Kolon- und Rektumkarzinom Immuntherapeutische Ansätze - Studien - Susanna Hegewisch-Becker Hämatologisch-Onkologische Schwerpunktpraxis Hamburg...
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Kolon- und Rektumkarzinom
Immuntherapeutische Ansätze - Studien
Susanna Hegewisch-Becker
Hämatologisch-Onkologische Schwerpunktpraxis Hamburg-
Eppendorf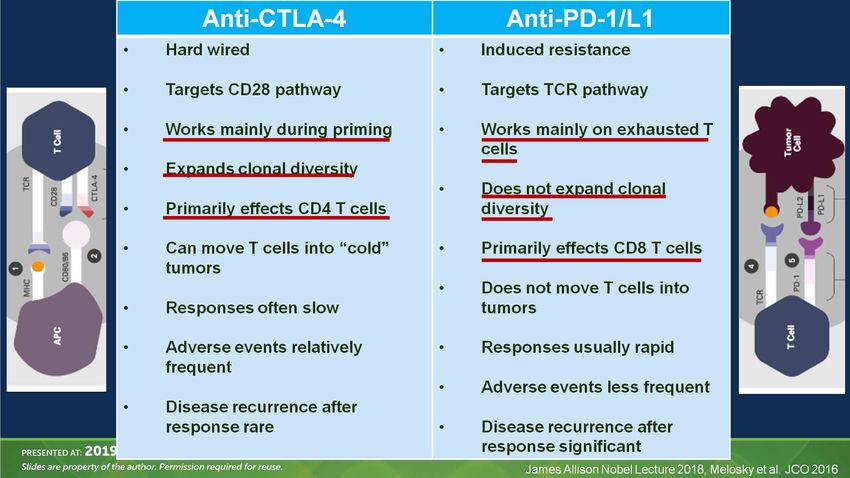
Offenlegung potentieller Interessenkonflikte
Beratungstätigkeit
Lilly, Merck, Amgen, Pierre-Fabre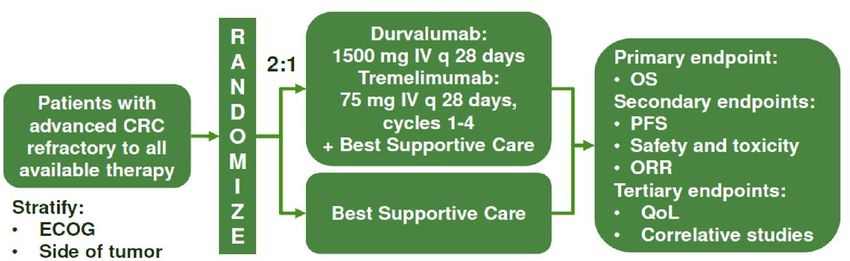
Prognostische Eckpunkte KRK • TNM Klassifikation • RAS/BRAF Mutationsstatus • Her2-Expression • MSI-H vs MSS • TMB • TIL´s • CMS
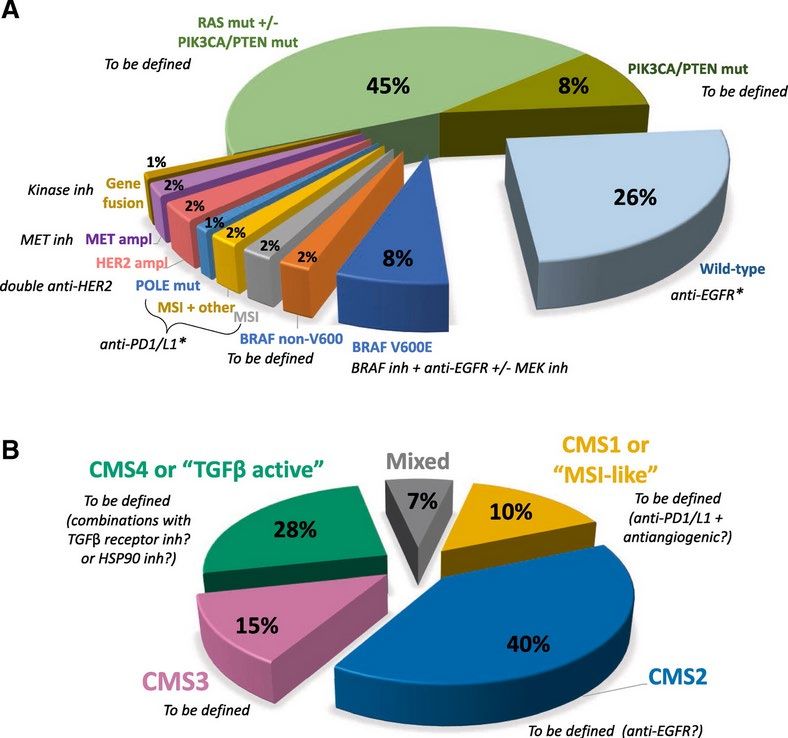
Dienstmann, R: Educational Book, ASCO 2018

Consensus molecular subtypes (CMS)
Tumor-Microenvironment als Ansatz zur Immunmodulation
Bedingt Tumorheterogenität, unterscheidet
