Antimykotika - Pharmakologische Schreckgespenster?
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Antimykotika –
Pharmakologische Schreckgespenster?
Mag. pharm. Dr. Ulrike Porsche, aHPh
Landesapotheke Salzburg
Abteilung für Arzneimittelinformation
Infektiologischer Arbeitskreis
an den Salzburger Landeskliniken (SALK)
Webinar, 15. Oktober 2021
© Dr. Ulrike Porsche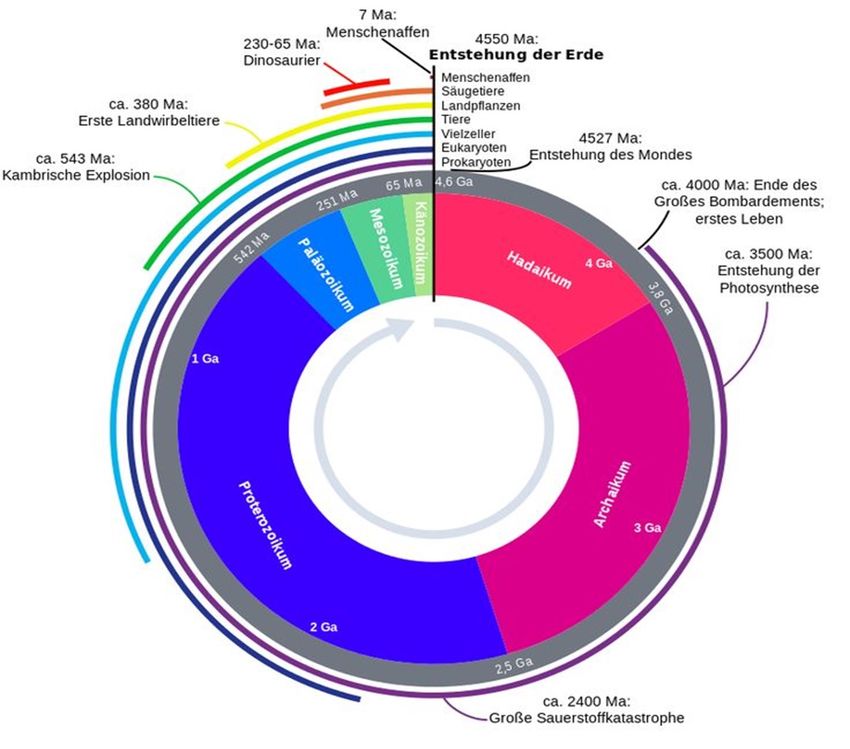
Agenda
1. Was ist ein Pilz?
2. Antimykotika - Pharmakokinetik
3. Antimykotika - Pharmakodynamik
4. Antimykotika - Dosierung
5. Antimykotika - Therapieversagen
© Dr. Ulrike Porsche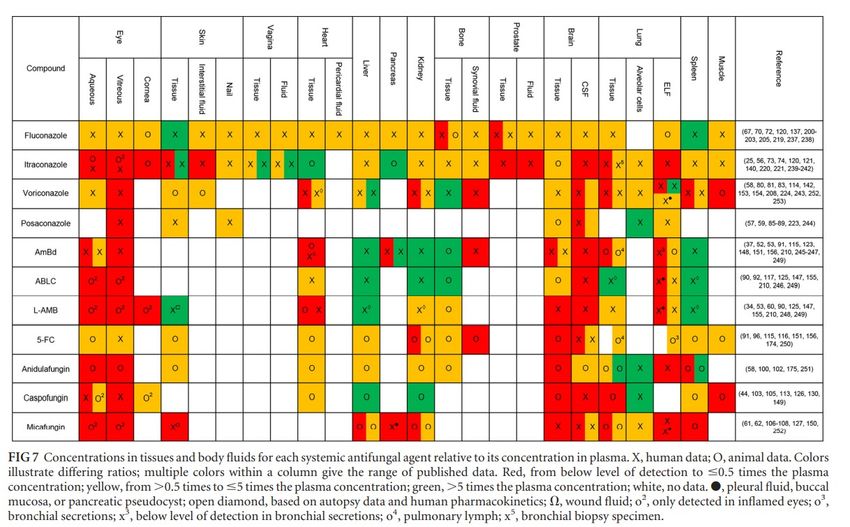
Was ist ein Pilz?
