Aesthetic Facial Surgery - Bilingual Edition (English/German) Heinz Gerhard Bull (ed.)
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Heinz Gerhard Bull (ed.)
Aesthetic Facial Surgery
Bilingual Edition (English/German)
Einhorn-Presse Verlag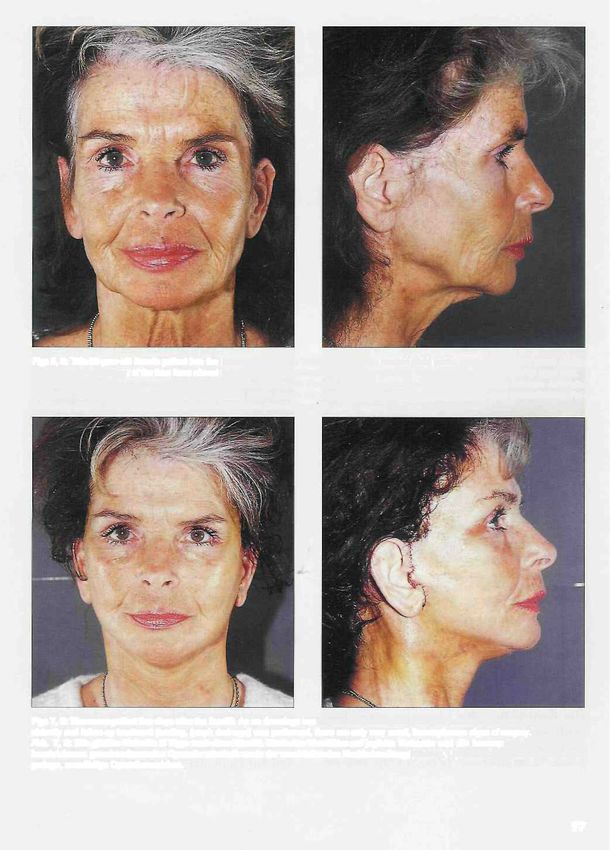
Surgical Rejuvenation
ofthe Face and Neck
Plastisch-chirurgische Verjungung
von Gesicht und Hals
Thomas A.B. Bell • Frank Muggenthaler
Introduction ation ofthe mid-face and the neck. Considera-
An aesthetic surgeon's quest for improved re- tion of overall facial harmony is essential to
sults in facial rejuvenation is based on a thor- achieve a natural non-operated look following
ough understanding of facial anatomy and its surgical rejuvenation of the face. A surgeon
variations as well as development of tech- must have a vision of what looks good for each
niques based on this understanding. patient. One's techniques must then be adapted
The focus of this discussion will be on rejuve- and altered to achieve the best possible result
nation ofthe mid-face and neck. Of course, it is for each specific patient. A sound basis in un-
essential to assess the entire face including derstanding the anatomical changes ofthe ag-
brow position periorbital changes and overall ing face and how best to address these changes
condition ofthe skin in addition to one's evalu- are what are most important.
Einleitung von entscheidender Bedeutung für ein na-
Voraussetzungcn optimaler Ergebnisse in der türliches, ,,unoperiert" wirkendes Ergebnis nach
asthetischen Chirurgie der Gesichtsverjungung der plastisch-chirurgischen Gesichtsverjungung.
sind zunachst genaue Kenntnisse der Anatomie Der Operateur muss eine bildhafte Vorstellung
mit all ihren Variationen und einc stetige Wei- davon haben, von welcher Veränderung jeder
tercntwicklung der Operationstechnik. einzelne Patient asthetisch profitieren würde.
Im Mittelpunkt des folgenden Beitrages stcht Um im Einzelfall das optimale Ergebnis zu
die plastisch-chirurgische Verjungung von Mit- erzielen, muss die eigene Operationstechnik
telgesicht und Hals. Die Beurteilung der Aus- den individuellen Erfordernissen des jeweiligen
gangssituation muss jedoch selbstvcrstandlich Patienten angepasst werden. Von ausschlag-
das gesamte Gesicht einschlieslich Augenbrau- gebender Bedeutung sind dabei die genauen
enposition, periorbitaler Veränderungen und Kenntnisse der anatomischen Veränderungen
allgemeiner Hautbeschaffenhcit umfassen. Die des alternden Gesichtes sowie der optimalen
Beachtung der Gesichtsharmonie insgesamt ist Lösungsansätze zu deren Behebung.
Consultation Evaluation of the existing hairline reveals
One of the most important steps in surgical rejuve- whether it has a youthful appearance or not.
nation of the face and neck is the initial patient If the distance from the lateral corner of
consultation. Our approach has been to have a the brow to the temporal hairline is excessive
seated patient, using a hand held mirror, or the inferior position of the sideburn hairline
review their facial aesthetic concerns. We then is high (above the crus helicis) then the fur-
explain in detail the changes that we see and ther posterior/superior shift of the preauricu-
how we propose to correct them surgically. lar/temporal skin will leave an unacceptable
This discussion will also include issues such as hairline. This discussion of incision placement
anaesthesia, pre and post-op course and full should be carried out with the patient during
disclosure of possible minor and major compli- the consultation. A similar assessment of
cations. Charting of the patient's history shift of post-auricular/neck skin is made
as well as a complete functional inquiry is and recorded. If the skin shift is excessive
also carried out. Appropriate requests for any (>2-3 cm) then a hairline incision is again
pre-operative consultations are then made. considered to avoid dislocating the hairline.
Documentation of a surgical plan for facial A "step-off" is typical in the post-auricular
rejuvenation is essential. Assessment of pre- hairline when a large skin shift is encountered
existing hairlines and the amount of expected (4-6cm), but the surgeon still elects to place
skin shift in both the pre and post auricular the post-auricular incision behind the hair-
areas are the two most important issues. line.
Präoperatives Patientengesprach kular. Der Verlauf des Haaransatzes ist dar-
Einer der wichtigsten Schritte bei der chir- aufhin zu beurteilen, ob er jugendlich wirkt
urgischen Verjüngung von Gesicht und Hals oder nicht. Bei zu grossem Abstand zwischcn
ist das erste Patientengesprach. Der sitzende lateralem Augenbrauenende und tempora-
Patient stellt zunachst mit Hilfe eines lem Haaransatz oder hoher (d.h. oberhalb
HandSpiegels dar, was ihn am eigencn Ge- des Crus helicis) Grenze im Kotelettenbe-
sicht stört. Als nächstes erläutern wir detail- reich führt eine weitere Verschiebung der
liert, wclchc Verandcrungcn moglich er- praeurikularen/temporalen Haut in posteri-
scheinen und welches operative Vorgehen orer bzw. superiorer Richtung zu einem un-
sinnvoll ist. Dieses Gesprach beinhaltet vorteilhaften Verlauf des Haaransatzes. Die
auch das Narkoseverfahren, den prä- und Frage der Schnittfuhrung sollte daher prä-
postoperativen Verlauf sowie eine ausführli- operativ mit dem Patienten erörtcrt werden.
che Aufklarung über sämtliche Komplika- In ähnlicher Weise sind auch die hinter dem
Ohr und im Halsbereich zu erwartenden
tionsmoglichkciten. Die Erhebung eincr um-
Hautverschiebungen zu planen und zu do-
fassenden Anamnese und eines kompletten
kumentieren. Falls stärkere Hautverschie-
Funktionsstatus gehören ebenfalls dazu.
bungen (>2—3 cm) zu erwarten sind, ist zur
Anschliefiend werden gegebenenfalls pra- Vermeidung einer Verlagerung des Haaran-
operativ noch erforderliche Untersuchun- satzes auch hier eine prätricheale Schnitt-
gen veranlasst. führung zu erwagen. Wählt der Operateur
Unverzichtbar ist die Dokumentation einer trotz ausgeprägter Hautverschiebung (4-6 cm)
Operationsplanung für das Facelifting. Die dennoch eine postaurikulare Schnittfuhrung
beiden wichtigsten Aspekte dabei sind der hinter der Haaransatz linie, so resultiert
vorgegebene Verlauf des Haaransatzes sowie zwangslaufig eine Stufenbildung im Verlauf
das Ausmass der zu erwartenden Hautvcr- der postaurikularen Haaransatzlinie.