immunogene von nicht-immunogenen Tumoren
• Tumor-infiltrierende Lymphozyten
• Zytokine
• Stroma
• Neoangiogenese /Blutgefäße
• TGF-ß
• Erhöhte Expression von CTLA-4 auf T-
Lymphozyten (Negativer Effekt auf T-
Zellaktivierung über Bindung an CD80 und CD
86 auf APC´s (Antigen-präsentierenden Zellen)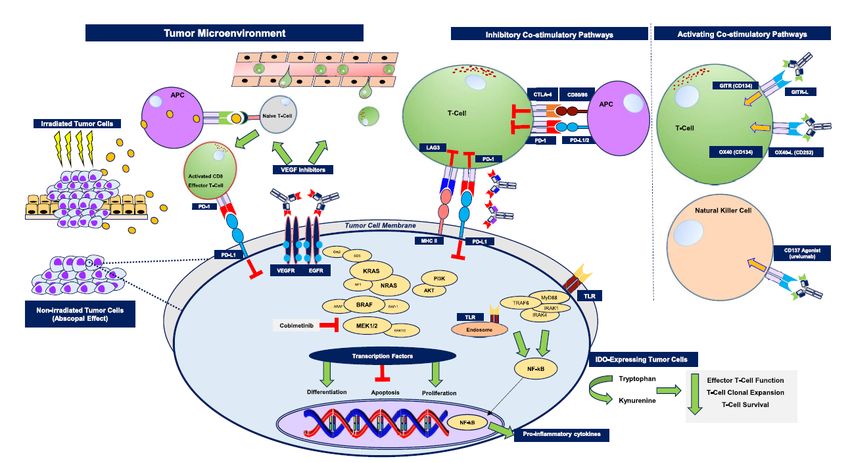
Franke et al.: JNCI 2019
Immuntherapeutische Ansätze Vakzinierungsstudien • Adjuvans • Als Erhaltungstherapie • Nach Lebermetastasenresektion PD-1/PD-L1 Immuncheckpointinhibitoren • MSI-H • als Monotherapie • in KombinationZytokine • MSS • Als Monotherapie • In Kombination Geplante Studien
Vakzinierung in der Adjuvans
Active specific immunotherapy (ASI) for stage II and stage III human colon cancer: A randomised trial.
Vermorken et al. Lancet 1999
• Autologe Tumorzell-BCG Vakzine, 3 wöchentl. Gaben und Boost nach 6 Mon.
