die im Rahmen einer Neoplasie auftretende Dermatomyositis ist nach Entfernung der Neoplasie vollständig reversibel.
Der Lupus erythematodes (lateinisch lupus, deutsch ‚Wolf‘, und altgriechisch ἐρυθηματώδης erythēmatṓdēs aus ἐρύθημα erýthēma, deutsch ‚Röte‘, und Suffix - ώδης -ṓdēs, deutsch ‚ähnlich wie‘), auch Schmetterlingsflechte, ist eine seltene Autoimmunerkrankung. Beim Lupus erythematodes ist das körpereigene Immunsystem fehlreguliert: Es richtet sich hierbei gegen gesunde körpereigene Zellen. Dadurch werden Organe und Organsysteme, z. B. die Haut, geschädigt. Es gibt unterschiedliche Formen des Lupus erythematodes: Die verschiedenen Formen des kutanen Lupus erythematodes (CLE) befallen üblicherweise nur die Haut. Der systemische Lupus erythematodes (SLE) kann alle Organe befallen. Er gehört zur Gruppe der Kollagenosen. Als Kollagenose gehört der systemische Lupus erythematodes zu den Erkrankungen des rheumatischen Formenkreises. Der neonatale Lupus erythematodes bei Neugeborenen ist eine Folge der mütterlichen Lupus-erythematodes- Erkrankung. Der Name Lupus wurde von dem lombardischen Chirurgen Roger Frugardi (um 1140–1195) eingeführt, ist aber auch schon im 10. Jahrhundert belegt. Der Begriff Lupus leitet sich vom lateinischen Namen für den Wolf ab. Früher verglich man die Narben, die nach dem Abheilen der Hautschäden verbleiben, mit Narben von Wolfsbissen.
Das Erythema gyratum repens gehört zu den figurierten Erythemen. Es tritt paraneoplastisch auf, vor allem bei Bronchial- und Mammakarzinomen sowie bei malignen Tumoren des weiblichen Genitales, des Ösophagus oder des Magens. Die Hautveränderungen können dem Tumorleiden 4-8 Monate vorausgehen. Das Eyrthema gyratum repens tritt vor allem bei Erwachsenen zwischen dem 40. und 60. Lebensjahr auf. Das Erythema gyratum repens präsentiert sich als urtikariell eleviertes, rasch wanderndes (in Stunden), 1- 2 cm breites, streifiges Erythem. Die Effloreszenzen sind anulär, girlandenartig oder spiralig ineinander geschwungen und erinnern an Holzmaserungen. Im Randbereich weisen sie eine halskrausenartige Schuppung auf. Das Erythema gyratum repens tritt bevorzugt im Bereich des Körperstamms und an den proximalen Extremitätenabschnitten auf. Die Ursache für das Erythema gyratum repens ist unklar. Vermutet wird eine immunologische Reaktion auf Antigene wie z.B. Verbindungen, die von Tumoren produziert werden. Die Hautveränderung kann schon mehrere Monate auftreten, bevor andere Symptome einer Tumorerkrankung auffallen. Der Primärtumor ist meist ein Karzinom (Mamma-, Magen-, Lungen-, Prostata-, Ösophagus-, Genitalkarzinome), seltener werden andere Neoplasien wie ein Melanom oder ein Plasmozytom gefunden.
Pityriasis versicolor (Kleienpilzflechte, auch: Kleieflechte) ist eine häufig vorkommende Pilzinfektion der obersten Hautschicht (Epidermis). Der Erreger dieser Hautmykose ist Malassezia furfur (früher u. a.: Pityrosporum orbiculare bzw. Pityrosporum ovale). Der Pilz bleibt als Hefe im einzelligen Stadium, bildet also keinen Fruchtkörper und kein Mycel aus. Es gibt von Land zu Land unterschiedliche Prävalenzen für die versch. Malassezia-Spezies. Die Erkrankung ist harmlos und nicht ansteckend. Malassezia-Hefen gehören bei annähernd 100 % der Bevölkerung zur normalen Hautflora. Die Gründe, warum sie bei manchen Menschen pathogen (krankhaft) werden, sind nicht ganz geklärt. Es wird jedoch beobachtet, dass die Hautmykose verstärkt in den Sommermonaten und bei Menschen mit Neigung zu starkem Schwitzen auftritt. Auch eine Verbindung mit hoher Schilddrüsenfunktion wird angenommen. Es bildet sich ein Pilzrasen, der zum einen physikalisch Licht blockiert, zum anderen toxisch die Melaninproduktion hemmt. Bei Sonnenkontakt bräunt die befallene Haut weit weniger als die umgebenden Partien, wodurch weiße Flecken (Maculae) entstehen. Diese können linsengroß sein oder sich zu einer landkartenartigen Marmorierung der Haut ausweiten. Die Diagnose wird vom Dermatologen meist als Blickdiagnose gestellt und kann durch das Abkratzen von Hautschuppen und die Begutachtung unter dem Mikroskop bestätigt werden. Die Pilzzellen sind als traubenförmige Kugelhäufchen zu erkennen.
Erythema necrolyticum migrans Bei Glukagon-produzierenden Tumoren (Glukagonom) auftretendes paraneoplastisches Syndrom der Haut mit erythematösen bogenförmigen Arealen mit Krusten- bildung und langsamer Ausbreitungstendenz. Weitere mögliche Erscheinungen sind Cheilitis, Nageldystrophi- en, Stomatitis, Diarrhö, Thromboseneigung, Diabetes mellitus, Hyperglukagonämie und B-Symptomatik. Diagnostiziert wird klinisch, laborchemisch und his- tologisch. Das Glukagonom wird gesucht und saniert. Bizarr geformte zirzinäre Erytheme mit zentrifugaler Ausbreitung und Pustelbildung. Erythema necroticans migrans; Fünfte obligate kutane Paraneoplasie; Impetigo circinata; Necrolytic migratory erythema; Nekrolytisches migratorisches Erythem; Paraneoplasie fünfte obligate kutane; Staphylodermia superficialis circinata. Postuliert wird durch das erhöhte Glucagon eine katabole Stoffwechsellage mit einem Mangel an Zink und verschiedenen Aminosäuren. Für diese These spricht das rasche Ansprechen der Hautverändeurngen auf Aminosäure-Substitutionen. Bemerkenswert ist, dass sich das klinische und histologische Bild nicht von Hautverändeurngen bei Zinkmangelsyndrom oder Biotin-Mangel unterscheidet.