schiebung sowohl prä- als auch postauri-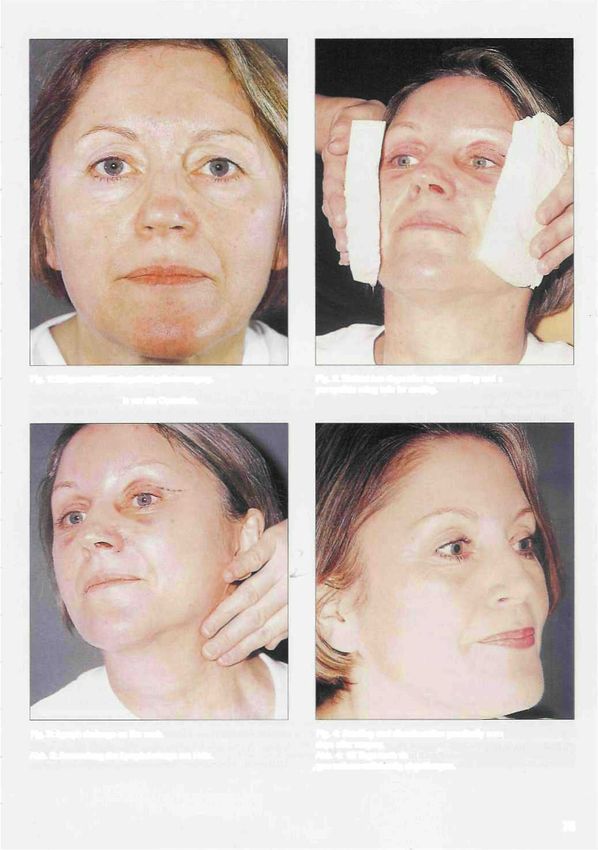
Other issues to assess and record include deep lar healing and ultimately less than ideal scars. tissue ptosis and extent of SMAS dissection to Once the consultation is complete a full set of improve the nasolabial changes as well as ir- pre-operarive photographs are taken. Excellent regularities (jowling) of the mandibular border. quality photographs are essential for documen- Considerations in the neck include extent of tation and may be referred to intraoperatively. looseness of skin, thickness and location ofpre- There are many opportunities to take post- platysmal fat, position of the platysma and operative photographs but only one chance for presence of platysmal bands. Also, is there any pre-operarive photos. We currently use 35mm significant fat deposits deep to the platysma or slide film but will soon switch to digital camera any significant enlargement or ptosis of the systems. submaxillary glands? Lastly, one must consider any form of rejuvenation of the surface of the Anaesthesia skin. We feel that in the majority of cases perio- Neurolept anaesthesia is preferred in the vast ral dermabrasion or perioral laser resurfacing majority of facial rejuvenation patients. In an may be carried out safely with a concurrent otherwise healthy patient the neurolept in- face and necklift. We perform this resurfacing cludes: at the end of the facelift procedure. Full face laser resurfacing with concurrent face and pre-op necklift is placing the cheek flaps at unaccept- - Ativan (Lorazepam) 2.0 mg / sublingual /I - ably high risk for delayed pre and post-auricu- 1 hr pre-op; Darüber hinaus müssen Ptosegrad der tiefen jedoch fur die Hautlappen ein nicht vertretba- Weichgewebsschichtcn sowic die zur Korrcktur res Risiko prä- und postaurikularer Heilungs- von nasolabialen Veranderungen und etwaigen störungen mit daraus resultierenden auffälli- Unregelmafiigkeiten im Unterkieferrandbe- gen Narben. reich erforderliche Ausdehnung der SMAS- Nach dem ersten Patientengesprach werden Praparation (SMAS = superfizielles muskulo- sämtliche praoperativen Fotografien angefer- aponeurotisches System) beurteilt und doku- tigt. Qualitativ hochwertige Fotos sind von ent- mentiert werden. Im Halsbereich müssen Fak- scheidender Bedeutung fur die Dokumentation toren wie Hautlaxitat, Dicke und Lage des pra- und können intraoperativ Hilfestellung leisten. platysmaren Fettgewebes, Platysmalage und Im Gcgcnsatz zu den postoperativen Aufnah- etwaige ,,PIatysmabander" beurteilt werden. men kehrt die Gelegenheit zur Anfertigung Relevante Fettpolster unterhalb des Platysmas praoperativer Bilder nicht zuriick. Zur Zeit ver- oder signifikant vergrösserte bzw. ptotische wenden wir 35mm-Diafilme, werden aber Glandulae submandibulares sind ebenfalls zu demnächst auf ein digitales Aufnahme system erfassen. Die verschiedenen Moglichkeitcn zur umstellen. Verjungung der Hautoberfläche sollten abschlie- end in die Überlegungen einbezogen werden. Anasthesie In der Mehrzahl der Fälle lässt sich eine peri- In den meisten Fallen entscheiden sich die Pati- orale Dermabrasio oder ein Laser-Resurfacing enten gemeinsam mit uns fur eine ,,Neurolept- problemlos mit einem Face- und Halslifting anasthesie", die bei fehlenden Vorerkrankun- kombinieren. Wir fuhren ein solches Resurfac- gen wie folgt durchgefuhrt wird: ing am Ende eines Facelifting-Eingriffs durch. Ein gleichzeitig mit einem Face- und Halslift- präopera tiv ing vorgenommenes vollstandiges Laser-Re- - Lorazepam 2,0 mg sublingual (1/2 bis 1 Stun- surfacing des gesamten Gesichtes bedeutet de praoperativ);

- Sublimaze (Fentanyl) 50 ug. I.V. 5-10 min. Sublimaze 200 pg,
pre-op; - Valium 20 mg,
- Valium (Diazepam) 5mg I.V. pre-op. - Benadryl 200 mg,
- Brietal 100 mg.
in traoperative Antibiotics are rarely used and only where
- Brietal (Methoxital) 30-50mg I.V. titrated specifically indicated. Intraoperative or post-
based on level of consciousness over 60-90 operative steroids are never used. Intraopera-
seconds. During this time local anaethesia is tive monitoring includes continuous E.C.G.
injected - 1/2% Xylcoaine 1:200.000 Epineph- pulse and oxygen saturation. Intermittent
rin approximately 20ml to incision sites and blood pressure is also taken. Intermittent se-
infraorbital and mental nerves on each side quential leg compression and warming blan-
of face. kets are used on most patients.
- 1/4 % Xylocaine 1:400.000 Epinephrin approx-
imately 30-40 ml field block to each side of Surgical Technique
face and neck. Following a brief pre-operative assessment of
During the procedure Sublimaze 25 pg. Valium the patient in the sitting position the inferior ex-
2,5 mg and Benadryl (Diphenhydramine) 20 mg tent of neck dissection is marked. As well, the
are alternated and given to keep the patient in superior extent of the temporal flap is also
a very comfortable but amnesiac state. Total marked bilaterally. The patient is then taken to
dosages for a typical facial rejuvenation case: the operating room and the neurolept anaesthe-
- Fentanyl 50 pg i.v. (5-10 Minuten praopera- - Fentanyl 200 μg,
tiv); - Diazepam 20 mg,
- Diazepam 5,0 mg i.v. (unmittclbar praopera- Diphenhydramin 200 mg,
tiv). - Methohexital 100 mg.
Antibiotika kommen selten, d.h. nur bei Vor-
intraoperativ liegen einer speziellen Indikation, zum Einsatz.
Methohexital 30-50 mg i.v., titriert iiber Kortikosteroide werden weder intra- noch
60-90 s nach Massgabe der Bewusstseinslage. postoperativ verabreicht. Das intraopera-
Wahrend dicser Zeit wird das Lokal- tive Monitoring umfaBt neben der konti-
anasthetikum injiziert; ca. 20 ml Lidocain nuierllchen EKG-Ableitung die Uberwa-
0,5 % mit Adrenalinzusatz [1:200.000] im Be- chung von Herzfrequenz und Sauerstoff-
reich der geplantcn SchnittfCihrung und zur sattigung (Pulsoxymetrie); zusatzlidh crfolgen
beidseittgen Leitungsblockade der Nervi in- intermittierende Blutdruckmessungen. Bei
fraorbitales mid mentales; den meisten Patienten kommen darubcr
- ca. 30-40 ml Lidocain 0,25% mit Adrenalin- hinaus intermittierende, sequentielle Beinkom-
zusatz (1:400.000) als beidseitiger Feld- pression und Warmedecken zur Anwen-
block im seitlichen Gesichts- und Halsbc- dung.
reich.
