Mastozytose 19. März 2021 - Dr. med. Axel Rüfer, Co-Chefarzt Hämatologie, Luzerner Kantonsspital
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Zentrum für Hämatologie Mastozytose 19. März 2021 Dr. med. Axel Rüfer, axel.ruefer@luks.ch Co-Chefarzt Hämatologie, Luzerner Kantonsspital

Einleitung
Erstbeschreibung der Mastzellen durch Paul Ehrlich 1878
in seiner Dissertation an der Universität Leipzig
Verleihung Nobelpreis 1908
Differenzierung der Mastzellen aus CD34+ pluripotenten
Stammzellen – Einfluss Stem Cell Factor (SCF)
Rezeptor für SCF ist KIT = Protein mit Kinaseaktivität
Codierung durch c-KIT auf Chromosom 4 (q11-12)
Paul Ehrlich, 1854 - 1915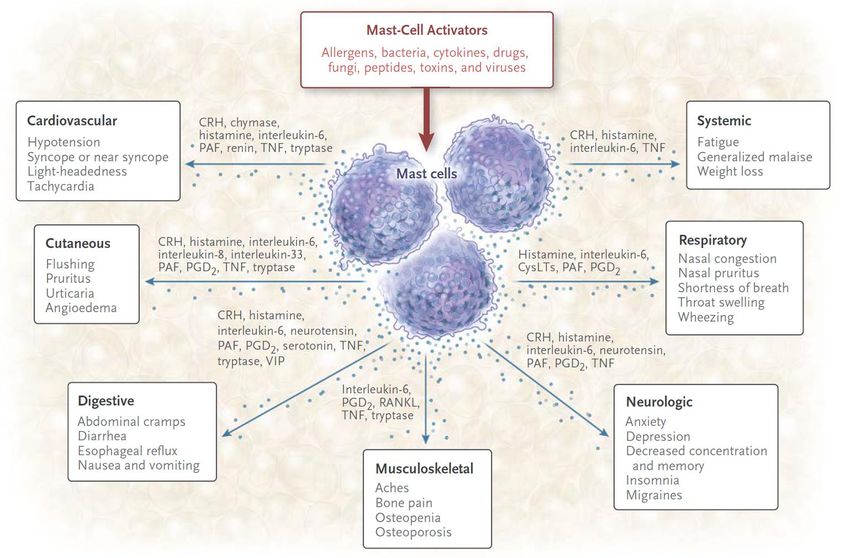
WHO-Klassifikation 2017: Mastozytose
Kutane Mastozytose
Urtikaria pigmentosa - Kinder + Erwachsene
Diffuse kutane Mastozytose - Kinder
Mastozytom der Haut - Kinder
Systemische Mastozytose (SM)
Indolente SM, ISM
Smouldering SM, SSM
SM mit assoziierter hämatologischer Neoplasie, SM-AHN
Aggressive SM, ASM
Mastzell-Leukämie, MCL
2017
Mastzell-Sarkom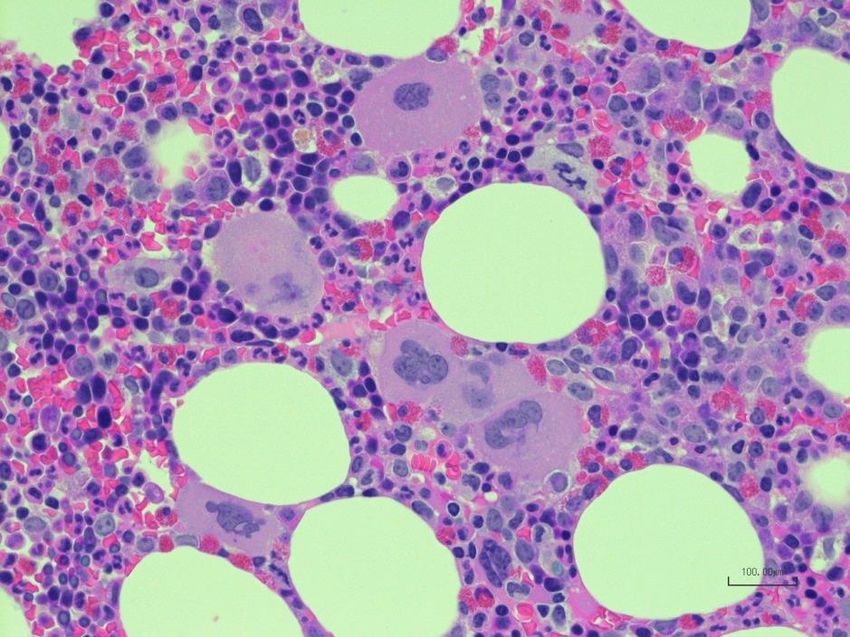
Kutane Mastozytose Ohne systemische Beteiligung Darier- Zeichen

Systemische Mastozytose Mit systemischer Beteiligung (± Haut) Knochenmark Leber und Milz Lymphknoten GI-Trakt Skelett

Systemische Mastozytose
Organbeteiligung bei 342 Patienten der Mayo Clinic
Lim K et al. Blood 2009;113:95727-36
Symptome, klinische Zeichen, Labor
Valent P. EHA 2013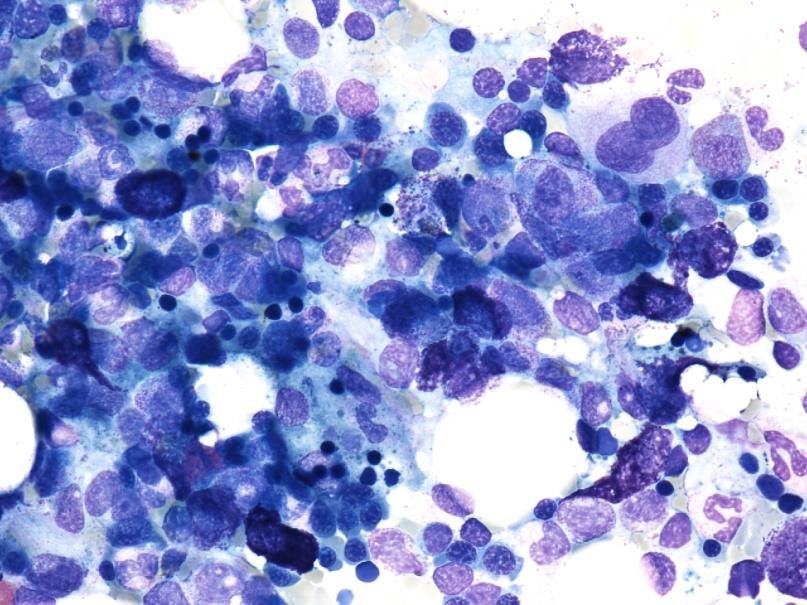
Mediatorfreisetzung
IgE vermittelt
Physikalische Reize
Chemische Reize
Zytokine
Komplement
Emotionaler Stress
Theoharides TC et al. NEJM 2015;373:163-72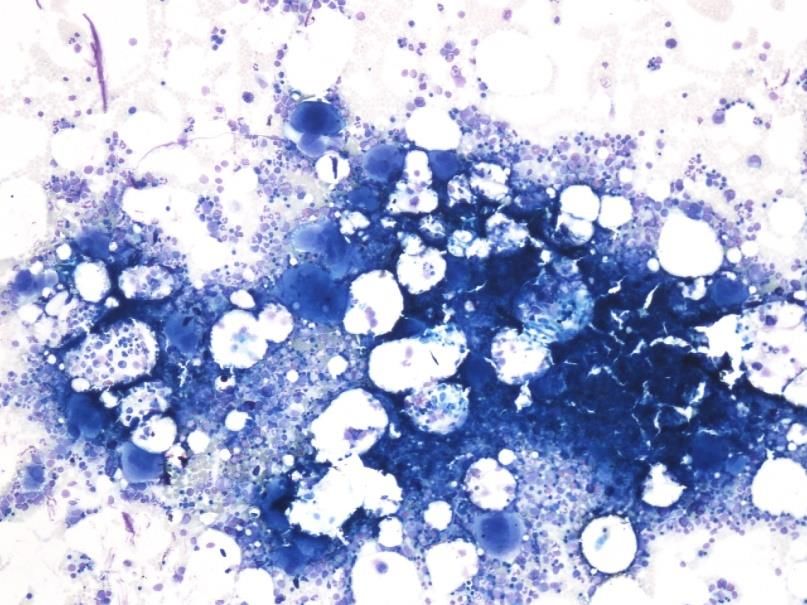