• Die Pilzzelle ist eukaryotisch. Sie weist demnach einen Zellkern auf, der
die DNA umgibt und schützt, sowie ein komplexes Membransystem und eine
innere Kompartmentierung.
• Die Zellwand der Pilze besteht unter anderem aus Chitin und Glukanen (im
Unterschied zu Pflanzen, deren Zellwand v.a. aus Zellulose besteht). Pilze
sind daher mit (mehrzelligen) Tieren näher verwandt als mit
Pflanzen.
• Ihre Plasmamembran enthält charakteristischerweise Ergosterol. Die
Ergosterolsynthese ist ein wichtiger Angriffspunkt der Antimykotika.
© Dr. Ulrike Porsche
DocCheck Flexion, Zugriff 2021-09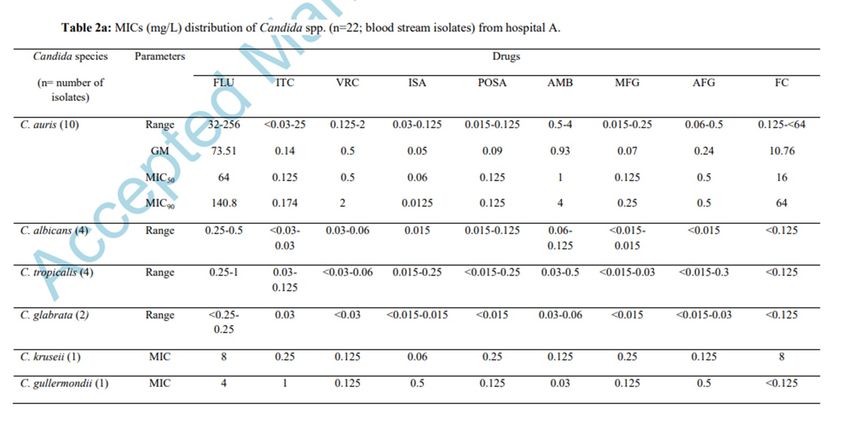
Pilzzellwand – Zusammensetzung humanpathogener Pilze © Dr. Ulrike Porsche Latgé JP et al., Annu. Rev. Microbiol. 2017, 71, 99–116.
Wie alt sind Pilze? © Dr. Ulrike Porsche
Agenda
1. Was ist ein Pilz?
2. Antimykotika - Pharmakokinetik
3. Antimykotika - Pharmakodynamik
4. Antimykotika - Dosierung
5. Antimykotika - Therapieversagen
© Dr. Ulrike Porsche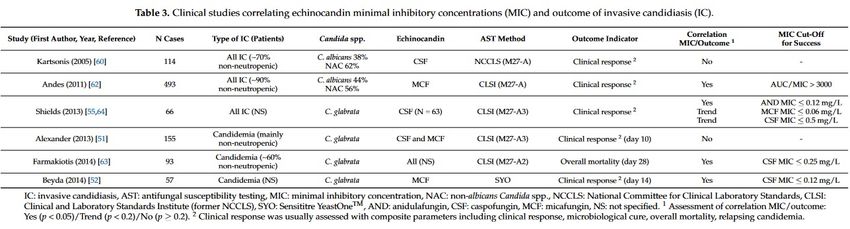
Physiochemie und Pharmakokinetik
von Antimykotika
Isavuconazole* 437 3.6 99.3 110-115 6
© Dr. Ulrike Porsche
*Langer P et al, Poster ECCMID 2017 Ergänzt nach T. Fellton et al., CMR 2014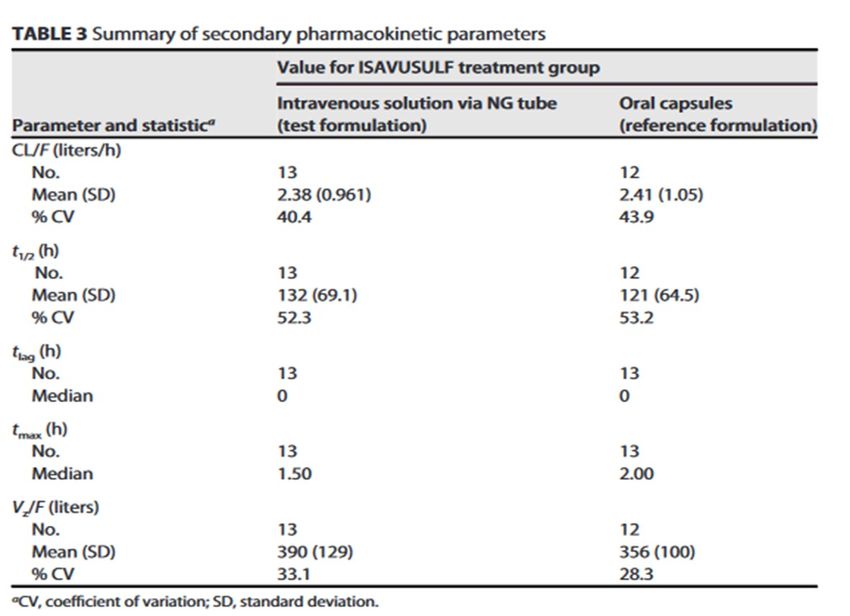