Im Verlauf des Eingriffs werden abwechselnd Operationstechnik
25 μg Fentanyl, 2,5 mg Diazepam und 20 mg Nach kurzer, praoperativer Untersuchung am
Dephenhydramin verabreicht, um den Paticn- sitzenden Patienten wird die kaudale Grenze
ten in einem entspanntcn und amnestischen der geplanten HaLspraparation angezeichnet
Zustand zu halten. Bei einem typischen Fall Die kraniale Begrenzung der temporalen Lap-
von Gesichtsverjungung ergeben sich folgende penbildung wird ebenfalls beidseits markiert.
Gesamtdosen: Nach Hinlcitung der ,,Neuroleptanasthesie"
71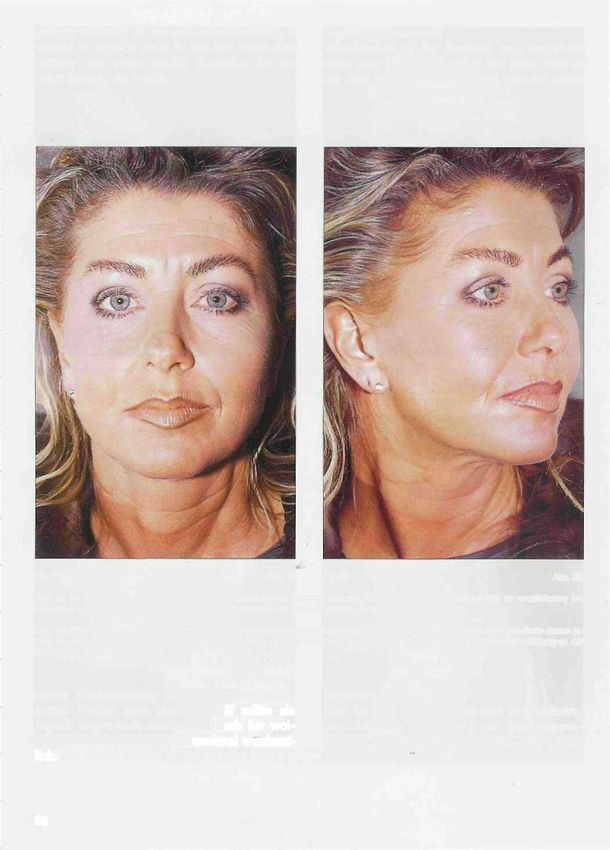
sia is commenced as previously described. The shift is excessive (le. more than 2,5-3,0 cm in the
entire head is prepped with aqueous Zeohryn. temporal area or 4,0-6,0 cm in the post-auricu-
The head is free draped from the base of the lar region) then a portion or the majority ofthe
neck. A sterile child's diaper is placed beneath temporal and post-auricular markings should
the head for its absorbent properties. be at the hairline. This will avoid an unaccept-
able temporal hairlinc/sideburn shift or post-
a) Markings auricular "step" in the hairline.
Based on the consultation and recording of per- The markings around the ear typically include
tinent information the surgical markings are a post-tragal incision.
carried out. Placement of incisions is based on Important considerations include:
pre-existing hairlines and accurate assessment 1. following the curve of helix anteriorly,
ofthe anticipated skin shift both in the tempo- 2. visualizing an appropriate length to the tra-
ral as well as post-auricular regions. If the pa-
gus,
tient has a youthful hairline and the skin shift is
3. the inferior tragal incision should turn at 90°
not excessive then the temporal incisions and towards the lobe. This avoids the telltale tra-
the majority of the post-auricular incision may gal flap anterior to the earlobe,
be placed behind the hailine and is therefore 4. a 1-2 mm rim of cheek skin should be left
well hidden. However, if the hairline is reced- with the earlobe as this gives a much more
ing, if the patient is a secondary facelift with natural appearance when set back into the
previous hairline shift or, if the anticipated skin cheek skin following skin shift,
wird der gesamte Kopf mit wassriger Zephryn- als 2,5-3,0 cm temporal bzw. 4,0-6,0 cm
Losung vorbehandelt; anschliessend erfolgt das postaurikular), sollte die temporale und
Abdecken mit Tüchern in der Wcisc, dass der postaurikulare Schnittfiihrung ubcrwiegend
Kopf bis zur Halsbasis freiliegt. Als äussergst pratrichcal verlaufen. Auf diese Weise wird
saugfahige Unterlage wird z.B. eine sterile eine unvorteilhafte Verlagerung des tempora-
Baby windel unter den Kopf geschoben. len Haaransatzes bzw. cine postaurikulare
Stufenbildung im Verlauf der Haaransatzlinie
a) Schnittfuhrung vermieden.
Entsprechend dem Aufklarungsgesprach Zu der Schnittfuhrung um das Ohr gehort in
und der dokumentierten Befunde werden die der Regel die posttragcale Inzision. Wichtige
Markierungen fiir die Operation eingczeich- Regern hierfur sind:
net. Die Wahl der Schnittführung richtet sich 1. der anterioren Helix-Kriimmung folgen;
nach der Haaransatzlinie und nach einer 2. Tragus korrekt darstellen;
sorgfältigen Abschätzung der zu erwarten- 3. kaudale Tragusinzision sollte im 90°-Winkel
den Hautverschiebungen sowohl temporal auf das Ohrlappchen zulaufen, so daB die
als auch postaurikular. Bei jugendlichem Ver- ,,verraterische" Narbe vor dem Ohrlapp-
lauf der Haaransatzlinie und nur mässiger chen vermieden wird.
Hautverschiebung lassen sich die temporalen 4. 1-2 mm breiten Wangenhautstreifen am
und meistens auch die postaurikularen Inzi- Ohrlappchen belassen, da sich auf diese
sioncn in den behaarten - und somit unsicht- Weise beim Wicdcrcinlagern in die Wange
baren - Bereich legen. Im Falle eines hohen nach erfolgter Hautverschiebung ein we-
Haaransatzes, bei Patienten mit sekundärcm sentlich natiirlicherer Eindruck ergibt.
Face-Lifting nach vorausgegangener Korrek- 5. posteriorc Inzision in der concho-mastoida-
tur des Haaransatzes oder wenn ausgeprägte len Falte und nicht auf der Ruckflache der
Hautverschiebungen zu erwarten sind (mehr Ohrmuschel verlaufen lassen;
72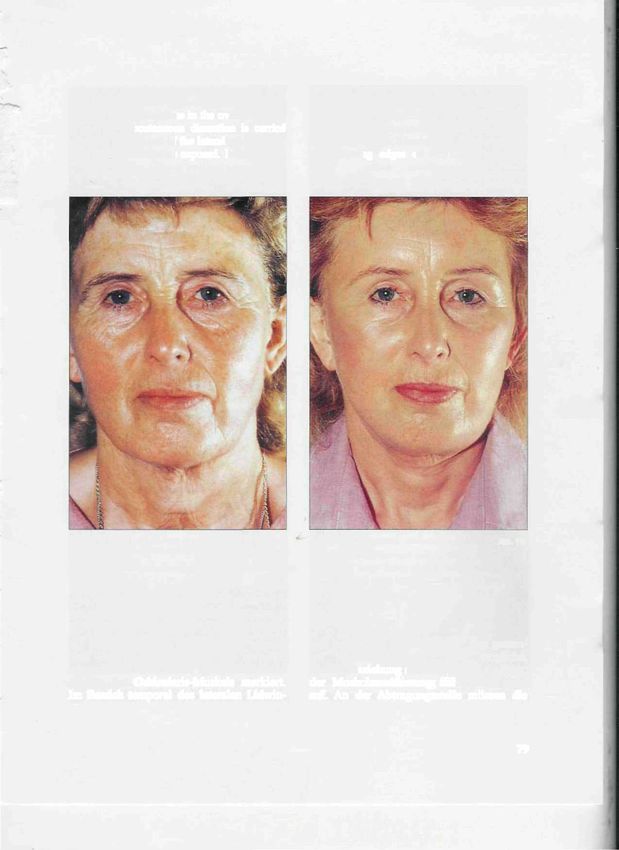
5. the posterior incision should run in the con- poral area to allow for adequate rotation of the
cho-mastoid crease and not up on the con- skin flap. Medially, the dissection exposes the
chal surface,, lateral orbicularis oculi then extends inferiorly
6. in most cases the incision will turn posteri- over the malar prominence where the
orly and inferiorly at a point where the hair- release of the cutaneous ligaments is carried out.