Die Sichelzellkrankheit oder Sichelzellenanämie (medizinisch Drepanozytose), auch Sichelzellanämie ist eine erbliche Erkrankung der roten Blutkörperchen (Erythrozyten). Sie gehört zur Gruppe der Hämoglobinopathien (Störungen des Hämoglobins) und führt zu einer korpuskulärenhämolytischen Anämie. Bei den Betroffenen liegt eine Mutation der β-Kette des Hämoglobins vor. Es können entweder alle β-Ketten betroffen sein (schwere, homozygote Form) oder nur ein Teil (mildere, heterozygote Form). Die Krankheit tritt vor allem bei dunkelhäutigen Personen aus Subsahara-Afrika und deren Nachfahren, aber auch in Teilen des Mittelmeerraums und des Nahen Ostens bis Indien auf und wurde durch Migration global verbreitet. Sie ist nach wie vor in den Entwicklungsländern mit einer hohen Mortalität verbunden. Die Krankheit wurde 1910 von James Herrick und Ernest Lyons bei einem Patienten aus der Karibik beschrieben und die Bezeichnung Sichelzellenanämie wurde zuerst von Vernon Mason 1922 benutzt. Die Betroffenen bilden ein abnormes Hämoglobin (Sichelzell-Hämoglobin, HbS), das bei Sauerstoffmangel zur Bildung von Fibrillen neigt. Dabei verformen sich die roten Blutzellen durch die enthaltenen Fasern zu sichelförmigen Gebilden, verklumpen miteinander und verstopfen kleine Blutgefäße, wodurch eine Entzündungentsteht. Durch die Verklumpung und Gefäßverstopfung kann es bei der homozygoten Form zu anfallsartigen schmerzhaften, z. T. lebensbedrohlichen Durchblutungsstörungen (Sichelzellkrisen) kommen, die unter anderem zu venösen Thrombosen führen können. Aufgrund einer Punktmutation auf Chromosom 11 ist bei der Sichelzellenanämie an der Position sechs der β- Globin-Protein-Untereinheit des Hämoglobins die Aminosäure Glutaminsäure durch Valin ersetzt. Die Bezeichnung dieser Variante in offizieller genetischer Nomenklatur lautet HBB-p.E6V. Die betroffenen Erythrozyten verformen sich bei abnehmendem Sauerstoffpartialdruck sichelförmig, verfangen sich leicht in den Kapillaren und lysieren überdies sehr schnell. Durch die Hämolyse werden Hämoglobin, Arginase und freie Sauerstoffradikale freigesetzt. Freies Hämoglobin bindet Stickstoffmonoxid etwa 1000-mal stärker als intrazelluläres und Arginase verwandelt Stickstoffmonoxid zu Nitrit und Nitrat. Stickstoffmonoxid ist der wichtigste Vasodilatator, und die Konzentrationsabnahme führt zur Gefäßverengung und somit zu Durchblutungsstörungen.
Hydroxycarbamid (INN), auch Hydroxyharnstoff oder Hydroxyurea, ist ein Zytostatikum, das zur Behandlung insbesondere von malignen Bluterkrankungen (Leukämien, Myeloproliferative Neoplasien) eingesetzt wird. Es ist auch für die Behandlung der Sichelzellanämie zugelassen. Im Rahmen von experimentellen Studien wurde es für die antiretrovirale Behandlung bei HIV-Infektion getestet. Die Wirkung der Substanz beruht auf der Hemmung des Enzyms Ribonukleotidreduktase, welche die Ribose zur Desoxyribose reduziert. Diese verläuft über einen radikalischen Mechanismus, der die Bildung eines Tyrosinradikals im aktiven Zentrum des Enzyms erfordert. Das stabile Tyrosinradikal entsteht durch ein nahegelegenes Eisenzentrum, welches aus zwei Fe3+ besteht. Hydroxyharnstoff komplexiert das Eisen und bewirkt die Reduktion des Eisens zum Fe2+, wodurch die DNA-Synthesekapazität der jeweiligen Zelle deutlich eingeschränkt wird. Durch die europäische Arzneimittelbehörde EMA wurde die Substanz auch zur Behandlung der Sichelzellanämie zugelassen. Hydroxycarbamid erhöht die fetale Hämoglobin-Synthese (Hb F) im Blut. Ein prozentual erhöhter Anteil von Hb F im Blut wirkt protektiv gegenüber der Polymerisation von Sichelzellen. In mehreren klinischen Studien konnte die Wirksamkeit im Rahmen vaso-okklusiver Krisen gezeigt werden.
Modification of the Pathophysiology of Sickle Cell Disease by Hydroxyurea. All the manifestations of sickle cell disease depend, directly or indirectly, on sickling, which in turn is produced, as red cells deliver oxygen to tissues, by the polymerization of deoxyhemoglobin S. Sickled red cells may become stuck in capillaries and, by jamming small vessels, may cause vaso-occlusion and consequent pain crises. Sickled red cells may undergo lysis within the bloodstream (intravascular hemolysis), whereby hemoglobin released in the plasma will bind nitric oxide (NO), resulting in vasoconstriction that will further favor vaso-occlusion. Sickled red cells will also be phagocytosed by macrophages (extravascular hemolysis); together with intravascular hemolysis, this causes anemia, often severe. Sickled red cells will also adhere to the endothelium, causing a chronic inflammatory state that is associated with neutrophil leukocytosis. The main action of hydroxyurea is to cause an increase in the intracellular concentration of fetal hemoglobin (HbF), which interferes with the deoxyhemoglobin S polymer formation, reducing the rate of sickling. Through this mechanism, hydroxyurea affects the very source of all the pathologic features of sickle cell disease. In addition, hydroxyurea lowers the neutrophil count, thus reducing the chronic inflammatory state.
Hydroxyurea for Children with Sickle Cell Anemia in Sub-Saharan Africa Hydroxyurea is an effective treatment for sickle cell anemia, but few studies have been conducted in sub- Saharan Africa, where the burden is greatest. Coexisting conditions such as malnutrition and malaria may affect the feasibility, safety, and benefits of hydroxyurea in low-resource settings. We enrolled children 1 to 10 years of age with sickle cell anemia in four sub-Saharan countries. Children received hydroxyurea at a dose of 15 to 20 mg per kilogram of body weight per day for 6 months, followed by dose escalation. The end points assessed feasibility (enrollment, retention, and adherence), safety (dose levels, toxic effects, and malaria), and benefits (laboratory variables, sickle cell–related events, transfusions, and survival). Retention of Participants in the Trial. The shaded area represents the 95% confidence interval for death or withdrawal from the trial. The inset shows the same data on an enlarged y axis.
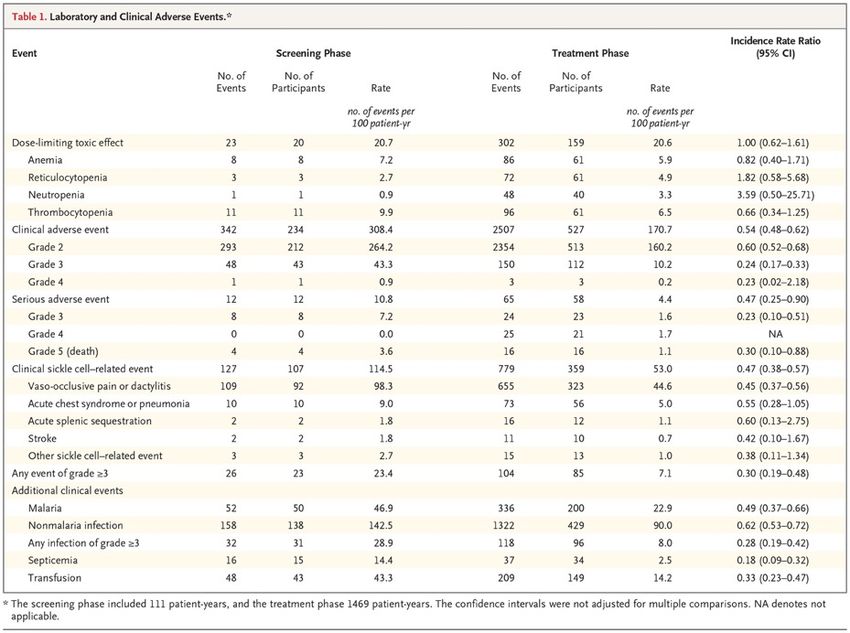
During hydroxyurea treatment, the white-cell count, absolute neutrophil count, and absolute reticulocyte count significantly decreased, reflecting the intended mild bone marrow suppression, and these effects were sustained over time. The overall rate of sickle cell–related events was significantly reduced (114.5 vs. 53.0 events per 100 patient-years; incidence rate ratio, 0.47; 95% CI, 0.38 to 0.57), and the rates of vaso- occlusive pain and the acute chest syndrome were both reduced. The rates of infection also declined, including rates of nonmalaria infection (142.5 vs. 90.0 events per 100 patient-years; incidence rate ratio, 0.62; 95% CI, 0.53 to 0.72) and severe infection of grade 3 or higher (28.9 vs. 8.0 events per 100 patient- years; incidence rate ratio, 0.28; 95% CI, 0.19 to 0.42). Analyses of additional key clinical events revealed significant reductions during hydroxyurea treatment in the rate of malaria infections (46.9 vs. 22.9 events per 100 patient-years; incidence rate ratio, 0.49; 95% CI, 0.37 to 0.66), blood transfusion (43.3 vs. 14.2 events per 100 patient-years; incidence rate ratio, 0.33; 95% CI, 0.23 to 0.47), and death (3.6 vs. 1.1 events per 100 patient-years.