Pharmakokinetik von Azolen
im Vergleich
© Dr. Ulrike Porsche
Langer P et al, Poster ECCMID 2017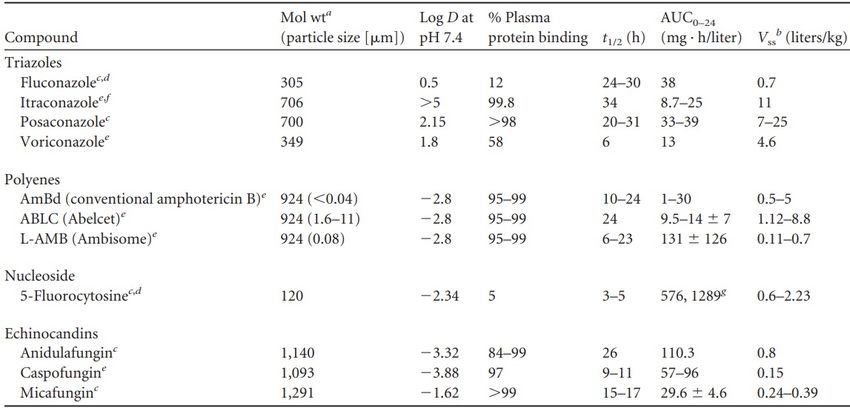
PK von Isavuconazol via Nasogastralsonde
Zubereitung + Applikation:
• 1 Amp. Cresemba® + 5 ml Aqua ad iniect.
• Applikation der gesamten Ampullenlösung
via Sonde, nachfolgende Spülung 3x mit
je 5 ml Aqua ad iniect. Die rekonstituierte
Lösung wurde unter 25°C maximal 1 h
vor der Applikation gelagert.
© Dr. Ulrike Porsche
Gesunde Freiwillige! A. Desai et al., AAC 2021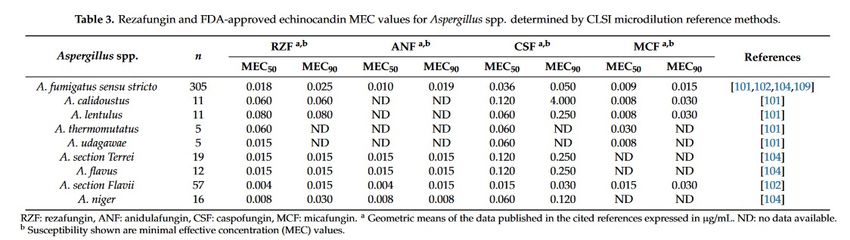
Gewebekonzentrationen von Antimykotika – Theorie (1)
• Eine Schlüssel-Determinate einer klinisch relevanten Wirksamkeit von Antimykotika ist
eine hohe Gewebepenetration.
• Die antimykotische Aktivität ist abhängig von der freien, ungebundenen
Arzneimittelkonzentration am Infektionsort (Gewebekonzentation)
• Die Gewebepenetration des Antimykotikums ist abhängig von der Membran-
permeabilität – physiochemische Eigenschaften von Pilzmitteln beeinflussen die
Permeabilität.
– Lipophilität erhöht die Permeabilität.
– Molekulargewicht und Polarität verringern sie.
• Krankheitsspezifische Änderungen der Membranphysiologie
(Infektionsgeschehen, Inflammation) können die Permaeabilität verändern.