line meets the helical rim. Dissection over the mid-cheek continues inferi-
Other than the skin incisional markings, mark- orly over the chin prominence. The mandibular
ings for SMAS and platysma incisions arc also cutaneous ligaments are always released to im-
placed on the skin. Once the subcutaneous dis- prove the submental contour. This is tine key ma-
section is complete then these markings are noeuvre in correcting a witch's chin deformity.
transferred onto the deep surface with ink. The inferior extent of subcutaneous neck dissec-
tion is based on the pre-op patient assessment.
When midline platysmal muscle work is
The lower the skin shift, subcutaneous excision
planned then a 2 cm long incision is placedjust
of fat or platysmal dissection the lower (more in-
posterior to the mandibular ligament submen-
ferior) the extent of subcutaneous dissection. The
tal crease. lower the extent of subcutaneous dissection an-
teriorly and laterally in the neck the longer and
b) Subcutaneous dissection further posteriorly the post-auricular/ncck inci-
The extent of subcutaneous dissection varies sions must be made to give the best appearance
from patient to patient. Typically, a wide subcu- for red raping of the neck skin.
taneous dissection extends superiorly in the tem-
6. Inzision in der Regel dort nach posterior sung kutaner Anheftungen freiprapariert wird.
und kaudal umwenden, wo sich B e - - Die Praparation im Wangenbereich setzt sich
haarungsgrenze und Helixrand treffen. kaudalwarts iiber die Kinnprominenz hinweg
fort. Zur Vcrbcsserung der submentalen Kon-
Neben den Markierungen fur die Hautschnitt- tur werden etwaige ,,Platysmabander" stets
fuhrung werden auch die vorgesehenen SMAS- durchtrennt. Dies ist das entscheidende
und Platysmainzisionen auf der Haut ange- Manöver zur Korrcktur cines ,,Hexenkinns".
zeichnet. Nach Abschluss der subkutanen Die Ausdehnung der subkutanen Halspräparation-
Praparation werden diese Markierungen mit nach kaudal richtet sich nach dem jeweil-
chirurgischer Tinte auf die tieferen Strukturen igen praoperativen Befund: je weiter kaudal-
libertragen. Falls Platysmakorrekturcn im Mit- warts Hautverschiebung/ subkutane Fett-
tellinienbereich vorgesehen sind, wird eine gewebsabtragung oder Platysmapraparation
2cm lange Inzision unmittelbar posterior der crfolgcn sollen, desto weiter ist die subkutane
Submentalfalte iiber den Flatysmabandern pla- Praparation nach kaudal auszudehnen. Je
ziert. weiter die subkutane Praparation anterior und
b) Subkutane Praparation lateral nach kaudal ausgedehnt wird, desto
Die erforderliche Ausdehnung der subkutanen langer und weiter posterior miissen die post-
Praparation ist von Patient zu Patient unter- aurikularen Inzisionen angelegt werden, um
schiedlich. Nach kranial erfolgt in der Regel bestmogliche Verhaltnisse fur die Wiederanla-
eine grossflaähigc subkutane Praparation der gerung der Halshaut zu schaffen.
Temporalregion, um eine ausreichende Rotati-
on des Hautlappens zu ermöglichen. Nach c) Offene Fettabsaugung am Hals
medial wird der laterale Anteil des Musculus Nach Abschluss der subkutanen Praparation
orbicularis oculi dargestellt, bevor in kaudaler erfolgt die offene Fettabsaugung im Halsbe-
Richtung die Jochbeinprominenz unter Ablö- reich. Unterkieferrand und -winkel werden mit
73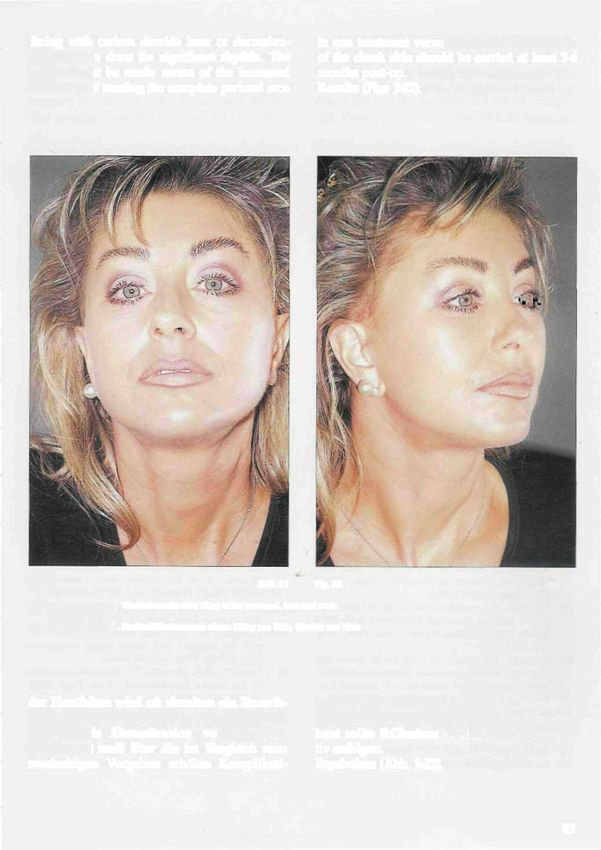
c) Open liposuction ofthe neck point of rotation of the SMAS anteriorly had
Once the subcutaneous dissection is complete/ previously been marked. This point will be-
open liposuction of the neck is performed. The come more prominent from the "dog ear" full-
mandibular border and angle is marked with ink, ness following SMAS rotation and fixation.
Superior rotation of the SMAS/platysma laterally The lateral SMAS incision runs interiorly over
along the jawline requires that you do not remove the platysma. The inferior extent of the SMAS
the preplatysmal fat in this area. Once the SMAS incision varies in each patient (this will be
elevation/rotation is carried out this preplatysmal addressed in the platysma discussion).
fat will be positioned over the jawline/mandibular Alice clamps are used to grasp the SMAS layer
angle. Any excess may then be removed. The open and elevate it from the deeper structures. The
liposuction is carried out with a single hole reverse SMAS incision is then made with small dissect-
angle 6 mm cannula and standard aspirator. A ing scissors. The anterior extent of the SMAS
sweeping motion will pluck the fat cells from the incision carries over the zygomaticus major.
platysmal surface. You do not need any pressure The lateral SMAS incision over the parotid is
on the deep surface when using the cannula. carried inferiorly. This SMAS incision will then
start to divide the superior extent of the platys-
d) SMAS dissection ma muscle laterally. Sharp dissection is then
Ink is used to mark out the SMAS incisions. employed to raise the SMAS flap off the
The superior incision runs along the zygomatic parotid gland and deep fascia overlying the
arch anteriorly to the malar prominence. A masseter. The anterior extent of SMAS eleva-
chirurgischer Tinte markiert. Fiir die Kranial- dieser Bereich prominenter. Die laterale SMAS-
rotation von SMAS und Platysma im lateralen lnzision verläuft kaudalwärts über das Platys-
Bereich entlang dem Unterkieferrand darf ma. Die kaudale Ausdehnung der SMAS-Inzi-
das präplatysmare Fettgewebe in diesem Be- sion wird bei jedem Patienten individuell ge-
reich nicht entfernt werden. Erst wenn sich die- wählt (eingehendere Erörterung im Abschnitt
ses praplatysmare Fettgewebe nach SMAS-Ele- zur Platysma Präparation).