Der Weg des Patienten … … führt ihn zuerst zum Hausarzt oder zum Allergologen / Dermatologen Klassisch: Hymenopterengift-Allergie – mit lebensgefährlicher Allergiereaktion Grad III – IV (Anaphylaxie) - Biene, Wespe, Hornisse
Erste (nicht – hämatologische) Diagnostik …
… durch den Allergologen: Hautteste (in vivo),
Serologische Teste (in vitro), Provokations-Teste,
Tryptase Prävalenz allergischer
Erkrankungen =
… durch den Dermatologen: Hautbiopsie Allgemeinbevölkerung
… durch den Hausarzt: TRYPTASE (Basalkonzentration)
< 20 µg/l > 20 µg/l Anaphylaktische
Reaktionen
Systemische Ja OHNE
Symptome Hautbeteiligung –
Hämatologie
an Mastozytose
Nein denken und
TRYPTASE bestimmen
Beratung DiagnostikSerum-Tryptase Enzym, korreliert mit % der Mastzell-Infiltration Total Serum-Tryptase: Inaktive Vorstufen von α- und ß-Tryptase + aktive, reife ß-Tryptase Mastozytose / Hämatologische Neoplasien: Erhöhte Basalkonzentration – aber Normalwert schliesst Mastozytose nicht aus! Gelegentlich bei schweren Anaphylaxien nur minimal erhöht Allergische Reaktion: Peak nach 30-90 Minuten, Absinken innerhalb von 3-6 Stunden, Basalwert nach 24 Stunden
Hämatologische Diagnostik
Systemische Mastozytose?
Status (v.a. Haut). ± Tryptase. Molekulargenetik aus peripherem Blut.
Arock M et al. Leukemia. 2015;29:1223-32Hämatologische Diagnostik
Systemische Mastozytose?
Status (v.a. Haut). ± Tryptase. Molekulargenetik aus peripherem Blut.
Knochenmarkuntersuchung
Histologie:
Morphologie
Immunhistochemie
Molekulargenetik
Zytologie:
Morphologie
Immunphänotypisierung
± MolekulargenetikMajor + Minor ODER ≥ 3 Minor
Major-Kriterium