• N= 254, St. II u. III, medianes Follow-up 5.3 Jahre
• 44%ige Risikoreduktion für Rezidiv im St.II, kein Effekt in St. III
Relapse free survival
N= 106
Turksma et al., Clin Cancer Res 2016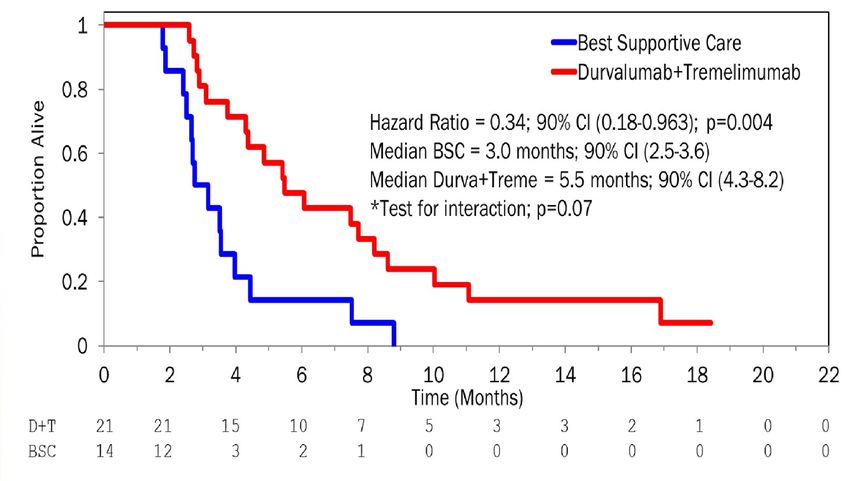
Vakzinierung nach Lebermetastasenresektion
LICC: Finale Ergebnisse
Eine randomisierte, doppelblinde, placebokontrollierte, multizentrische Phase-II-
Studie zur adjuvanten Immuntherapie mit Tecemotid (L-BLP25) nach R0/R1
Resektion von Lebermetastasen beim kolorektalen Karzinom
Carl Christoph Schimanski, Hauke Lang, Stefan Kasper, Andreas Paul, Susanna Hegewisch-Becker, Jan Schröder, Heinz-Jochen
Gassel, Friedrich Overkamp, Martin Büsing, Frank Kullmann, Karl-Heinz Dietl, Wolf Otto Bechstein, Matthias Vöhringer, Wolfgang
Steurer, Robert Öllinger, Florian Lordick, Volker Heinemann, Michael Geißler, Ludger Staib, Armin Schulz-Abelius, Bernhard Linz,
Helga Bernhard, Michael R. Schön, Richard Greil, Victoria Smith-Machnow, Irene Schmidtmann, Markus Möhler
Visceralmedizin, Wiesbaden Okt. 2019
Prof. Dr. Carl Schimanski
Viszeralmedizin 2019
KV 312
Schimanski et al., ASCO-GI 2019 und Viszeramedizin 2019Einleitung
• KRK-Patienten: 35 % Fernmetastasen bei Erstdiagnose
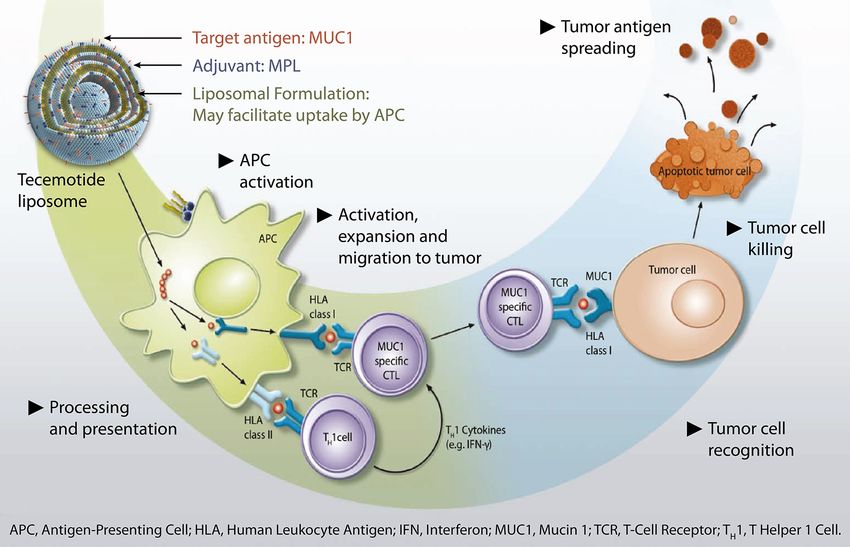
Tecemotide (L-BLP25):
• Hepatische Metastasektomie: Einzige potentiell kurative eine MUC1 Antigen-spezifische Peptid-Vakzine
Behandlung für mKRK beschränkt auf Lebermetastasen
• Hohe Rezidivrate nach Resektion: 50-75% der Patienten mit
Rezidiv innerhalb von 2 Jahren a
• Medianes Überleben:
Primär resezierte Patienten: 46 – 62 Monate b
Sekundär resezierte Patienten: 36 – 55 Monate c
Prof. Dr. Carl Schimanski
Viszeralmedizin 2019
a Folprecht et al, 2014, Annals of Oncol; Alberts et al, 2005, J Clin Oncol; Allard et al, 2017, Br J Cancer; De
Jong, 2009, Annals of Surgery
b Nordlinger et al., 2013, Lancet Oncol.; Portier et al., 2006, J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. Adjusted from Thatcher N, Heighway J. Oncologist 2010
c Folprecht et al., 2014, Annals of Oncol; Holch et al. 2018, Int. J. CancerStudiendesign
Haupteinschlußkriterien Tecemotide 930µg
Wöchentlich für 8 Wochen,
• Stadium IV KRK beschränkt
auf Lebermetastasen danach Erhaltungstherapie alle 6 Wochen für 2 Jahre a
n= 79
• Primäre oder sekundäre