vati on/Rotation über dem Unterkieferrand Die SMAS-Schicht wird mit Klemmen gefasst und
und -winkel befindet, kann ein etwaiger Über- von den tieferen Schichten angehoben. Es folgt
schuss entfernt werden. Die offene Fettabsau- die SMAS-Inzision mit einer feinen Praparicr-
gung wird mit einer einlumigen, nach rück- schere. Die anteriore Ausdehnung der SMAS-In-
warts umgebogencn 6 mm-Kanule und cincm zision rcicht bis übcr den Musculus zygomaticus
Standardsaugcr vorgenommen. Mit einer major hinweg. Die laterale SMAS-Inzision iiber
Wischbewegung lassen sich die Fettzellen von der Glandula parotis wird nach kaudal geftihrt,
der Platysmaoberfläche ablösen. Bei Verwen-
wo sie den oberen Anteil der Platysmamuskula-
dung der Kanule braucht kein Druck auf die
tur lateral durchtrennt. Durch scharfe Präparati-
Oberfläche der ticfen Strukturen ausgeübt zu
on wird nun der SMAS-Lappen von Glandula
werden.
parotis und tiefer Faszie über dem Musculus
masseter abgelöst. Die Ausdehnung der SMAS-
d) SMAS-Praparatton Praparation nach anterior variiert. Durch Lösen
Mit chirurgischer Tinte werden die SMAS-Inzi- der Ligamente in der Jochbeinregion wird eine
sionen markiert. Die obere Inzision verlauft starkere SMAS-Verschiebung ermöglicht. Zug
vor der Jochbeinpromincnz am Jochbogcn ent- am SMAS-Lappcn solltc cine Bewegung im mitt-
lang. Bereits zuvor wurde ein anteriorer Dreh- leren Oberlippenbereich und die gewünschte
punkt fiir die SMAS-Rotation angezeichnet. In- Verschiebung der tiefen Gewebeschichten iiber
folge der SMAS-Rotation und -Fixierung wird dem Unterkieferrand bewirken.
74
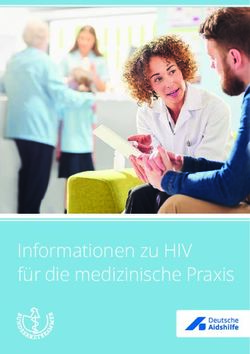
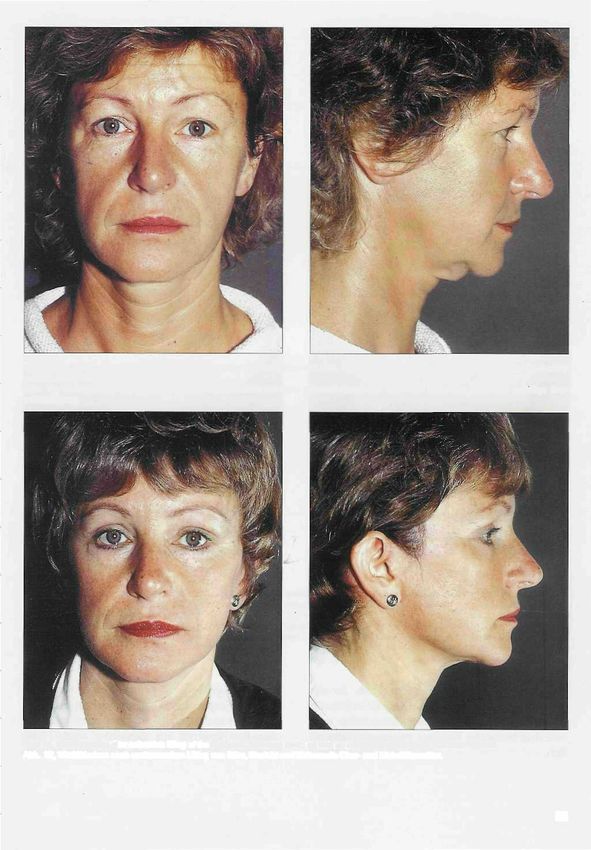
Fig. 1: 52-year-old female patient prior to surgery. Fig. 2. Patient two days after eyebrow lifting and correction ofthe up-
pereyelids using tofu for cooling.
Abb. 1: 52jahrige Patientin vor der Operation. Abb. 2: Patientin 2wei Tage nach eirtem Lifting der Augenbrauen und
einer Korrektur der Oberiider bei der Anwendung von Tofu zur Kuhlung.
Fig. 3: Lymphatic drainage on the neck. Fig. 4: Swelling and discolouration practically completely subsided 10
days alter surgery.
Abb. 3: Anwendung der Lymphdrainage am Hals. Abb. 4: 10 Tage nach dem Eingriil sind Schwellungen und Verfärbun-
gen nahezu vollstandig abgeklungen.
75tiort is variable. Release of the zygomatic liga- f) Platysma dissection
ments will allow increased shift of the SMAS. Meical platysma banding is a very common de-
Traction on the SMAS flap should translate into formity of the aging neck. The medial aspects of
movement of the medial portions of the upper each platysmal sheet appear to shorten with age
lip and adequate shift ofthe deep tissues over creating the tight medial banding effect. If this is
the mandibular border. the case then release of the medial platysma from
the submental area inferiorly to the cricoid is car-
e) SMAS flaps ried out. Any existing platysma decussation is
The excess of SMAS may be excised prior to su- excised at this point. A partial lateral release of
turing - or may be used as SMAS flaps. The su- the medial band for 2-3 cm may be done at the
perior flap may be secured to the deep temporal cricoid level. If the platysmal muscles are gene-
fascia and help to elevate the superior portions rally tight, then a full width release ofthe platys-
of the nasolabial fold. The more commonly used ma will give the best results. The platysma divi-
lateral SMAS flap is rotated posteriorly and se- sion in the lateral neck is continous with the
cured over tlie mastoid area. This flap helps to SMAS dissection above. A division ofthe platys-
support the platysma in the neck and may be of ma is approximately 1 cm medial and paralleling
benefit in supporting ptotic submaxillary glands. the sternocleidomastoid muscle. Very low in the
Suturing ofthe SMAS and the SMAS flaps is neck the platysma division is then swung medi-
done with a combination of 4-0 nylon and 4-0 ally at the level of the cricoid to complete the full
vicryl sutures. width transection.
e) SMAS-Lappen gelöst. Gleichzeitig werden etwaige kreuzende
Überschüssige SMAS-Antcile konnen entweder Platysmafasern exzidiert. Auf Hohe des Ring-
vor dem Vernähen exzidiert oder aber als knorpels kann einc partielle laterale Lösung des
SMAS-Vcrschiebelappen genutzt werden. Der medialen Platysmabandes über eine Strecke
kraniale Lappen lässt sich mit Nähten an die von 2-3 cm vorgenommen werden. Ist die Pla-
ticfe Temporalisfaszie heften und so zur Anhe- tysmamuskulatur insgesamt zu straff, ergibt
bung der kranialen Anteile der Nasolabialfalte eine vollständige Lösung des Platysmas auf
nutzen. Der häufiger vcrwendete laterale ganzer Breite die besten Ergebnisse. Die Platys-
SMAS-Lappen wird nach posterior rotiert und maspaltung im lateralen Halsbereich geht in die
über dem Mastoidbereich fixiert. Dieser Lap- oben beschricbene SMAS-Praparation iiber. Das
pen trägt zur Platysmastraffung im Halsbe- Platysma wird ungefähr 1 cm medial vom und
reich bei und kann auch ptotische Glandulac parallel zum Musculus sternocleidomastoideus
submandibulares stützen. durchtrennt. Sehr weit kaudal im Halsbereich
Zum Nahtverschlufi des SMAS bzw. zur An- wird die Platysmaspaltung auf Hohe des Ring-
naht der SMAS-Lappen wird Nylon 4-0 in knorpels nach medial geführt, um die Durch-
Kombination mit Vicryl 4-0 verwendet. trennung auf ganzer Breite zu vervollständigen.