© Dr. Ulrike Porsche
Langer P et al, Poster ECCMID 2017Gewebekonzentrationen von Antimykotika – Theorie (2)
• Zusätzliche physiologische Faktoren wie die Dichte des Endothels oder die
Aktivität von Efflux-Pumpen (P-gp mit aktiver Pumpfunktion retour ins Plasma)
können den Grad einer antimykotischen Gewebepenetration negativ beeinflussen.
• Bestimmte Gewebe (sanctuary sites wie die Gehirnregion oder die Testes)
kombinieren ein dichtes Endothel mit einer hohen Expressionsrate von
Effluxpumpen und bilden daher eine effektive Barriere gegen die Penetration von
Arzneimitteln wie Antimykotika.
Pgp aktive Effluxpumpe
Pe passive Diffusion
© Dr. Ulrike Porsche Langer P et al, Poster ECCMID 2017Antimykotika – Gewebekonzentrationen – Theorie (3)
• Kleine polare Amtimykotika mit einer niedrigen Proteinbindung
(Fluconazol, 5-FU) verteilen sich schneller in verschiedene Gewebe als
große lipophile Substanzen (Itraconazol) oder amphiphile Moleküle wie
Amphotericin B oder Echinocandine.
• Lipophile oder amphiphile Substanzen können eine längere
Verweildauer in Geweben haben und zu Konzentrationen über dem
Plasma-Niveau akkumulieren. (Postantifungaler Effekt)
Timothy Felton et al., Microbiology Reviews 2014.
© Dr. Ulrike PorscheAntimykotika –
Gewebekonzentrationen –
Praxis
5 gesunde Freiwillige! Crandon JL et al., , ANTIMICROBIAL AGENTS
© Dr. Ulrike Porsche
AND CHEMOTHERAPY, Dec. 2009, p. 5102–5107Antimykotika – Gewebekonzentrationen – Fazit 1
• Die messbare Plasmakonzentration
ist nicht automatisch ein Parameter
für die klinische Wirksamkeit (im
Gewebe).
Timothy Felton et al.,
Microbiology Reviews 2014.
© Dr. Ulrike PorscheAntimykotika – Gewebekonzentrationen – Fazit 2
• Die messbare Gewebekonzentration ist nicht automatisch ein Parameter für
die biologische Aktivität im infizierten Kompartiment. Cave Biopsie-Studien!
T. Fellton et al., CMR 2014
Mouton J et al, Journal of Antimicrobial
Chemotherapy (2008) 61, 235– 237
© Dr. Ulrike Porsche© Dr. Ulrike Porsche
T. Fellton et al., CMR 2014Agenda
1. Was ist ein Pilz?
2. Antimykotika - Pharmakokinetik
3. Antimykotika - Pharmakodynamik
4. Antimykotika - Dosierung
5. Antimykotika - Therapieversagen
© Dr. Ulrike PorschePilze in der Blutkultur 2020 BRD
https://ars.rki.de/Content/Database/
© Dr. Ulrike PorschePathogene Pilze - Antimykotika
von Lilienfeld-Toal M et al, Dtsch Arztebl Int 2019; 116: 271–78
© Dr. Ulrike PorscheWirkungsweisen von Antimykotika
Monteiro al., intechopen.87302
© Dr. Ulrike PorscheDie Pilzzellwand - ein Paradigmenwechsel Früher: inertes Exoskelett Heute: lebende, dynamische Organelle • Zusammensetzung und Lokalisation verschiedener Zellwandbestandteile in den äußeren Schichten verändern sich je nach Veränderungen der Umwelt des Pilzes • Die Erkennung der Zellwand durch den Wirt spielt für den Start der Immunantwort eine essentielle Rolle während einer Infektion (z. B. durch Aspergillus) • Tragende Rolle der Zellwand während einer Pilzinfektion © Dr. Ulrike Porsche Latgé JP et al., Annu. Rev. Microbiol. 2017, 71, 99–116.
Aspergillus fumigatus
MsbA (Aspergillus fumigatus Mucin)
zentrales Stress-Sensormolekül des
Pilzes für:
• Zellwandmorphologie
• Pilzwachstum Wikipedia, Zugriff 10/2021
• Virulenz
• Regulation der Immunantwort des Wirtes
© Dr. Ulrike PorscheA. fumigatus – Rolle von MsbA
Pilzwachstum
© Dr. Ulrike Porsche Gurgel et al. ASM mSpere 2019A. fumigatus – Rolle von MsbA
Biofilmformation
© Dr. Ulrike Porsche Gurgel et al. ASM mSpere 2019A. fumigatus – Rolle von MsbA
Immunantwort
Furthermore, beside recognition,
the mutant strain is capable of
evading killing machinery during
phagocytosis and surviving more
than the wild-type strain.