Multifokale, dichte Mastzellinfiltrate (≥ 15 Mastzellen
in Aggregaten) im Knochenmark oder anderen
extrakutanen Organen
Minor-Kriterien
> 25% der Mastzellen im Infiltrat sind spindelförmig oder haben eine atypische
Morphologie, oder, von allen Mastzellen im Aspirat sind > 25% unreif oder
morphologisch atypisch
Nachweis KIT Punktmutation am Kodon 816 (meist D816V) im Knochenmark,
Blut oder anderem extrakutanen Organ
Nachweis Expression von CD25 (sensitiverer Marker) ± CD2
Serum-Tryptase > 20 µg/lKIT Punktmutation(en)
30% bei Kindern
80% bei Erwachsenen
Arock M et al. Leukemia. 2015;29:1223-32B (burden of disease) und
C (cytoreduction-requiring) findings
B-findings
1. > 30% Mastzell-Infiltration und Tryptase > 200 µg/L
2. Zeichen von Dysplasie oder Myeloproliferation mit Blutwerten normal oder leicht
abnorm
3. Hepato-/Splenomegalie ohne Funktionseinschränkung ± LK-Vergrösserung
C-findings
1. ≥ 1 Zytopenie (ANCSystemische Mastozytose – aber welche? Indolente SM, ISM Keine C-findings, geringe Mastzell-Masse, Hautbefall Knochenmark-Mastozytose Knochenmark-Befall, kein Hautbefall Smouldering SM, SSM ≥ 2 B-findings, keine C-findings, hohe Mastzell-Masse SM mit assoziierter hämatologischer Neoplasie, SM-AHN AHN z.B. MDS, MPN, AML, Lymphom, u.a. (WHO-Entität) Aggressive SM, ASM ≥ 1 C-finding, meist kein Hautbefall
Weitere Diagnostik Systemische Mastozytose! Osteodensitometrie - nicht kassenpflichtig in CH Sonographie Abdomen: Hepato-/Splenomegalie? Aszites? LK-Vergrösserung? ÖGD / Koloskopie bei GI-Symptomen, immer mit Biopsie und immer mit CD117 - Immunhistochemie
CASE 1: Gentleman, born 1956
Referral from GP 2015:
Haematological assessment, «known Mastocytosis for years»