Sind die Platysmabänder nicht verkiirzt oder
f) Platysmapräparation gespannt, sondern eher locker und schlaff, so
Mediane ,,Platysmabänder" sind eine sehr häu- wird ein eventuell vorhandener mediancr Über-
fige Altersveränderung
schuss exzidiert. im Halsbereich.
Nach entsprechender Präpara-Die me-
dialen Anteile beider Platysmahälften verkür- tion und Lösung des Platysmas werden die me-
zen sich offenbar im Alter, so daβ der Eindruck dialen Platysmaränder von der Submcntalregi-
straffer, medialer Bänder entsteht. In solchen on bis hinab zum Hyoidbereich vernäht. Derzeit
Fällen werden die medialen Platysma- verwenden wir hierfiir eine zweischichtige, fort-
fasern submental bis hinab zum Ringknorpcl laufende Mersilene-Naht der Fadenstarke 4-0.
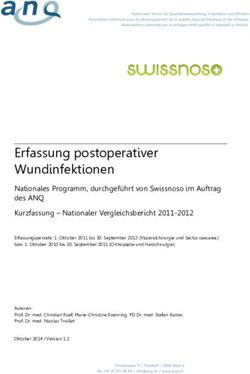
76Figs 5, 6: This 61-year-old female patient has the ideal conditions for a facelift as she has a marked facial profile with very prominent cheek bones.
The slackened soft tissues ofthe face have altered facial proportions and caused generalized wrinkling. This marks the appearance of an aged face.
Abb. 5, 6: Die 61jahrige Patientin bietet ideale-Voraussctzungen fur ein Facelift, da sie ein markantes Gesichtsprofil mit einer betonten Jochbein-
prominenz aufweist. Die erschlafften Gesichtsweichteile haben sowohl die Gesichtsproportionen verändert als auch zu einer generalisierten Fal-
tenbildung geführt. Dadurch wird der Eindruck des gealterten Gesichtes geprägt.
Figs 7, 8: The same patient five days after the facelift. As no dressings were used, the tissue-sparing surgical technique described was used con-
sistently and follow-up treatment (cooling, lymphatic drainage) was performed, there are only very small, inconspicuous signs of surgery.
Abb. 7, 8: Die gleiche Patienin 5 Tage nach dem Facelift. Dank des Verzichtes auf jegliche Verbände und die konsequente Anwendung der
beschriebenen gewebeschonenden Operationstechnik sowie der anschliessenden Nachbehandlung (Kühlung, Lymphdrainage) bestehen nur sehr
geringe, unauffallige Operationszeichen.
77If the platysma banding is not short or tight but currently use 2 layers of running 4-0 mersilene instead seems loose and floppy then any appar- sutures. ent midline excess is excised. Once the appropri- ate platysma dissection and release are complete g) Thinning of orbicularis oculi muscle the medial platysma edges are sutured from the The sphincter action of the orbicularis oculi is submental area down to the hyoid region. We a depressor of the lateral brow. Excessive Fig. 9: In this 62-year-old female patient, there is marked ptosis of all soft Fig. 10: Seven days after lifting the forehead, face and neck. The tissues of the face. The eyebrows have dropped, faking ptosis (pseudopto- neck could be clearly defined again due to extensive modelling of fat sis) of the upper eyelids. There is also marked slackening of the neck. deposits and resuspension of the platysma. Abb. 9: Bei dieser 62jahrigen Patientin besteht eirie ausgeprägte Ptose Abb. 10: 7 Tage nach einem Lifting von Stim, Gesicht und Hals. der gesamten Gesichtsweichteile. Die Augenbrauen haben sich gesenkt, Durch eine umfangreiche Modellierung der Fettansammlungen und wodurch eine Ptose (Pseudoptose) der Oberlider vorgetäuscht wird. Resuspension des Platysmas konnte die kiare Definition des Halses Daneben liegt eine ausgeprägte Erschlaffung der Halspartie vor. wiederhergestellt werden. g) Ausdünnung des M. orbicularis oculi nen die laterale Augenbraue herabgezogen, Die Kontraktion des Musculus orbicularis zum anderen entstehen ,,Krähenfüsse"-artige oculi zieht die laterale Augenbraue nach Veränderungen der darüberliegenden unten. Im Falle cincr Hyperaktivitat dieses Haut. Bei subkutaner Preparation nach me- Muskels im lateralen Bereich wird zum ei- dial auf Hohe der lateralen Orbita kommen 78
action of the lateral orbicularis oculi will mark the area of the orbicularis to be thinned.
depress the lateral brow as well as create The full thickness thinning of this muscle is
"crow's feet" deformities in the overlying skin. done over the area lateral to the lateral canthus.
When the subcutaneous dissection is carried A possible slight depression in this area as a re-
medially at the level of the lateral orbit, the la- sult of the muscle thinning will not be noticed.
teral orbicularis oculi is exposed. Ink is used to The thinning edges of the muscle must be
Fig. 11a Abb. 11a ' Fig. 11b Abb. 11b
Figs 11a, b: The same patient priort o (a) and 20 days after (b) surgery.
Abb. 11a, b: Dieselbe Patientin vor (a) und 20 age nach (b) dem Eingriff.
die lateralen Anteile des Musculus orbicu- kels betrifft die ,,Ausdünnung" den gesam-
laris oculi zur Darstellung. Mit chirurgi- ten Muskelquerschnitt. Eine mögliche,
scher Tinte werden die auszudünnenden leichte Einziehung an dieser Stelle als Folgc
Anteile des Orbicularis-Muskels markiert. der Muskcl ausdünnung fällt spater nicht
Im Bereich temporal des lateralen Lidwin- auf. An der Abtragungsstelle miissen die
79bevelled so as not to create a noticeable ridge in The excess of skin is pulled in the appropriate
this area. Care must to be taken in thinning the posterior-superior direction. Skin tension is judged
lateral most portion of this muscle as the with the use of the D'ASSUMPCAO marker. A 4-0
frontal brach of the facial nerve may be in- nylon suture is used to secure the skin flap at the
creased risk in this area. key points. The post-auricular key point is ap-
proximately 3 cm posterior to the conchal carti-
h) Irrigation and insertion of drains lage along the hairline. The D'ASSUMPCAO marker
The subcutaneous plane throughout the face is again used. The skin excess to be excised is
and neck is irrigated thoroughly with saline. A measured and recorded the remaining skin in-
final check for hemostasis is carried out. A sin- cluding the skin around the ear is trimmed so
gle round 4 mm JACKSON-PRATT drain is placed that there is no tension on the closure.
through a separate post-auricular stab incision.
The drain is placed across the neck and left in j) Suturing
place overnight. Once all of the skin excess is excised the skin su-
turing is carried out. Behind the hairline skin
i) Points offixation staples are used. Along the hairline half - buried
Two key points of fixation are used when posi- vertical mattress 4-0 nylon sutures are used as
tioning and suturing the skin flap. The well as individual and running 6-0 nylon su-
tcmporal/pre-auricular key point is approxi- tures to approximate the skin edge. If the origi-
mately 1-2 cm above the crus helix. nal key sutures seem too tight they are replaced.