Überleben des Pilzes
© Dr. Ulrike Porsche Gurgel et al. ASM mSpere 2019A. fumigatus – Rolle von MsbA
Entzündungsmediatoren Antimykotika MIC
© Dr. Ulrike Porsche Gurgel et al. ASM mSpere 2019Agenda
1. Was ist ein Pilz?
2. Antimykotika - Pharmakokinetik
3. Antimykotika - Pharmakodynamik
4. Antimykotika - Dosierung
5. Antimykotika - Therapieversagen
© Dr. Ulrike PorschePilztherapie bei Candida albicans © Dr. Ulrike Porsche
Fluconazol – Dosierung
bei kritisch Kranken
Modell-basierte Dosierung:
Optimale loading dose: 1,450 mg
(1,250 to 1,700 mg).
Optimale Erhalungsdosis : 400 mg
(300 to 550 mg)
Dosierung lt. Guideline:
Loading dose: 800 mg
Erhaltungsdosis: 400 mg
Dosierung lt. Fachinfo (2020-12)
Invasive Candidose
Loading dose: 800 mg
Erhaltungsdosis: 400 mg
Cryptokokkose:
Bei lebensbedrohlichen Infektionen kann die
Tagesdosis auf 800 mg erhöht werden.
© Dr. Ulrike Porsche Sandaradura I et al., Antimicrob Agents Chemother March 2021Pilztherapie bei Candida glabrata © Dr. Ulrike Porsche
Caspofungin in kritisch Kranken
For Candida strains with MIC
of 0.064 mcg/ml PK/PD
targets were not attained in
all patients.
The caspofungin dose
should not be reduced in
critically ill patients in the
absence of cirrhosis, and
we advise against the use
of the C-P score in
patients with trauma- or
sepsis-induced liver
injury.
© Dr. Ulrike Porsche Kurland S. et al., AAC Juni 2019Caspofungin - Dosierung nach
KG Körpergewicht
i tt
hn
s sc
Au
Märtson AG et al., Antimicrob Agents
© Dr. Ulrike Porsche Chemother. 2020;64(9):e00905-20.Amphotericin B liposomal -
Dosierung bei Übergewicht
• For patients whose TBW exceeds 120% of their IBW, dosing LAmB by adjBW may be
reasonable in patients who are not critically ill and who have lower-risk infections.
• In critically ill patients or those with fungal pathogens or sites of infection that
are associated with higher mortality risk, dosing by TBW can be considered.
ADE: renal toxicity!
© Dr. Ulrike Porsche Ting MH et al., Antimicrob Agents Chemother. 2021 Aug 17;65(9)Anidulafungin – Dosierung
bei Übergewicht
In summary, in our internally validated PK model for obese and normal-weight subjects, weight was found
to influence both clearance and volume of distribution. This leads to lower exposure to anidulafungin
in (morbidly) obese individuals. As a consequence, a 25% increase in both the loading and maintenance
doses could be considered in patients weighing more than 140 kg.
© Dr. Ulrike Porsche
Wasmann et al., AAC 2018Micafungin – Dosierung
bei Übergewicht
When considering recent MIC distributions for C. albicans, the most frequent isolated species, our
results indicate that, to obtain adequate coverage (FTA ≥90%), the micafungin dose should be
increased to 150 mg/24 h for nonobese patients (≤115 kg) and to 200 mg/24-h for those with
body weight > 115 kg
© Dr. Ulrike Porsche Maseda et al. Critical Care (2018) 22:94Micafungin – Dosierung 1 – 2x/ Woche
… case reports demonstrate efficacy and safety of single 1400-mg
doses. Thus, a single dose of micafungin, or 2 such doses within a
few days of each other, is not only logical, but might even lead to
faster clearance of Candida.
© Dr. Ulrike PorscheRezafungin – Dosierung 1x/ Woche
• Rezafungin is much more stable in solution than the older echinocandins. This fact
is beneficial in terms of dosing flexibility and storage but also in terms of
manufacturing.
• Rezafungin is proposed as a drug to be administered once-weekly (intravenous).
• Dosing: 400 mg loading dose in Week 1, followed by 200 mg once weekly, for a
total of 2 to 4 doses.