Present complaint:
feels ill since several months
watery diarrhoea, up to 12 times daily, since many years,
despite several endoscopies without causeCASE 1: Gentleman, born 1956 06/2011: Oesophagogastroduodenoscopy + Colonoscopy «No obvious cause for the diarrhoea found» Suggestion: PPI (not tolerated) 08/2011: Oesophagogastroduodenoscopy Refluxoesophagitis Suggestion: alternative PPI + eradication of H. pylori 01/2013: Colonoscopy Two polyps: tubular adenoma Suspicion of eosinophilic colitis with focal proliferation of eosinophils Suggestion: Budenofalk® (not tolerated), Aerius® helps
CASE 1: Gentleman, born 1956 Analysis Result Normal Leucocytes 18.0 2.6-7.8 Giga/l Myelocytes 0.27 Giga/l Metamyelocytes 0.45 Giga/l Neutrophils 13.95 0.9-5.4 Giga/l Serum-Tryptase: Eosinophils 1.08 0-0.4 Giga/l 183 µg/l (< 11.0) Haemoglobin 139 127-163 g/l MCV 89 80-97 fl MCH 30 27-34 pg MCHC 342 330-364 g/l Thrombocytes 130 130-330 Giga/l CRP
CASE 1: Gentleman, born 1956 BM-Histology: multifocal, nodular infiltrates of spindle shaped mast cells CD25-expression of mast cells Moleculargenetics: BCR-ABL1, t(9;22), JAK2 V617F, FIP1L1-PDGFRa - negative cKIT D816V - mutated Cytogenetics 46,XY[20] Flowcytometry CD25- und CD2-expression of mast cells
CASE 1: Gentleman, born 1956 Hepato- and Splenomegaly (18.4 cm diameter) Osteoporosis, no osteolytic lesions
CASE 1: Gentleman, born 1956
Pathology:
How about colon biopsies –
any evidence for mast cell infiltration?
With friendly approval by Dr. F. Aebersold Keller, LuzernCASE 1: Gentleman, born 1956
Pathology:
How about colon biopsies –
any evidence for mast cell infiltration?