Muskelränder angeschragt werden, damit Richtung nach hinten oben gezogen. Mit Hilfe
keine sichtbare Stufe zuruckblcibt. Beson- des D'AssuMPCAO-Markers wird die Hautspan-
dere Sorgfalt ist bcim Ausdünnen der nung beurteilt. Anschliefiend wird der Haut-
äussersten latcralen Muskelfasern geboten, lappen mit einem Nylonfaden der Stärke 4-0
da hier der Stirnast des Nervus facialis er- an den Schlüsselstellen fixiert. Die postauri-
hebheh gefahrdet ist. kuläre Schlüsselstelle liegt etwa 3 cm hinter
dem Conchaknorpel im Verlauf der Haaran-
h) Spiülung und Drainage satzlinie. Auch hier wird der D'ASSUMPCAO-
Die eröffnete Subkutanschicht des gesamten Marker benutzt. Der zu exzidicrende Haut-
Gesichtsbereichs wird gründlich mit Kochsalz- überschuss wird gemessen und dokumentiert.
losung gcspült. Abschlicssend wird noch ein- Die Haut - einschliefilich der periaurikularen
mal die Blutstillung kontrolliert. Es folgt das Anteile - wird anschliefiend so exakt eingepafit,
Einbringen eines runden 4 mm-Drains nach dafi jegliche Spannung auf die Naht vermieden
JACKSON-PRATT über cine separate Stichinzision wird.
postaurikular. Der Drain wird quer über den
Hals verlaufend plaziert und über Nacht belas- /) Naht
sen. Nach Resektion des Hautuberschusses folgt die
Hautnaht. Im behaarten Bereich werden Haut-
i) Fixationsnähte klammern verwendet, wahrend entlang des
Die Repositionierung und Annaht des Haut- Haaransatzes vertikale Riickstichnahte mit Ny-
lappens orientiert sich an zwei Schlüsselstcl- lon 4-0 sowie Einzelknopfnahte oder fortlau-
len. Die temporale/präaurikularc Schlüssel- fende Nahte mit Nylon 6-0 zur Adaptation der
stelle liegt etwa 1-2 cm oberhalb der des Crus Hautrander gelegt werden. Sollten die ur-
helicis. spriinglichen Nahte an den Schlusselstellen zu
Der Hautüberschuss wird in die entsprechende straff erscheinen, werden sie erneuert.
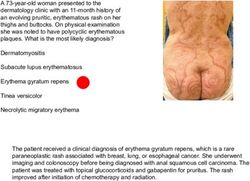
80Fig, 12; 38-year-old female patient with ptosis of the forehead, face Fig. 13: The same patient three weeks after extensive lifting of the fore-
and neck and dermatochalasis ofthe upper and lower eyelids. head, face and neck as well as correction of the upper and lower eyelids.
Abb. 12: 38- jährige Patientin mit Ptose von Stirn, Gesicht und Hals Abb. 13: Dieselbe Patientin drei Wochen nach urnfassendem Lifting
und Dermatochalasis der Ober- und Unterlider. von Stirn, Gesicht und Hals sowie Ober- und Unteriidkorrektur.
Fig. 14a Abb, 14a Fig, 14b Abb. 14b
Figs 14a, b: The same patient prior to and three weeks after surgery.
Abb. 14a, b: Dieselbe Patientin vor und drei Wochen nach dem Eingriff.
81Post-Op four days depending on the intervention, cool- A light absorbent dressing is applied in a tur- ing, avoidance of pressure and stimulation of ban style. This is not a pressure dressing and lymph flow are the three most crucial measures does not involve the submental or neck area. to be taken. Compression type dressings possibly constrict Cooling can be performed using special cold lymphatic and return and potentially create masks. The use of TOFU has proved to be very healing problems. Post-operative overnight favourable. When cut in strips and soaked in monitoring is carried out by a registered nurse icy water, it conforms ideally to the contours of in a private room at our facility. The next morn- the face and also exercises a soothing effect on ing, the dressing and drain are removed and wounds. Any pressure on any places where the the patient takes a shower and washes hi s/her skin was detached from its base during surgery hair before leaving the clinic. leads to an increase in swelling, a feeling of ten- Generally/ the patient will return on DAY 3 sion, hyperthermia and increased discoloura- post-op for removal of the 6-0 skin edge su- tion due to limited circulation. Thus, ifpossi- tures and again on DAY 8 post-op for removal ble, no compression bandages should be ap- of all remaining sutures and staples. Further plied after surgery and facial massage should post-operative visits are at 1 month, 3 months, notbe performed for two to three weeks. 6 months and one year. Correct lymph drainage starts below the oper- In the first phase after surgery, which begins ated zones. This means in the cheek region and with the end of surgery and lasts for two to on the neck after forcheadplasty or eyelid Postoperative Nachsorge nach Eingriff 2-4 Tage andauert, sind vor allem Es wird ein leichter, saugfhäiger Turbanver- drei Massnahmen entscheidend: Kühlung, das band angelegt, der Submentalregion und Hals Vermeiden von Druck und das Anregen des unbedeckt lasst und ausdrücklich nicht als Lymphabflusses. Druckverband dient. Kompressionsverbande Die Kühlung kann durch spezielle Kältemas- können zu einem Lymphstau mit der mögli- ken erfolgen. Als sehr vorteilhaft hat sich chen Folge einer Heilungsstorung fiihren. Post- hierfur auch die Anwendung von TOFU er- operativ vcrbleiben die Patienten fur eine wiesen. In Streifen geschnitten und getränkt Nacht unter der Aufsicht einer examinierten in Eiswasser lässt es sich ideal dem Ge- Pflegekraft auf unserer Abteilung. Am nach- sicht anschmiegen und übt zusatzlich eine sten Morgen werden Verband und Drain ent- lindernde Wirkung aus. An den Stellen, an fernt, so dass der Patient noch vor der Entlas- denen die Haut während der Operation von sung duschen und sich die Haare waschen ihrer Unterlagc abgelöst worden war, führt kann. jeglicher Druck zu einer Zunahme von In der Regel werden die Patienten zur Entfer- Schwellungen, Spannungsgefühl, Überwär- nung der 6-0-Hautnahte fur den 3. postopcrati- mung und wegen der eingeschränkten ven Tag und zur Entfernung der restlichen Durchblutung zu verstärkten Verfärbungen. Nahte und Hautklammern fiir den 8. postope- Daher sollten nach der Operation moglichst rativen Tag wiedereinbestellt. Es folgen weitere kcine Druckverbande angelegt und fiir zwei Verlaufskontrollen nach 1, 3, 6 und 12 Mona- bis drei Wochen auf Gesichtsmassagen ver- ten. Im Rahmcn des Nachschautermins nach zichtet werden. einem Jahr werden postoperative Fotos angc- Die richtige Lymphdrainage setzt unterhalb fertigt. der operierten Zonen an. Das heisst, nach ei- In der ersten Phase nach der Operation, die di- nem Stirnlifting oder einer Li dope ration an rekt mit dem Operationsende beginnt und je der Wangengegend und am Hals, nach 82
Figs 15, 16: 48-year-old female patient with ptosis ofthe forehead, face and skin, derrnatochalasis of the upper and lower eyelids. Particularly
marked double chin.
Abb. 15, 16: 48 jahrige Patientin mit Ptose von Stirn, Gesicht urid Hals, Dermatochalasis der Ober- und Unterlider; besonders auffällige Dop-
pelkinnbildung.
Figs 17, 18: Six weeks after extensive lifting ofthe forehead, face and neck, as well as correction ofthe upper and lower eyelids.
Abb. 17, 18:6Wochen nach umfassendem Lifting von Stim, Gesicht und Hals sowie Ober- und Llnterlidkorrektur.