Adverse Events before and during Hydroxyurea Treatment. Error bars indicate 68% confidence intervals, which correspond to approximately 1 standard error. In this trial involving children with sickle cell anemia living in sub-Saharan Africa, we found that hydroxyurea treatment was feasible, reasonably safe, and had both laboratory and clinical benefits. Specifically, as compared with pretreatment rates, the rates of clinical events, including vaso- occlusive pain, infection, malaria, transfusion, and death, declined after 1 year of hydroxyurea treatment. In conclusion, our results show that daily hydroxyurea treatment was feasible and safe for children with sickle cell anemia in sub-Saharan Africa. Moreover, hydroxyurea treatment reduced the rates of painful events, infection, malaria, transfusion, and death. Despite the recognition that 50 to 90% of affected children in Africa die before the age of 5 years, sickle cell anemia remains a neglected disease for which safe and effective treatment options are needed.
The choice of the graft conduit for coronary artery bypass grafting (CABG) has significant implications both in the short- and long-term. The patency of a coronary conduit is closely associated with an uneventful postoperative course, better long-term patient survival and superior freedom from re- intervention. The internal mammary artery is regarded as the primary conduit for CABG patients, given its association with long-term patency and survival. However, long saphenous vein (LSV) continues to be utilized universally as patients presenting for CABG often have multiple coronary territories requiring revascularization. Traditionally, the LSV has been harvested by creating incisions from the ankle up to the groin termed open vein harvesting (OVH). These concerns regarding wound morbidity and patient satisfaction led to the emergence of endoscopic vein harvesting (EVH). Published experience comparing OVH with EVH suggests decreased wound related complications, improved patient satisfaction, shorter hospital stay, and reduced postoperative pain at the harvest site following EVH. Despite these reported advantages concerns regarding risk of injury at the time of harvest with its potential detrimental effect on vein graft patency and clinical outcomes have prevented universal adoption of EVH.
Randomized Trial of Endoscopic or Open Vein-Graft Harvesting for Coronary- Artery Bypass The saphenous-vein graft is the most common conduit for coronary- artery bypass grafting (CABG). The influence of the vein-graft harvesting technique on long-term clinical outcomes has not been well characterized. We randomly assigned patients undergoing CABG at 16 Veterans Affairs cardiac surgery centers to either open or endoscopic vein-graft harvesting. The primary outcome was a composite of major adverse cardiac events, including death from any cause, nonfatal myocardial infarction, and repeat revascularization. Leg-wound complications were also evaluated.
Leg-wound infections occurred in 18 patients (3.1%) in the open-harvest group and in 8 patients (1.4%) in the endoscopic-harvest group (absolute difference, 1.7 percentage points; relative risk, 2.26; 95% CI, 0.99 to 5.15). Incisional leg pain had little or no effect on functioning at 6 weeks after surgery in 62.2% of the patients in the open-harvest group, as compared with 79.1% of those in the endoscopic-harvest group (relative risk, 0.79; 95% CI, 0.73 to 0.85). Antibiotics were administered at follow-up to 14.4% of the patients in the open- harvest group and in 4.6% of the patients in the endoscopic-harvest group (relative risk, 3.15; 95% CI, 2.06 to 4.82).
In this trial, in which vein-graft harvesting for CABG was performed by operators with documented experience, we did not find any significant difference between open and endoscopic vein-graft harvesting in the rate of major adverse cardiac events over a median follow-up of 2.78 years. We found a trend toward lower rates of major adverse cardiac events in association with the endoscopic technique when recurrent events were compared between the two treatment groups, although longer-term follow-up will be necessary to determine whether this finding is persistent. Endoscopic harvesting resulted in better harvest-site healing than did the open approach, a finding consistent with previous observations. In conclusion, our trial did not show a significant difference between endoscopic and open vein-graft harvesting in the rate of major adverse cardiac events among patients undergoing CABG surgery during a follow-up period with a median duration of 2.78 years. The rate of wound complications was lower in the endoscopic- harvest group than in the open-harvest group. Further studies are needed to establish standards for harvester expertise to ensure the safety of patients and effectiveness of the procedure.
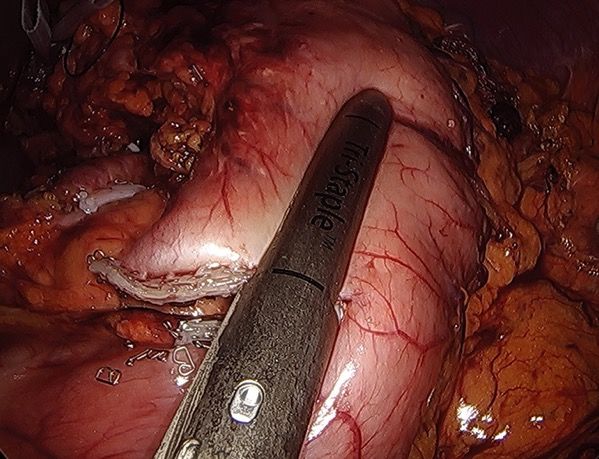
Hybrid and total minimally invasive esophagectomy: how I do it Esophagectomy is a major surgical procedure associated with a significant risk of morbidity and mortality. Minimally invasive esophagectomy is becoming the preferred approach because of the potential to limit surgical trauma, reduce respiratory complications, and promote earlier functional recovery. Various hybrid and total minimally invasive surgical techniques have been introduced in clinical practice over the past 20 years, and minimally invasive esophagectomy has been shown equivalent to open surgery concerning the short-term outcomes. Implementation of a minimally invasive esophagectomy program is technically demanding and requires a significant learning curve and the infrastructure of a dedicated multidisciplinary center where optimal staging, individualized therapy, and perioperative care can be provided to the patient. Both hybrid and total minimally invasive techniques of esophagectomy have proven safe and effective in expert centers. The choice of the surgical approach should be driven by preoperative staging, tumor site and histology, comorbidity, patient’s anatomy and physiological status, and surgeon’s experience.