Tryptase – MC always express CD117
not specific for MC,
may be absent in SM
With friendly approval by Dr. F. Aebersold Keller, LuzernCASE 1: Gentleman, born 1956
Diagnosis:
Smouldering systemic mastocytosis
B-findings: Myeloproliferation, Hepato-/Splenomegaly
GI-Infiltration with MC
Therapy:
H1-Blockade - Desloratadine
H2-Blockade - Ranitidine, since 09/2019 not available
in Switzerland, Germany, Canada, USA - Famotidine is
alternative, requires approval and import to CH 2017
Alendronate
Emergency set
Before diagnosis of eosinophilic colitis: CD117 staining has to be performedCASE 2: Gentleman, born 1967
Referral from Allergologist 2015:
Haematological assessment,
anaphylactic reactions after bee- and wasp stings
(desensibilisation since 2004)
Past Medical History:
Coronary heart disease
Myocardial infarction 2006 (aged 39 years) - DES
In-Stent Restenosis 2008
Cardiovascular RF: ?CASE 2: Gentleman, born 1967
Serum-Tryptase:
20.2 µg/l (< 11.0)CASE 2: Gentleman, born 1967
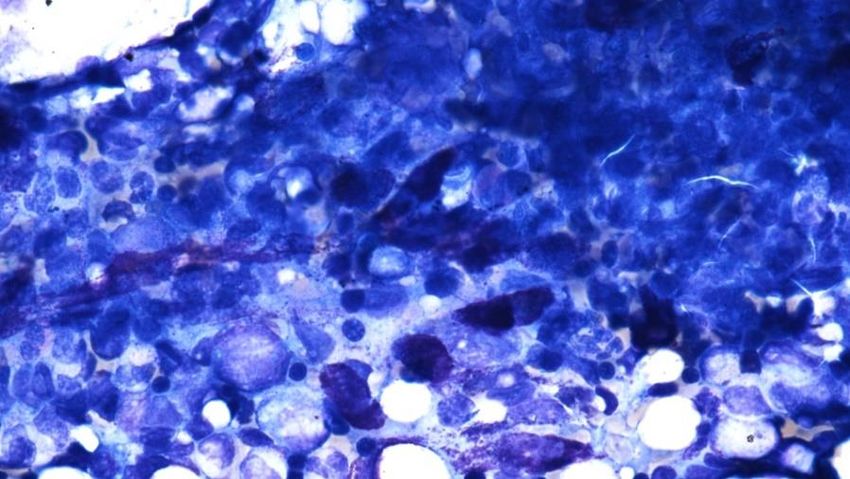
BM-Aspirate smear:
Proliferating Proliferating
and atypical, large Megakaryocytes ↑ and atypical, spindle shaped MC ↑CASE 2: Gentleman, born 1967
BM-Histology:
Tryptase ↑ c-KIT ↑
CD25 →
Cluster of
large - giant Megakaryocytes ↑
With friendly approval by Dr. C. Schürch, BernCASE 2: Gentleman, born 1967 BM-Aspirate and Histology: multifocal infiltrates of spindle shaped mast cells CD25-expression of mast cells proliferation of atypical megakaryocytes Moleculargenetics: JAK2 V617F - mutated cKIT D816V - mutated Flowcytometry CD25- und CD2-expression of mast cells
CASE 2: Gentleman, born 1967
Diagnosis:
Systemic mastocytosis with an associated
haematological neoplasm (SM-AHN)
Type of SM: Indolent SM
Type of AHN: Myeloproliferative Neoplasm (MPN) / ET
Therapy:
H1-Blockade (Desloratadine)
H2-Blockade (Famotidine)
Peginterferon alpha-2a (Pegasys®) 2017
Emergency set + lifelong desensibilisation
Thromboembolic events without cvRF and with thrombocytosis: Think of MPNTherapie (1)
ISM SSM SM-AHN ASM MCL
H1-Blockade Cladribine (Litak®, off-label)
(Desloratadine, Aerius®) Interferon-α (off-label)
H2-Blockade Hydroxyurea
(Famotidine, Pepdul®) Midostaurin (Rydapt®, TKI,
Mastzell-Stabilisatoren zugelassen für SM-AHN, ASM, MCL =
(Cromoglicinsäure, fortgeschrittene SM,
Nalcrom®) 100mg 2 x täglich
Steroide - topisch und/oder Imatinib (Glivec®, TKI,
systemisch zugelassen für ASM mit Eosinophilie und einer
(Budesonid, Budenofalk®) PDGFR -alpha oder -beta Mutation oder einem
Interferon-α (bei fehlender FIP1L1-PDGFR-alpha Fusionsprotein
Symptomkontrolle, off-label) Chemotherapie und Allogene HSCTTherapie (2) Anaphylaxie-Notfallset: 2 Tabletten Prednisolon (Spiricort®) 50mg 2 Tabletten Levoceterizin (Xyzal®) 5mg Grad III und IV: Epipen® = Adrenalin 0.3mg, Fertiginjektor, i.m. Spezifische Immuntherapie (SIT) mit Bienengift oder Wespengift (bei spezifischer Sensibilisierung) – um 90% der Patienten mit Symptombesserung, Aufdosierung: entweder 1 Tag ultra-rush oder über 12 Wochen ambulant Spital Erhaltung: danach alle 4-6 Wochen beim Hausarzt, lebenslang bei SM ± Omalizumab (Xolair®) s.c. = monoklonaler Anti-IgE-Antikörper – nur on-label bei schwerem, allergischem Asthma und chronischer spontaner Urtikaria Therapie der Osteoporose: Calcium, Vitamin D, Bisphosphonate (Aclasta®). RANK-Ligand-Inhibitor Denosumab (Prolia®, XGEVA®). Teriparatid (Forsteo®).