83Post-Op four days dependng on the intervention, cool- A light absorbent dressing is applied in a tur- ing, avoidance of pressure and stimulation of ban style. This is not a pressure dressing and lymph flow arc the three most crucial measures does not involve the submental or neck area. to be taken. Compression type dressings possibly constrict Cooling can be performed using special cold lymphatic and return and potentially create masks. The use of TOFU has proved to be very healing problems. Post-operative overnight favourable. When cut in strips and soaked in monitoring is carried out by a registered nurse icy water, it conforms ideally to the contours of in a private room at our facility. The next morn- the face and also exercises a soothing effect on ing, the dressing and drain are removed and wounds. Any pressure on any places where the the patient takes a shower and washes hi s/her skin was detached from its base during surgery hair before leaving the clinic. leads to an increase in swelling, a feeling of ten- Generally, the patient will return on DAY 3 sion, hyperthermia and increased discoloura- post-op for removal of the 6-0 skin edge su- tion due to limited circulation. Thus, ifpossi- tures and again on DAY 8 post-op for removal ble, no compression bandages should be ap- of all remaining sutures and staples. Further plied after surgery and facial massage should post-operative visits are at 1 month, 3 months, not be performed for two to three weeks. 6 months and one year. Correct lymph drainage starts below the oper- In the first phase after surgery, which begins ated zones. This means in the cheek region and with the end of surgery and lasts for two to on the neck after foreheadplasty or eyelid Postoperative Nachsorge nach Eingriff 2-4 Tage andauert, sind vor allem Es wird ein leichter, saugfäiiger Turbanver- drei Mafinahmen entscheidend: Kiihlung, das band angelegt, der Submentalregion und Hals Vermeiden von Druck und das Anregen des unbedeckt lässt und ausdrucklich nicht als Lymphabflusses. Druckverband dient. Kompressionsverbande Die Kuhlung kann durch spcziclle K a ltemas- können zu einem Lymphstau mit der mögli- ken erfolgen. Als sehr vorteiihaft hat sich chen Folge einer Heilungsstorung fiihren. Post- hierfur auch die Anwendung von TOFU er- operativ verbleiben die Patienten fiir eine wiesen. In Streifen geschnitten und getrankt Nacht unter der Aufsicht einer examinierten in Eiswasscr lafit cs sich ideal dem Ge- Pflegekraft auf unserer Abteilung. Am näch- sicht anschmiegen und iibt zusatzlich eine sten Morgen werden Verband und Drain ent- lindernde Wirkung aus. An den Stellen, an fernt, so dass der Patient noch vor der Entlas- denen die Haut wahrend der Operation von sung duschen und sich die Haare waschen ihrer Unterlage abgelost worden war, fuhrt kann. jeglicher Druck zu einer Zunahme von In der Regel werden die Patienten zur Entfer- Schwellungen, Spannungsgefuhl, Uberwar- nung der 6-0-Hautnahte fur den 3. postoperati- mung und wcgcn der cingeschrankten ven Tag und zur Entfernung der restlichen Durchblutung zu verstarkten Verfarbungen. Nähte und Hautklammern fiir den 8. postope- Daher sollten nach der Operation moglichst rativen Tag wiedereinbestellt. Es folgen weitere keine Druckverbande angelegt und fur zwei Verlaufskontrollen nach 1, 3, 6 und 12 Mona- bis drei Wochen auf Gesichtsmassagen ver- ten, im Rahmen des Nachschautermins nach zichtet werden. eincm Jahr werden postoperative Fotos ange- Die rkhtige Lymphdrainage setzt unterhalb fertigt. der operierten Zonen an. Das heiSt, nach ei- In der ersten Phase nach der Operation, die di- nem Stimlifting oder einer Lidoperation an rekt mit dem Operationsende beginnt und je der Wangengegend und am Hals, nach 82
surgery and only on the neck after facelifting. It Ancillary Procedures should be applied daily in the first week after Rejuvenation of the forehead and periorbital surgery and twice weekly thereafter for an- areas may be carried out at the same time as other three to six weeks. the face and neck. Concurrent perioral resur- Fig. 19 Abb. 19 Fig. 20 Abb 20 Figs 19, 20: Facelifting had been performed in this female patient 1 years previously. She felt that this had achieved only an unsatisfactory im- provement in her appearance. In objective terms, there was still very marked wrinkling on the forehead and cheeks. Abb. 19, 20: Bei dieser 52jahrigen Patientin war 1 H Jahre zuvor ein Facelifting durchgefuhrt worden Ihrem Empfinden nach resultierte daraus je- doch nur eine unzureichende Verbesserung ihres Aussehens. Objektiv bestanden immer noch sehr auffallige und pragende Faltenbildung an cter Stim und im Bereich derWangen. einem Gesichtslifting nur am Hals. In der Begleiteingriffe ersten Woche nach dem Eingriff sollte sie Eine Verjiingung von Sfirn und Periorbitalre- taglich angewandt werden. Danach für wei- gion lafit sich gleichzeitig mit dem entspre- tere drei bis sechs Wochen zweimal wochent- chenden Eingriff im Gesichts- und Hals- lich. bereich durchfuhren. Zur Korrektur storen- 84
facing with carbon dioxide laser or dermabra- in one treatment versus two. Laser resurfacing
sion is often done for significant rhytids. The of the cheek skin should be carried at least 3-6
patient must be made aware of the increased months post-op.
morbidity of treating the complete perioral area Results (Figs 1-22).
Fig. 21 Abb. 21 Fig. 22 Abb. 22
Figs 2 1 , 22: The same patient six weeks after lifting ofthe forehead, face and neck.
Abb. 2 1, 22: Dieseibe Patientin 6 Wochen nach einem Lifting von Stim, Gesichl und Hals.
der Hautfalten wird oft simultan ein Resurfa- onsrate der einzeitigen Korrektur aufgeklart
cing der perioralen Haut mit dem CO2-Lascr werden. Bin Laser-Resurfacing der Wangen-
oder mittels Dermabrasion vorgenommen. haut sollte frCihcstens 3-6 Monate postopera-
Der Patient mufi iiber die im Vergleich zum tiv erfolgen.
zweizeitigen Vorgehen erhohte Komplikati- Ergebnisse (Abb. 1-22).
85Summary Our objectives with this surgery are to create a
This discussion of mid-face and neck rejuvena- previously mentioned rejuvenation of the face
tion summarizes our current thoughts on how and neck must be harmonious with the forehead
we attempt to achieve our best possible results. and periorbital areas for the best possible results.
Zusammenfassung beshnogliche Ergebnisse zu erzielen, sind wir
Die vorliegende Erorterung der plastisch-chir- bei diesen Eingriffen bestrebt, eine mit der
urgischen Mittelgesichts- und Halsverjungung Stirn- und Periorbitalregion harmonierende
gibt einen Uberblick ubcr die nach unseren Verjungung von Gesicht und Hals zu
Erfahrungen aussichtsreichste Methodik. Um erzielen.
References - Literatur fascias. Relevance to rhytidectomy and aging.
(1) MITZ, V., PEYRONIE, M.: The superficial musculo- Plast. Reconstr. Surg. 89,441-449 (1992)
aponeurotic system (SMAS) in the parotid and (7) FURNAS, D.: The retaining ligaments of the
cheek aiea. Plast. Reconstr. Surg. 58-80 (1976) cheek. Plast. Reconstr. Surg. 83,11-16 (1989)
(2) RANDALL, P., SKTLES, M.S.: The "SMAS sling". An (8) CONNELL, B.F., MARTEN, T.J.: Submental crease:
additional fixation in face lift surgery. Ann Elimination of the double chin deformity at
Plast. Surg. 12,5-9(1984) ihytidectomy. Aesthet. Surg. 10,10-11 (1990)
(3) CONNELL, B.F.: Cervical lift: Surgical Correction (9) LAMBROS, V.: Fat contouring in the face and
of Fat contour Problems Combined with Full- neck. Climes Plast. Surg. 19,401-413 (1992)
Width Platysma Muscle Flaps. Ann. Plast. Surg. (10) CONNELL, B.F.: Face and neck lifts; SMAS vec-
355-362 (1978) tors for support and smile crease correction.
(4) CONNELL, B.F.: Neck Contour Deformities; The Can. J. Plast. Surg. 1, 75-82 (1993)
ATt, Engineering, Anatomic Diagnosis, Architec- (11) CONNELL, B.F., MARTEN., T.J.: Surgical correction
tural Planning and Aesthetics of Surgical Cor- of the crow's feet deformity, Clin. Plast. Surg.
rection. Clinics Plast. Surg. 14,683-692 (1987) 20,295-302 (1993)
(5) GuYUKON, B.: Modified Temple Incision for Fa- (12) Marten, T.J.: Physician administered office
cial Rhytidectomy Ann. Plast. Surg. 21, 439-443 anaesthesia. Clin. Plast. Surg. 18, 877-889 (1991)
(1988) (13) CONNELL, B.F., MARTEN, T.J.: Deep-Layer Tech-
(6) STUZIN, J.M., BAKER, T.K., GORDON, H.L.: The niques in Cervicofacial Rejuvenation. Deep
relationship of the superficial and deep facial Face-Lifting Techniques. Thieme, 161-190 (1994)
86Sie können auch lesen