Preoperative staging and tumor characteristics influence the choice of the surgical strategy, i.e., a 2-stage or a 3-stage procedure. In some circumstances, starting with laparoscopy or thoracoscopy may be useful to provide the ultimate staging. Initial laparoscopic approach for gastric conduit preparation, as part of a hybrid or total minimally invasive Ivor Lewis operation, is feasible in the majority of patients with esophageal adenocarcinoma.
Laparoscopic division of the left gastric artery between Hemolock clips.
Laparoscopic gastric tubulisation.
Trans-thoracic esophago-gastric anastomosis. (A) Circular stapler introduced into the gastric tube through a gastrotomy at the apex of the lesser curve; (B) the anastomosis as viewed through the gastrotomy site.
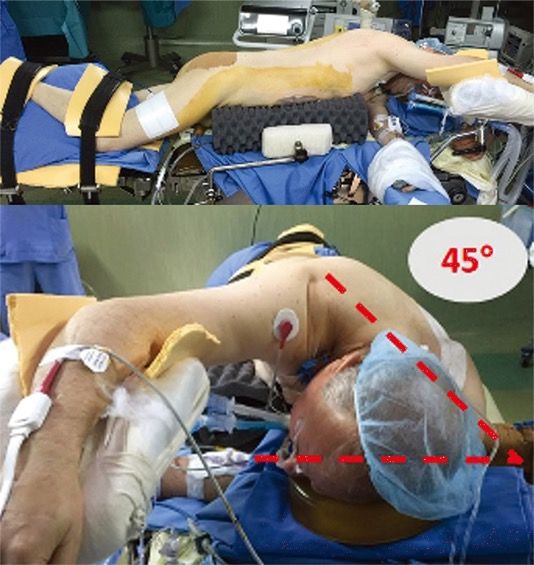
Semi-prone patient positioning with a typical 45° angle.
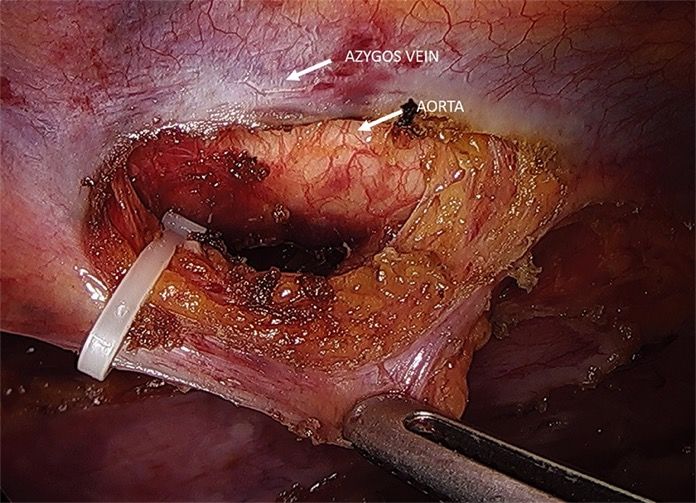
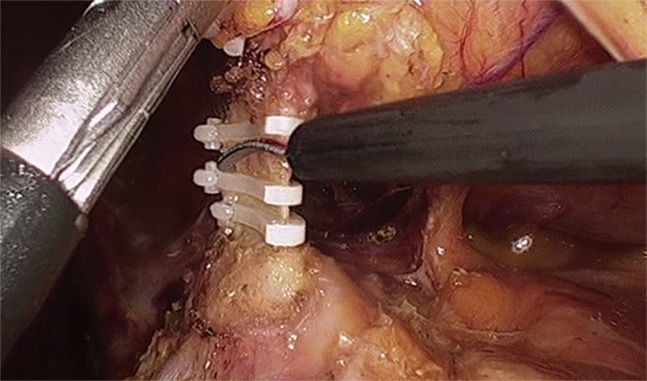
The thoracic duct is secured with Hemolock clip at the level of the diaphragm.
Hybrid Minimally Invasive Esophagectomy for Esophageal Cancer Postoperative complications, especially pulmonary complications, affect more than half the patients who undergo open esophagectomy for esophageal cancer. Whether hybrid minimally invasive esophagectomy results in lower morbidity than open esophagectomy is unclear. We performed a multicenter, open-label, randomized, controlled trial involving patients 18 to 75 years of age with resectable cancer of the middle or lower third of the esophagus. Patients were randomly assigned to undergo transthoracic open esophagectomy (open procedure) or hybrid minimally invasive esophagectomy (hybrid procedure). Surgical quality assurance was implemented by the credentialing of surgeons, standardization of technique, and monitoring of performance. Hybrid surgery comprised a two-field abdominal–thoracic operation (also called an Ivor–Lewis procedure) with laparoscopic gastric mobilization and open right thoracotomy. The primary end point was intraoperative or postoperative complication of grade II or higher according to the Clavien–Dindo classification (indicating major complication leading to intervention) within 30 days. Analyses were done according to the intention-to-treat principle.
The percentage of patients receiving neoadjuvant therapy was similarly high in the two groups (75% in the hybrid-procedure group and 72% in the open-procedure group). A total of 3 patients (3%) who had been assigned to the hybrid-procedure group underwent intraoperative conversion to the open procedure: 1 underwent laparotomy without resection because of advanced disease, 1 underwent intraoperative conversion to the open procedure because of subcutaneous emphysema, and 1 underwent intraoperative conversion to the open procedure, as decided by the surgeon on the basis of intraoperative physiological stress of the patient. According to the intention-to-treat principle, these patients were included in the hybrid-procedure group.
After adjustment for age, sex, American Society of Anesthesiologists risk score, neoadjuvant therapy use, tumor location, histologic subtype, resection-margin status, pathological tumor and node stages, and trial center, we found that minimally invasive surgery was associated with a 77% lower risk of major intraoperative and postoperative complications within 30 days than open surgery (adjusted odds ratio, 0.23; 95% CI, 0.12 to 0.44; P
In this multicenter, randomized, controlled trial, we found that hybrid minimally invasive esophagectomy was associated with a 77% lower risk of major intraoperative and postoperative complications than open esophagectomy. Furthermore, minimally invasive surgery was associated with a 50% lower risk of major pulmonary complications than open surgery. Overall survival and disease-free survival were at least as good with minimally invasive surgery as with the open procedure. In parallel to previous findings regarding colorectal resection and gastrectomy, we found that a minimally invasive approach to the abdominal phase of an Ivor–Lewis two-field abdominal– thoracic esophagectomy was associated with substantially lower major morbidity, specifically pulmonary morbidity. In conclusion, this multicenter, randomized, controlled trial showed that hybrid minimally invasive esophagectomy resulted in a lower incidence of major complications (specifically, pulmonary complications) during or after esophagectomy for cancer than did open surgery. The hybrid procedure also resulted in overall survival and disease- free survival that were similar to those observed with open esophagectomy.