Resektion (R0/R1) von Langzeit
R
Lebermetastasen (<
2:1 FU
8 Wochen vor
Randomisierung)
Placebo Liposomen
• ECOG 0 oder 1 Wöchentlich für 8 Wochen,
n=121 danach Erhaltungstherapie alle 6 Wochen für 2 Jahre b
• CHT >4 Wochen vor stratifiziert nach
Randomisierung R0/R1 n=42
a Cyclophosphamid 300 mg/m2 vor erster Immunisierung mit Tecemotide
b Kochsalzlösung vor erster Gabe von Placebo
Co-primäre Endpunkte: Sekundäre Endpunkte:
Prof. Dr. Carl Schimanski
Viszeralmedizin 2019
• Rezidivfreies Überleben • Sicherheit / Tolerabilität
• 3-Jahres Überlebensrate • MUC1 spezifisches RFS/OS
CHT: Chemotherapie; CP: Cyclophosphamid; FU: Follow Up; KRK: Kolorektales Karzinom Clinical trial information: NCT01462513
Schimanski et al, 2012, BMC CancerWirksamkeitsanalyse
Rezidivfreies Medianes RFS
100 Events Median RFS
N(%) Months (90% CI)
Proportion of patients w ithout event [%]
90
Überleben Tecemotide: 6,1 Monate
L-BLP25 + Cyclophosphamide 61 (77.2) 6.1 (5.8 - 8.8)
80 PLACEBO + Saline 28 (66.7) 11.4 (5.0 - 20.3)
+ Censored
70
60 Placebo: 11,4 Monate
50
40
30
20
10 Kein statistisch signifikanter Unterschied im RFS
0
0 6 12 18 24 30 36
zwischen beiden Behandlungsarmen
RFS [months]
Num ber at risk
L-BLP25 +
79 40 24 22 18 16 0
Cyclophosphamide
PLACEBO + Saline 42 26 18 17 14 12 0
Medianes Überleben 3-Jahres Überlebensrate
100
Gesamtüberleben
Proportion of patients w ithout event [%]
90
80
70
Tecemotide: 62,8 Monate Tecemotide: 69,1%
60 Placebo: nicht erreicht Placebo: 79,1%
50
40
30 Events Median OS
20
N(%) Months (90% CI)
Kein statistisch signifikanter Unterschied im
Prof. Dr. Carl Schimanski
L-BLP25 + Cyclophosphamide 30 (38.0) 62.8 (45.1 - NA)
10
+
PLACEBO + Saline
Censored
12 (28.6) NA (53.6 - NA)
Überleben zwischen beiden Behandlungsarmen
Viszeralmedizin 2019
0
0 6 12 18 24 30 36 42 48 54 60 66 72
OS [months]
Num ber at risk
L-BLP25 +
Cyclophosphamide
79 72 64 62 54 48 40 31 24 17 10 4 0
ABER: Unerwartet langes Überleben in beiden
PLACEBO + Saline 42 38 37 34 34 32 29 24 16 9 8 2 0 BehandlungsarmenAbhängigkeit von MUC1 Expression
Low Medium High
RFS A
100 Events Median RFS
C
100 Events Median RFS
E
100 Events Median RFS
Tecemotide + N(%) Months (90% CI) N(%) Months (90% CI) N(%) Months (90% CI)
90 Cyclophosphamide 90 90 Tecemotide +