Prävention und Information
Vermeiden aller bekannten auslösenden Faktoren
Prämedikation vor Einsatz histaminliberierender Medikamente
(Röntgenkontrastmittel, Lokalanästhetika, Opiate, Muskelrelaxantien):
Vorabend oder 2 h vorher + evtl. 1 h vor Eingriff i.v.
Levocetirizin (Xyzal®) 1 Tab. Clemastin (Tavegyl®) 2 - 4 mg
Prednisolon (Spiricort®) 50 mg Methylprednisolon (Solu-Medrol®)
250 mg
Notfall-Ausweis, Informationsblatt
Instruktion des PatientenMastzell-Aktivierungs-Syndrom (MCAS)
Diagnose-Kriterium A:
Schwere, wiederholte (episodische) systemische (mindestens zwei
Organsysteme: kardiovaskular, respiratorisch, dermatologisch, GI)
Mastzell-Aktivierung - häufig in Form von Anaphylaxie
Diagnose-Kriterium B:
Basalkonzentration Serum-Tryptase → Plus 20% + 2 µg/l (30-120 Minuten nach Symptombeginn)
Diagnose-Kriterium C:
MCAS wenn A + B + C
Ansprechen auf H1-Blocker
Primäres = klonales MCAS:
KIT D816V + CD25-Expression, entweder mit bestätigter kutaner oder systemischer Mastozytose
(häufig) oder mit höchstens 2 Minor-Kriterien für Systemische Mastozytose
Sekundäres MCAS:
IgE-vermittelte Allergie / Hypersensitivität oder immunologische Erkrankung, welche MCA induziert
– keine Hinweise für klonale Mastzellen oder KIT D816V
Idiopathisches MCAS:
Diagnosekriterien erfüllt, aber weder primäres noch sekundäres MCAS
Valent P et al. J Allergy Clin Immunol Pract. 2019;7:1125-33Histaminintoleranz Ausschluss IgE-vermittelte Allergie Ausschluss Systemische Mastozytose (Serum-Tryptase bestimmen) Allenfalls Hautteste / OPT mit Additiva / Lebensmittelfarbstoffen Ernährungsberatung: Histaminarme Kost für 4-6 Wochen Ernährungsberatung führt zur Symptombesserung: Histaminintoleranz → allenfalls zusätzlich H1-Blocker / DAO-Ersatz (DAOSIN® [vor dem Essen] = Nahrungsergänzungsmittel mit DiAminOxidase) Ernährungsberatung führt nicht zur Symptombesserung: Keine Histaminintoleranz → Gastroenterologische Abklärung (Colon irritabile?)
European Competence Network on Mastocytosis
LUKS: Center of Excellence of ECNM
53 Patienten mit
systemischer Mastozytose
der Hämatologie LUKS
sind im ECNM registry
eingeschlossen.
Merci an Gaby Fahrni!MERCI!
Sie können auch lesen