Das WHIM-Syndrom (kurz für Warzen-Hypogammaglobulinämie- Immundefizienz-Myelokathexis-Syndrom) ist eine vererbbare, seltene Immunschwächekrankheit. Charakteristisch für das WHIM-Syndrom ist eine Immunschwäche, die sich in wiederkehrenden bakteriellen und viralen Infektionen äußert. Davon sind insbesondere die Atemwege mit Nasennebenhöhlenentzündungen, Mandelentzündungen und Lungenentzündungen betroffen. Die Patienten sind anfällig für Infektionen mit humanen Papillomaviren, die sich in zahlreichen Warzen, insbesondere im Hand- und Fußbereich, äußern. WHIM- Syndrom-Patienten haben darüber hinaus ein erhöhtes Risiko, an viral-bedingten Krebsarten, wie beispielsweise demCervixkarzinom, zu erkranken. Im Blutserum der Patienten können erniedrigte IgG-Konzentrationen gemessen werden (Hypogammaglobulinämie). Histologisch erscheint das Knochenmark der WHIM-Patienten voller T-Vorläuferzellen. Dem gegenüber kann eine Neutropenie beobachtet werden, die auf eine gestörte Auswanderung und somit Zurückhaltung neutrophiler Granulozyten aus dem Knochenmark zurückgeführt werden kann (Myelokathexis). Das WHIM-Syndrom ist eine autosomal-dominant vererbte Krankheit. Als häufigste Ursache, die bei 92 % der betroffenen Patienten gefunden wurde, werden Mutationen eines Gens auf dem Genlocus 2q21, das den Chemokinrezeptor CXCR4 codiert, angesehen. Diese Mutationen im intrazellulären Teil des membranständigen Rezeptors für das Zytokin CXCL12 (SDF-1) führen zu einem verkürzten Rezeptorprotein, dem die Fähigkeit der Internalisierung nach Aktivierung fehlt. Somit sind Mechanismen der negativen Selbstregulation unterbrochen und der Rezeptor kann dauerstimuliert werden.
Plerixafor for the Treatment of WHIM Syndrome
WHIM syndrome (warts, hypogammaglobulinemia, infections, and myelokathexis), a primary immunodeficiency
disorder involving panleukopenia, is caused by autosomal dominant gain-of-function mutations in CXC
chemokine receptor 4 (CXCR4). Myelokathexis is neutropenia caused by neutrophil retention in bone marrow.
Patients with WHIM syndrome are often treated with granulocyte colony-stimulating factor (G-CSF), which can
increase neutrophil counts but does not affect cytopenias other than neutropenia. In this investigator-initiated,
open-label study, three severely affected patients with WHIM syndrome who could not receive G-CSF were
treated with low-dose plerixafor, a CXCR4 antagonist, for 19 to 52 months. Myelofibrosis, panleukopenia,
anemia, and thrombocytopenia were ameliorated, the wart burden and frequency of infection declined, human
papillomavirus–associated oropharyngeal squamous-cell carcinoma stabilized, and quality of life improved
markedly. Adverse events were mainly infections attributable to the underlying immunodeficiency. One patient
died from complications of elective reconstructive surgery.
The periods of treatment with granulocyte colony-stimulating factor
(G-CSF) and plerixafor are demarcated by the red and blue bars at
the top of each corresponding column of graphs. The dotted
portion of the red line for Patient 1 denotes the time when high-
dose G-CSF treatment (300 μg subcutaneously every day) was
interrupted owing to severe thrombocytopenia and the drug was
given at a reduced dose (150 μg subcutaneously every other day)
only during episodes of cellulitis. Horizontal dashed black lines in
each graph designate the upper and lower limits of the normal
range for each variable, as determined by the National Institutes of
Health (NIH) Clinical Center Clinical Hematology Laboratory.
Baseline values were assessed when neither drug was being taken
(solid circles). All values for Patients 1 and 2 at baseline and during
plerixafor treatment were determined at the NIH. Peak refers to
values obtained approximately 3 hours after plerixafor
administration, the time of the peak white-cell count, as defined
previously. Trough refers to values obtained approximately 12
hours after a dose of plerixafor was administered. Most white-cell
values for Patient 3 were determined at trough by the local provider
in Germany owing to travel limitations; exceptions are designated
by the peak and trough symbols in the figure key, and these values
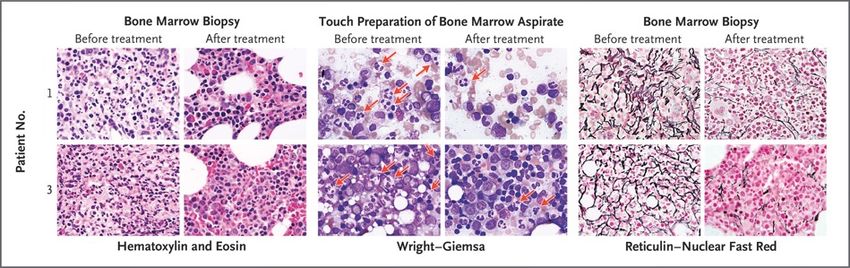
were determined at the NIH.Amelioration of Myelokathexis and Myelofibrosis during Long-Term, Low-Dose Plerixafor Treatment. Core bone marrow–biopsy samples were obtained from Patients 1 and 3 approximately 3 days before starting plerixafor (before treatment) and 24 and 52 months after starting plerixafor (after treatment) for Patients 1 and 3, respectively. Pretreatment hematoxylin and eosin–stained biopsy samples from both patients show markedly hypercellular marrow with granulocytic hyperplasia, right-shifted myelopoiesis, an elevated myeloid-to-erythroid ratio of approximately 5:1, and abundant neutrophils consistent with myelokathexis. This pattern was found in approximately 90% of the pretreatment marrow but in only 40 to 50% of the post-treatment marrow. The post- treatment images depict areas of normocellular marrow with normal myelopoiesis and a normal myeloid-to- erythroid ratio of 2:1. The pretreatment touch preparations of bone marrow aspirate (Wright–Giemsa stain) show frequent atypical neutrophils with pyknotic nuclear segments connected by thin, wispy strands of chromatin that are characteristic of myelokathexis (red arrows). These neutrophils can still be seen in the post- treatment samples but are less frequent. Both patients had severe myelofibrosis as defined by pretreatment dense reticulin staining of bone marrow; myelofibrosis was ameliorated after plerixafor treatment. All images are at 1000× magnification.
Amelioration of Skin Pathologic Conditions during Long-Term, Low-Dose Plerixafor Treatment. Panel A shows the left medial lower leg, left foot, and right medial lower leg of Patient 1 both before starting plerixafor and after 36, 36, and 28 months of plerixafor therapy for the left, middle, and right post-treatment images, respectively. The fingers of Patient 2 are shown before plerixafor was started and after 9 months of treatment, and the hand of Patient 3 is shown before plerixafor was started and after 32 months of treatment. Patient 1 had chronic eczematoid dermatitis associated with recurrent cellulitis for 6 years. The left and middle post-treatment images of this patient show resolution of inflammation, with residual areas of hyperpigmentation probably representing uncleared hemosiderin; recurrent cellulitis ceased. The right pretreatment image of this patient shows a chronic inflammatory mass centered at a site of recurrent cellulitis and saphenous-vein insufficiency that was removed surgically 6 months after plerixafor was started. The surgical wound (16×10×2 cm) healed completely (right post-treatment image). Patients 2 and 3 had a reduced cutaneous wart burden after plerixafor therapy. Both patients also received topical imiquimod, and Patient 2 received human papillomavirus (HPV) vaccination during treatment. Panel B shows clearance of 17 HPVs and Trichodysplasia spinulosa polyomavirus in Patient 1 after 18 months of plerixafor therapy. The relative abundance of each of the viruses detected is conveyed by the arc length on the donut plot. The number in the center is the number of different HPV types plus polyomavirus species detected.