PLACEBO + Saline Tecemotide + 17 (77.3) 5.9 (3.3 - 8.8)
Cyclophosphamide
Proportion of patients without event [%]
Proportion of patients without event [%]
Proportion of patients without event [%]
7 (63.6) 20.9 (8.5 - NA) 24 (80.0) 6.0 (3.7 - 11.4)
80 80 Cyclophosphamide 80
+ Censored
5 (100.0) 11.4 (2.3 - 17.4) PLACEBO + Saline 4 (40.0) NA (1.9 - NA)
PLACEBO + Saline 14 (77.8) 8.7 (3.6 - 21.2) +
70 70 70 Censored
+ Censored
60 60 60
50 50 50
40 40 40
30 30 30
Keine statistisch
20 20 20
10 10 10
signifikanten
0 0 0
0 6 12 18 24 30 36 0 6 12 18 24 30 36 0 6 12 18 24 30 36
RFS [months] RFS [months] RFS [months]
Unterschiede in RFS
Number at risk Number at risk Number at risk
Tecemotide + Tecemotide + Tecemotide +
11 11 7 7 5 5 0 30 13 7 6 5 3 0 22 10 7 6 5 5 0
und OS für
Cyclophosphamide Cyclophosphamide Cyclophosphamide
PLACEBO + Saline 5 3 1 0 0 0 0 PLACEBO + Saline 18 10 7 7 5 3 0 PLACEBO + Saline 10 6 6 6 5 5 0
OS B
100
D
100
F
100
verschiedene MUC1-
90 90 90
Expressionslevel.
Proportion of patients without event [%]
Proportion of patients without event [%]
Proportion of patients without event [%]
80 80 80
70 70 70
60 60 60
50 50 50
40 40 40
30 Events Median OS 30 Events Median OS 30 Events Median OS
N(%) Months (90% CI) N(%) Months (90% CI) N(%) Months (90% CI)
20 20 20
Tecemotide + Cyclophosphamide 3 (27.3) NA (30.0 - NA) Tecemotide + Cyclophosphamide 8 (26.7) 65.1 (62.8 - NA) Tecemotide +Cyclophosphamide 8 (36.4) 45.8 (36.9 - NA)
Prof. Dr. Carl Schimanski
10 PLACEBO + Saline 2 (40.0) NA (17.8 - NA) 10 PLACEBO + Saline 10
4 (22.2) NA (NA - NA) PLACEBO + Saline 3 (30.0) 53.6 (28.4 - NA)
+ Censored + Censored + Censored
0 0 0
Viszeralmedizin 2019
0 6 12 18 24 30 36 42 48 54 60 66 72 0 6 12 18 24 30 36 42 48 54 60 66 72 0 6 12 18 24 30 36 42 48 54 60 66 72
OS [months] OS [months] OS [months]
Number at risk Number at risk Number at risk
Tecemotide + Tecemotide + Tecemotide +
11 11 10 9 8 8 5 5 5 4 3 0 0 30 25 22 22 19 17 16 14 12 10 7 4 0 22 21 20 20 18 15 13 8 4 2 0 0 0
Cyclophosphamide Cyclophosphamide Cyclophosphamide
PLACEBO + Saline 5 5 5 4 4 4 3 2 1 0 0 0 0 PLACEBO + Saline 18 18 17 16 16 15 14 12 8 6 6 1 0 PLACEBO + Saline 10 7 7 7 7 6 6 5 4 2 1 0 0Schlussfolgerung
• Die LICC-Studie hat ihren primären Endpunkt nicht erreicht.