We describe the CXCR4 antagonist plerixafor as a mechanism-based therapy for three patients with WHIM syndrome who could not receive G-CSF. There was a reduction in the frequency of infection in all three patients; resolution of chronic, progressive, multifocal eczematoid and follicular lesions in Patient 1, associated with clearance of TSPyV and 17 HPV types; a reduction in the wart burden in Patients 2 and 3; and a partial response of head and neck squamous-cell carcinoma in Patient 2. All three patients reported improved quality of life. Further controlled assessment of the safety and efficacy of plerixafor in patients with WHIM syndrome is a challenge because the disease is extremely rare. Nevertheless, our phase 3 trial of G-CSF versus plerixafor in WHIM syndrome is designed to permit this assessment.
Acute Infection and Myocardial Infarction
Until the early 20th century, the human life expectancy was less than 50 years, and infections were often
fatal. Only in the past century have humans, on average, lived long enough for cardiovascular disease to
develop regularly and have antimicrobial therapies made survival from infection the norm. Furthermore,
sophisticated techniques for assessing myocardial damage have evolved during the past 50 years. It is
therefore not surprising that an association between acute infections and myocardial infarction has been
appreciated only in the past few decades. We will review the evidence that acute bacterial and viral
infections are associated with an increased risk of myocardial infarction in the short, intermediate, and long
term, and we will then discuss mechanisms that might explain this association.
Temporal Pattern of Cardiovascular
Risk after the Onset of Acute Infection.
The risk of a cardiovascular event is
several times higher after the onset of
respiratory infection than in the
absence of infection. The risk of a
cardiovascular event is proportional to
the severity of the infection. The risk
returns to baseline over a period of
weeks after an upper respiratory tract
infection. However, the time required
for the risk to return to baseline is
prolonged after a severe infection,
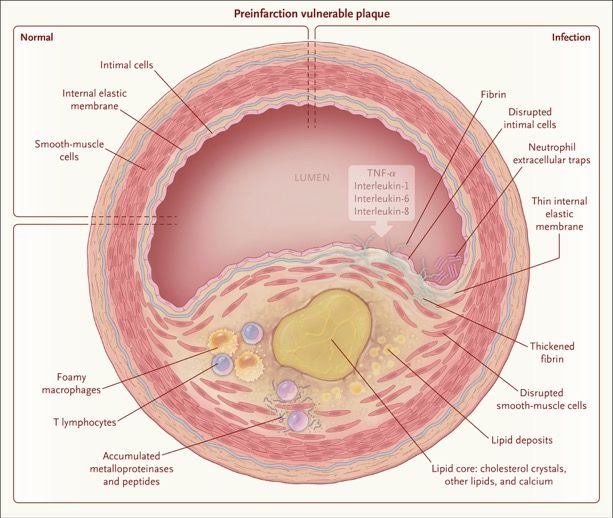
such as pneumonia.Features Present at the Time of Cardiac Involvement in Acute Infection. Shown is a vulnerable plaque (thin-cap fibroatheroma) during early infection before the development of myocardial infarction. Lipids have already accumulated in the wall of the coronary artery, with thinning of the internal elastic membrane, disruption of intimal and smooth- muscle cells, and fibrin deposition. Also present are foamy macrophages, T lymphocytes, metalloproteinases, peptidases, and neutrophil extracellular traps. In the lumen are inflammatory cytokines, including tumor necrosis factor α (TNF-α) and interleukins 1, 6, and 8, that result from sepsis elsewhere in the body.
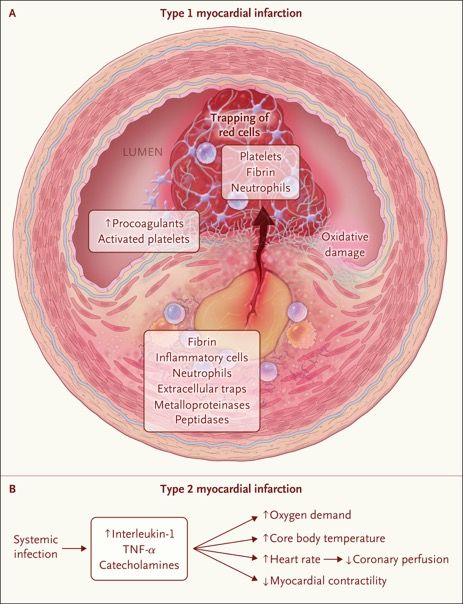
Mechanisms of Cardiac Involvement in Acute Infection. Panel A shows rupture of an atheromatous plaque, the mechanism of type 1 myocardial infarction. As a result of the inflammation that develops with infection, the thin-cap atheroma ruptures, releasing inflammatory cells and fibrin into the lumen. In the presence of circulating procoagulants and activated platelets, this release causes immediate accumulation of platelets, fibrin, and neutrophils and trapping of red cells, all of which cause acute obstruction of the coronary arteries. Panel B shows the process of demand ischemia, the mechanism of type 2 myocardial infarction. Acute infection causes the release of interleukin-1, TNF-α, and catecholamines, which increase the core body temperature, oxygen demand, and heart rate. Coronary perfusion declines because of decreased filling time. Cytokines also act to suppress cardiac output. These factors, taken together, cause a mismatch of oxygen needs and oxygen supply, resulting in demand ischemia.
Features Present after Cardiac Involvement in Acute Infection. Shown is an example of direct myocardial involvement in pneumococcal pneumonia. In the heart of a patient who was treated with antibiotic agents but still died from pneumococcal pneumonia, there are disrupted myocytes and there is a relative absence of neutrophil infiltration. In addition, in experimentally induced infection and without treatment, microcolonies of Streptococcus pneumoniae were present.
Vaccination A meta-analysis of five randomized trials showed a 36% lower risk of a composite of cardiovascular events among adults who had received influenza vaccine than among those who had not. The benefit was even greater when the analysis was limited to persons with known coronary artery disease. In contrast, there are limited data from randomized trials regarding the effect of pneumococcal vaccination on cardiovascular risk. A meta-analysis of eight observational studies, all of which were published after 2000, showed a 17% lower risk of myocardial infarction among patients 65 years of age or older who had received pneumococcal polysaccharide vaccine than among those who had not.40 The lack of a more prominent effect may reflect the decline in the prevalence of pneumococcal pneumonia in recent decades. Summary Practitioners may be able to influence the risk of postinfection myocardial infarction if they remain mindful of the increased risk of myocardial infarction during and after acute infections and if they do not dismiss elevated troponin levels as “troponin leak.” Among patients with acute infection who have clinical indications for statins and aspirin, these medications should be continued (if the patient is already receiving them) or may be initiated if no contraindications are present. Finally, because the risk of other cardiovascular events — such as heart failure, arrhythmias, and strokes — also increases after acute infection, the mechanisms that account for these associations need to be characterized. This is especially important in the case of heart failure, because after pneumonia the risk of worsening heart failure is even higher than the risk of myocardial infarction. An integrated understanding of the interplay between acute infections and the cardiovascular system should facilitate efforts to reduce the risk of myocardial infarction and other cardiovascular events after acute infections.
Ophthalmia Neonatorum
A 2-week-old baby girl with a 3-day history of
purulent discharge from both eyes was brought by
her parents to the ophthalmology clinic. The baby
had been born at full term by means of
spontaneous vaginal delivery. She had not
received ocular prophylaxis after delivery, and the
mother had not undergone prenatal testing for
chlamydia or gonorrhea infection. An eye-
discharge sample obtained from the baby and an
endocervical swab obtained from the mother
tested positive for Chlamydia trachomatis DNA and
negative for Neisseria gonorrhoeae DNA by
polymerase chain reaction. Perinatal transmission
of C. trachomatis or N. gonorrhoeae can result in
neonatal conjunctivitis, known as ophthalmia
neonatorum. The ongoing incidence of ophthalmia
neonatorum caused by C. trachomatis or N.
gonorrhoeae can be addressed by routine
maternal prenatal screening for and treatment of
sexually transmitted infections and by postpartum
neonatal ocular prophylaxis against N.
gonorrhoeae. In addition to treatment of the baby,
which included a 2-week course of oral
erythromycin, a single dose of oral azithromycin
was given to each parent. The baby’s symptoms
resolved within 5 days after the initiation of
treatment, and she remained healthy at follow-up 2
weeks later.“Trachealization” of the Esophagus A 32-year-old man presented to the emergency department with difficulty swallowing oral secretions and the feeling that food was stuck in his throat after he ate a pizza roll. The patient reported that similar episodes had occurred previously, but in each instance the feeling resolved spontaneously, and he did not seek medical care. At the time of presentation, the patient was drooling. Upper endoscopy revealed impacted food material (Panel A) and prominent mucosal rings extending 20 cm from the incisors to the level of the gastroesophageal junction, with two discrete areas of narrowing and associated linear furrows (Panel B). Biopsy specimens were obtained, and esophagitis was observed, with more than 40 eosinophils per high-power field. An endoscopic finding of fixed esophageal rings, or “trachealization,” is suggestive of eosinophilic esophagitis, although a definitive diagnosis is made on the basis of clinical presentation, histologic findings, and the exclusion of other causes of esophageal eosinophilia, such as proton-pump inhibitor–responsive esophageal eosinophilia. The patient was treated with an 8-week course of omeprazole, but there was no symptom resolution or histologic improvement on repeat endoscopic biopsies, which confirmed the diagnosis of eosinophilic esophagitis. He was started on an 8-week course of both swallowed fluticasone and a six-food elimination diet (elimination of the six most commonly identified types of allergenic food — wheat, milk, soy, nuts, eggs, and seafood). No additional endoscopies were performed after completion of treatment with fluticasone and the elimination diet. At a 1-year follow-up visit, the patient reported no further symptoms of food impaction.
Das United States Army Special Forces Command (Airborne) (USASFC; deutsch Luftlande- Sondereinsatzkommando des Heeres der Vereinigten Staaten; kurz Special Forces oder USSF) ist die dienstälteste Spezialeinheit der US Army. Ihre etwa 10.000 Soldaten werden aufgrund ihres grünen Baretts auch Green Berets genannt. Es handelt sich dabei ausschließlich um Kampftruppen, die für ihre Aufträge von anderen Einheiten des United States Army Special Operations Command (USASOC) „Sondereinsatzkräfte des Heeres der Vereinigten Staaten“ unterstützt werden. Bis zum 27. November 1990 hieß die Einheit United States Army 1st Special Operations Command. In der Diktion der US- Streitkräfte steht der Begriff Special Forces traditionell ausschließlich für das USASFC (Green Berets). Die anderen Sondereinsatzkräfte des Heeres, zum Beispiel das 75th Ranger Regiment oder das 160th SOAR, sowie die Spezialeinheiten der anderen Teilstreitkräfte werden unter dem Begriff Special Operations Forces subsumiert. Seit ihrer Aufstellung waren die Special Forces an allen militärischen Konflikten und Kriegen der Vereinigten Staaten mit Ausnahme des Einsatzes in Mogadischu 1993[A 1] beteiligt und leisteten weltweit in über 70 Nationen Militärberatung, infrastrukturelle und humanitäre Hilfe.
A 34-Year-Old Veteran with Multiple Somatic Symptoms A 34-year-old man was evaluated at this hospital because of headaches, cognitive changes, mood symptoms, flashbacks, chest pain, arm tingling, and gastrointestinal symptoms. The patient had served as a special operations combat medic in the U.S. Army Rangers for 8 years. He was wounded several times. He served in Operation Iraqi Freedom, completing three tours of duty. The patient had had multiple traumatic injuries and experiences during training and deployment. Nine years before the current evaluation, during a parachute-jump training, he had a syncopal episode. Afterward, he could recall only that he had awoken on the ground while a colleague was packing his parachute. He had 3 weeks of headaches, stiffness of the cervical and thoracic spine, and difficulty sleeping. Eight years before the current evaluation, the patient was hit by an explosive blast wave. Afterward, he reported “cloudy” mentation. While he served as the company medic, he was a first responder in two cases in which a soldier had committed suicide. Three years later, during his third deployment, the patient was involved in a motor vehicle accident as a helmeted back-seat passenger. The armored fighting vehicle rolled approximately 9 m into a canal, and the patient was pinned under several men. He had blunt trauma to the head and reportedly lost consciousness for 20 minutes; he had a concussion and traumatic injuries of the head and face, including a hard-palate fracture. He subsequently had headaches and difficulty eating and breathing because of lip and nose swelling. After the patient’s third deployment ended, his wife noticed that he placed kitchen items in the wrong location, became lost while grocery shopping, and was unable to recall the birth of his first daughter. The patient expressed difficulty adjusting to a postdeployment routine, which included child care. He mentioned that he missed his level of entrusted responsibility in the Army Rangers platoon. He reported having “deep, lingering pain at deaths of friends and exposures to children in dire circumstances” and “thinking philosophically about death” but did not report suicidal or homicidal ideation. Between 3 and 5 years before the current evaluation, while the patient was still in the military, he sought medical and psychiatric care on three occasions. During the first evaluation, duloxetine was prescribed, but it resulted in a rash and peeling of the skin. Three years before the current evaluation, he received inpatient treatment at a military hospital, which included psychotherapy sessions and muscle relaxation and breathing exercises. Two years before the current evaluation, various medications — including sumatriptan, ibuprofen, prednisone, topiramate, and amitriptyline — were tried, with varying degrees of success.
Twenty-two months before the current evaluation, the patient was honorably discharged from the military, and he moved to New England. Thirteen months before the current evaluation, his condition was assessed by a social worker, psychologist, physical therapist, and neurologist at another hospital. He reported being “constantly on guard” and “easily startled,” as well as having anhedonia, detachment, difficulty concentrating, anorexia, and fatigue. He reported using sarcasm, defensiveness, and intellectualization as coping mechanisms. A review of systems was notable for a reduced ability to move the head and neck to the left and “clicking” with motion of the neck, both of which diminished modestly with physical therapy. Laboratory test results are shown.