• Keine signifikante Verbesserung von RFS und OS durch die adjuvante Behandlung
mit Tecemotide.
• Es wurde kein Zusammenhang zwischen MUC1-Expression und
Behandlungsergebnis beobachtet.
• Ergebnisse der translationalen Begleitforschung sind noch ausstehend.
Prof. Dr. Carl Schimanski
Viszeralmedizin 2019Vakzinierung als Erhaltungstherapie
PD-1/PD-L1 Immuncheckpoint-Inhibitoren
PD-1 blockade in tumors with mismatch-repair Mismatch-repair deficiency predicts response
deficiency (pembrolizumab) of solid tumors to PD-1 blockade (pembrolizumab)
Le et al., N Engl J Med 2015 Le et al., Science 2017
N=86SINGE AGENT PD-1 inhibitor IN dMMR/MSI-H MCRC
Advanced/refractory disease
Setting Drug N ORR PFS rate OS rate
at 12 m at 12 m
≥2nd Nivolumab 74 31% 50% 73%
line Pembrolizumab 61 28% 34% 72%
30% 70%
Le et al. NEJM 2015; Overman et al. Lancet Onc 2017; Le et al. Science 2017Kombination von Anti-CTLA-4 (Ipilimumab) und Anti-PD-1/L1 (Nivolumab)
Slide 4
Presented By Michael Overman at 2019 Gastrointestinal Cancer SymposiumPD-1 + CTLA4 INHIBITION IN dMMR/MSI-H MCRC
(CHECKMATE 142)
1st line and refractory disease, at least 2 prior lines in 76%
Setting Drugs/Regimen N ORR PFS rate OS rate
at 12 m at 12 m
1st line Nivolumab (3) 45 60% 77% 83%
+ Ipilimumab
(1/6w)
≥2nd Nivolumab (3) 119 55% 71% 85%
line + Ipilimumab
(1/3w) 60% 85%
Overman et al JCO 2018, Lenz et al 2018
Overman et al., JCO 2018Neoadjuvant PD-1i + CTLA4i in CRC
nivolumab 3mg/kg d1, 15
ipilimumab 1mg/kg d1 no responses in pMMR/MSS
Chalabi et al ESMO 2018Neoadjuvant FOxTrot: MSI-H vs. MSS
predictiv für Ansprechen auf Chemo?
only very few regressions in dMMR/MSI-H
Seymour et al ASCO 2019ROLE OF MSI IN METASTATIC CRC (MCRC)
in the era of no immunotherapy and no BRAF
inhibition
dMMR/MSI-H better prognosis
Strongly influenced by BRAF
mutational status (BRAF mut
worse prognosis) ca. 30%
Taieb et al AnnOnc 2019Studien in der 1st line: MSI-H KRK KEYNOTE-177: Phase III (ClinicalTrials.gov NCT02563002) Rekrutierung beendet N = 308 Pembrolizumab vs. Investigators choice 1st line Finale Daten für 2021 erwartet
Studien in der Adjuvans und Neoadjuvans: in MSI-H KRK
Arm 1: mFOLFOX6 +
(Cycle 1 atezolizumab for 12
mFOLFOX6)* cycles, then atezolizumab
alone for an additional
ATOMIC Curative
resection of
Assessment