A 34-Year-Old Veteran with Multiple Somatic Symptoms Five months before the current evaluation, the patient reported having flashbacks (Wiedererleben oder Nachhallerinnerung) with associated emesis. The next month, he reported that his previous concussion was “acting up.” He described having a “hazy” feeling, verbal stuttering, and severe headaches, which he rated at 10 on a scale of 0 to 10 (with 10 indicating the most severe pain). The headaches lasted for days and were associated with sonophobia and photophobia; he used ice and ibuprofen for relief. He also began to have panic attacks in association with recall of memories. He described having a “rush of visions” of traumatic memories from childhood and the military and being “not able to turn them off”; lorazepam was prescribed. Recurrent pain and tingling of the left anterior chest and left anterior arm developed in association with these memories and later occurred independently of the memories. The patient treated himself for these symptoms with fans, cold baths, and benzodiazepines. The patient’s father had depression, and his mother, father, and paternal uncle each had a history of alcohol and drug use disorders. The patient had been raised by his grandparents. A sister had died in her 20s from bone cancer. The patient lived with his wife and two healthy young children. He had not worked outside the home since his honorable discharge from the military, instead performing child care duties while his wife worked. He had completed 3 years of college; he had thought about additional schooling but felt discouraged because of forgetfulness. The patient had used chewing tobacco in the past but had not used any in 2 years. He consumed up to four caffeinated drinks daily and had only three or four alcoholic drinks monthly, which was a reduction from his past alcohol consumption. He smoked marijuana daily but used no illicit drugs. Medications included nortriptyline, omeprazole, pantoprazole, sucralfate, ondansetron, and as needed, simethicone. On examination, the temperature was 37.1°C, the heart rate 94 beats per minute, the blood pressure 109/74 mm Hg, the respiratory rate 18 breaths per minute, and the oxygen saturation 97% while the patient was breathing ambient air. The weight was 86 kg, and the body-mass index (the weight in kilograms divided by the square of the height in meters) 26.4. The patient was well groomed, alert, cooperative, oriented, and lucid, with coherent speech. He was described as fidgeting, anxious, and irritable. The remainder of the cardiovascular, pulmonary, abdominal, and musculoskeletal examination was normal. A urine toxicology screen was positive for cannabinoids and negative for amphetamines, barbiturates, benzodiazepines, cocaine, opiates, and phencyclidine. A diagnosis was made.
Neurologic Diseases Cerebral aneurysm, vascular dissection, hemorrhage, ischemia, infections (meningitis and encephalitis), and pseudotumor cerebri can all cause headaches, mood symptoms, and cognitive changes. Tumors of the central nervous system (CNS) can cause these symptoms along with emesis and weight loss. Severe headaches or headaches in combination with certain “red flags,” such as focal neurologic signs or systemic illness, may indicate the presence of one of these serious underlying causes. Although imaging studies of the head would be obtained in this case to rule out a clinically significant abnormality of the brain or CNS, the chronic nature of this patient’s symptoms and the absence of other relevant findings most likely rule out a catastrophic neurologic diagnosis. Gastrointestinal Diseases Inflammatory bowel disease could explain the presence of gastrointestinal symptoms. However, although the onset of this disease can occur at any age, it typically occurs before 30 years of age, and the disease is usually associated with blood in the stool and not with vomiting or constipation, which were described by this patient. Endocrine Diseases Hyperthyroidism could explain this patient’s mood symptoms, anxiety, insomnia, diarrhea, and weight loss. However, he had a normal thyrotropin level, a finding that rules out this diagnosis. Toxic Exposures Veterans who served in Operation Iraqi Freedom have a number of potential toxic exposures, including depleted uranium, lead, sand and dust particles, burn pits, oil-well fires, and agents of chemical warfare. However, these exposures are known to result in rashes, widespread pain, respiratory problems, or persistent fatigue, in addition to headaches and cognitive changes. The patient’s symptoms and the timeline of illness are inconsistent with these exposures. Mood and Anxiety Disorders Bipolar disorder, major depressive disorder, and persistent depressive disorder could each explain the presence of mood changes and insomnia. A family history of depression and ongoing anxiety increase the likelihood of a mood disorder. Traumatic Brain Injury Traumatic brain injury (TBI) has developed in 19% of veterans who served in Operation Iraqi Freedom or Operation Enduring Freedom and is the signature wound of these wars. Cognitive consequences of TBI (known as neurocognitive disorder due to TBI) include decreased attention, executive function, learning, memory, language, and social cognition.
Post-Traumatic Stress Disorder Post-traumatic stress disorder (PTSD) is present in 13 to 17% of veterans who served in Operation Iraqi Freedom or Operation Enduring Freedom. PTSD occurs after exposure to a traumatic event and is characterized by re-experiencing of the event (often with physiologic reactions to trauma cues), avoidance of trauma-related thoughts and external reminders, negative alterations in cognition or mood, and hyperarousal.4 PTSD could explain this patient’s mood symptoms, insomnia, flashbacks, hypervigilance, startle, and panic attacks (with associated chest pain and tingling). Furthermore, veterans with PTSD are 4 times as likely to have chronic headaches and 3.5 times as likely to have irritable bowel syndrome as veterans without PTSD.8,9 A diagnosis of PTSD is the most parsimonious explanation of this patient’s panic attacks (a physiologic reaction to trauma cues), rather than an independent panic disorder. A patient must meet eight DSM-5 criteria for the diagnosis of PTSD to be established. The first criterion is direct exposure or indirect exposure (e.g., involving a family member) to a traumatic event. In patients with PTSD, the constellation of symptoms must lead to functional impairment or distress. In addition, to establish the diagnosis of PTSD, substance use and other medical conditions must be ruled out.
Discussion of Management Dr. Mireya F. Nadal-Vicens: Management of PTSD starts with a combination of psychotherapy and treatment with a selective serotonin-reuptake inhibitor or serotonin–norepinephrine reuptake inhibitor. In addition, mirtazapine, prazosin, tricyclic antidepressants, or phenelzine may be administered. At this patient’s initial evaluation, mirtazapine therapy was started, given its soporific and appetite-stimulating effects, but treatment was complicated by the development of a facial rash. Escitalopram therapy was started and was associated with no allergic reactions or unacceptable side effects. A key component of the patient’s treatment was completion of 12 weekly 90-minute sessions of prolonged exposure therapy, which is an evidence-based, trauma-focused method of psychotherapy whose effectiveness is based on mechanisms of habituation and learning. During prolonged exposure, patients are required to confront traumatic memories through repeated imaginal exposures and to decrease avoidance by engaging in feared activities in a hierarchical manner (in vivo exposures). In addition to receiving these interventions, patients who undergo prolonged exposure therapy receive extensive psychoeducation regarding the nature of the effects of trauma and the mechanisms through which prolonged exposure exerts positive effects. Patients are given realistic expectations regarding the degree of difficulty of the treatment. Unfortunately, PTSD is highly prevalent among U.S. veterans. One study showed that among nearly 4.5 million patients who were treated at Veterans Affairs primary care clinics in 2010 to 2011, approximately 9% had a diagnosis of PTSD, more than 25% had depression, 8% had a substance use disorder, and 5% had anxiety. However, among veterans who had returned from service in Iraq, the rate of PTSD was 16% — nearly twice the rate among all veterans. This patient had somatic symptoms, which are very common manifestations of PTSD. Back pain is nearly twice as common among patients with positive PTSD screens as among those with negative PTSD screens (occurring in 40% vs. 22%), and so is joint pain (50% vs. 26%). Headaches are 3 times as common (32% vs. 10%). Gastrointestinal symptoms such as stomachache, nausea, and constipation are also common among patients with PTSD. In response to these statistics, the Veterans Health Administration enacted a collaborative care model in which behavior health specialists were located in the same place as primary care practitioners and were immediately available for visits. The model was designed to improve the identification and treatment of veterans who have PTSD, as well as those who have depression, anxiety, and substance use disorders. Thereafter, mental health care was provided to nearly 6% of patients who were treated at Veterans Affairs primary care clinics, and the results of such treatment suggest decreased substance use, increased adherence to antidepressant regimens, enhanced patient engagement, and reduced stigma against accessing mental health services.
Sie können auch lesen