Registration and 13 cycles
NCI/ALLIANCE/AIO stage III
of dMMR
Status #
Randomization
colon cancer
|-------------------up to 10 weeks-----------------
-| Arm 2: mFOLFOX6 alone
for 12 cycles
Weitere Studien in Planung
• Adjuvant single agent PD-1/L1i od. Kombination von CTLA4i
• Neoadjuvant PD-1/L1i +/- CTLA4iThe German COLOPREDICT platform
Surgery for stage II/III colorectal
cancer in ... sites in Germany
postoperatively about 2000
preoperatively patients entered
patients per year entered into the
into the „NEO“-COLOPREDICT
COLOPREDICT platform
feeding adjuvant phase III feeding neoadjuvant phase
trials in patient subgroups II trials in patient subgroups
MSI-H/dMMR, ctDNA positive, MSI-H/dMMR, BRAF mutant
stage III (12%) stage II (10%) stage II/III (12%) stage II/III (6%)
mFOLFOX6 +/- observation +/- Binimetinib/Enc
PD-1/L1 +/-
atezolizumab chemo orafenib/Cetuxi
CTLA4
(ATOMIC) (CIRCULATE) mabMSS - niedrige Effektivität bei nicht selektionierten Patienten
Steigerung der Immunogenität durch Kombinationen der PD-1/PD-L1
Inhibitoren mit:
• Anti-VEGF-Antikörpern
• Radiatio
• MEK-Inhibitoren
• CTLA-4 Inhibitoren
• Chemotherapie
Bisher kein Durchbruch, Ergebnisse lediglich Hypothesen-
generierendMODUL trial: Biomarker driven maintenance therapy in mCRC
Grothey et al., ESMO 2018FP/Bev Atezo FP/Bev MSI 2% 1.6% MSS 98% 98.4%
Kombination von PD-L1 u. MEK-Inhibition: IMblaze370
Atezolizumab +/- Cobimentinib vs. Regorafenib
N=363, > 2 Vortherapien, 3% MSI-H
Drug N ORR (N) Responders in
MSI-H
Atezolizumab+ 183 3%(5) 2/3
Cobimentinib
Atezolizumab 90 2% (2) 1/3
Regorafenib 90 2% (2)
Eng et al., Lancet Onc 2019Phase Ib: Regorafenib+Nivolumab in MCRC (EPOC1603)
Weitere Studien mit Regorafinib 80 mg/d
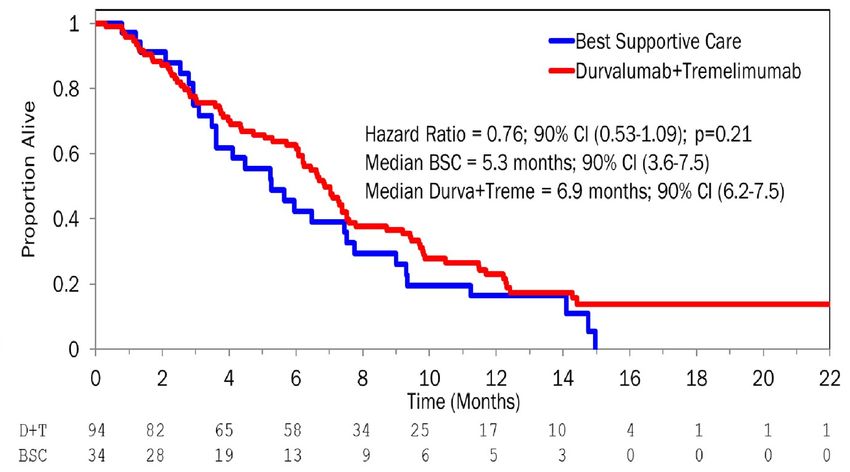
Fukuoka et al., ASCO 2019Last line mCRC: Durvalumab (PD-L1 AK) +Tremelimumab (CTLA-4 AK)
N = 180
cfDNA at trial
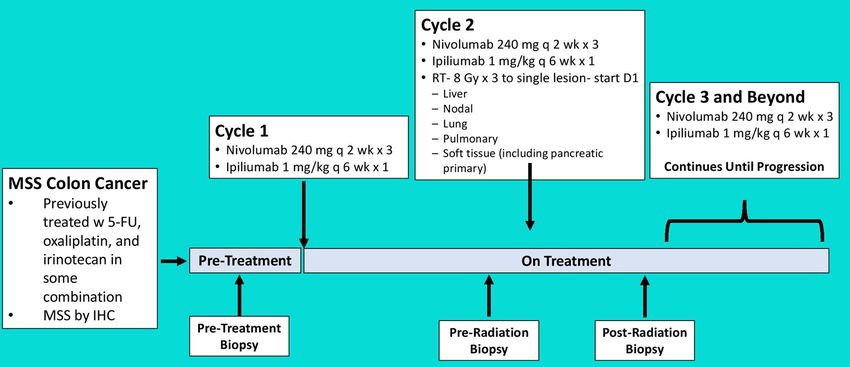
inclusion TMB>=28 TMBNivolumab+Ipilimumab+Radiotherapie
Parikh et al ASCO 2019AVETUX – Phase II (AIO-KRK-0216)
Avelumab, cetuximab and FOLFOX in 1st line MCRC
• generally feasible:
• no unexpected or additive toxicities,
besides immediate and otherwise
unexplained fever in 4 pts directly after
treatment
• only few avelumab related toxicities and
SAEsPatients characteristics (n=43) and results (n=39)
Patient characteristics Number (%)
Primary tumor location left 39 (91%)
location of metastases liver 30 (70%; 40% liver only)
microsatellite status
MSI-H/MSI-L 2/1 (5%/2%)
(local, partly central)
MSS 40 (93%)
RAS/BRAF status mutated
4 (9%)
(central tissue) (low frequent 15-30%)
Response Response rate (n) Response rate (%) ORR 79.5% and DCR 92.3%
Complete response 6/39 15.4% ETS (-20% SLD) at 8wks
Partial response 25/39 64.1% 79.5% (31/43)
(in 28 of 31 responders (CR+PR)
Stable diseae 5/39 12.8%
(90%) additional 3 pts with stable
Progressive disease 2/39 5.1% diseaseat 8 wks but >20% decrease
Not evaluable 1/39 2.6% in SLD)Discussion - results in perspective
No of RAS/BRAF Primary ORR (%) ETS >=20% mPFS
patients (%) (months)
randomized trials
OPUS 72 KRAS/BRAFwt uk 60 69.2 8.3
TAILOR 146 RASwt left sided 66.4 uk 9.2
CALGB 80405 198 RAS wt left sided (68.6)* 11.3
single arm trials
APEC 110 RASwt uk 62.7 80.6 13.3
AVETUX 43 RAS/BRAFwt 91% left 79.5 79.5 11.1
sidedTR - NGS data
Gene Target Region
AKT1 codons 10-30
APC codons 789 - 1589
B2M entire coding region
BRAF codons 582-605
CTNNB1 codons 30-46
EGFR exon 12,13,18,19,20,21
ERBB3 codons 85-105
FCGR3A codon 158
FCGR2A codon 131
HRAS codons 10-15
JAK1 entire coding region
JAK2 entire coding region
KRAS codons 10-15, 51-63, 98-150
NRAS codons 10-15, 51-63
PIK3CA codons 64-94, 316-346, 418-434, 527-560, 1002-1054
PD-L1 entire coding region
PTEN codons 71-124,130,173,267,268,320
SMAD4 entire coding region
TP53 entire coding region
26 patients with tumor mutations detectable in liquid biopsy with immediate drop during treatment
Mascha Binder, HalleTranslational Research Final results being presented at SITC 34th Annual Meeting (Society of Immunotherapy for Cancer, Nov. 6-10 2019)
FAZIT • Vakzinierungsstudien bisher in allen untersuchten Szenarien negativ • Hoher Stellenwert der Immunmodulation beim MSI KRK über alle Linien hinweg, Monotherapie oder in Kombination mit CTLA-4 Inhibitoren • Studien zur Adjuvans und Neoadjuvans laufen • Optimierung der Patientenselektion in Abhängigkeit vom TMB u. molekularem Subtyp (z.B. CMS, CMS Switch nach Anti-EGFR, TGF-ß etc.) • Stellenwert der Immunmodulation beim MSS KRK noch nicht eindeutig gezeigt
Sie können auch lesen