• New forms of administration are in development such as topical and subcutaneous
forms.
Data: Cidara Therapeutics Inc. Phase III (ReSTORE),
Garcia-Effron G. Rezafungin-Mechanisms of Action, Susceptibility and Resistance: Similarities and
© Dr. Ulrike Porsche Differences with the Other Echinocandins. J Fungi (Basel). 2020 Nov 1;6(4):262Rezafungin – Therapieoption
gegen Aspergillus ssp.
Garcia-Effron G. Rezafungin-Mechanisms of Action, Susceptibility and Resistance: Similarities and Differences
© Dr. Ulrike Porsche
with the Other Echinocandins. J Fungi (Basel). 2020 Nov 1;6(4):262Azol-Hochdosistherapie
Isavuconazol
© Dr. Ulrike Porsche Cornely OA et al, AAC 2015Azol-Hochdosistherapie –
Posaconazol
Schauwvlieghe AFAD et al., Mycoses. 2020 Feb;63(2):122-130.
Adverse events of 16
patients receiving
intentionally HD-POS
Grade 3-4 AEs were observed in 6 patients, and all of them were 600 (IQR 400 750) mg
daily graded accordingly to
considered at least possibly related using Naranjo scale. the Common Terminology
Criteria for Adverse Events
10 patients had significantly higher Ctrough conc. (> 4 mg/L) and (version 4.03)
6 patients had Ctrough concentrations 3.0 - 4.0 mg/L . On the
average patients had these concentrations for a median 76 days (IQR
Reason for HD-POS:
20 162). • Vori-resistant strain
• Mucormycosis
• Salvage
• Mixed infection
• Sanctuary site infection
Naranjo adverse drug reaction probability scale: >9: definite, 5 to 8: probable,
© Dr. Ulrike Porsche 1-4: possible. −3 to 0: doubtful.Agenda
1. Was ist ein Pilz?
2. Antimykotika - Pharmakokinetik
3. Antimykotika - Pharmakodynamik
4. Antimykotika - Dosierung
5. Antimykotika - Therapieversagen
© Dr. Ulrike PorscheWenn die Therapie nicht funktioniert…
© Dr. Ulrike Porsche
Nach Lortholary, Antifungal Workshop Innsbruck 2007Therapieversagen - HOST - Neutropenie
Isavuconazole
Warn AP et al, AAC 2009
© Dr. Ulrike PorscheTherapieversagen - HOST - kritisch krank
Caspofungin – Pharmakokinetik bei kritisch Kranken
There was a relatively large interindividual variation
in the AUC0 –24 and the other PK parameters,
which is in agreement with previous studies on
caspofungin pharmacokinetics in ICU patients
© Dr. Ulrike Porsche Kurland S. et al., AAC Juni 2019Therapieversagen – HOST – kritisch krank © Dr. Ulrike Porsche Kurland S. et al., AAC Juni 2019
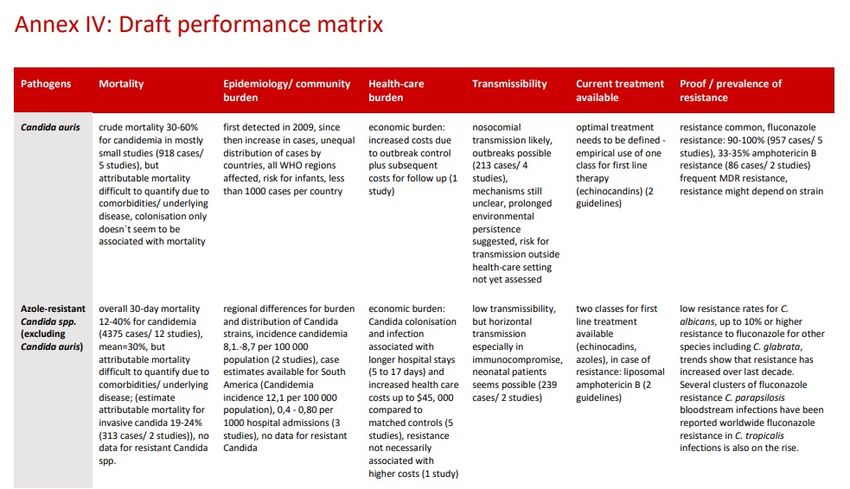
Therapieversagen – FUNGUS – resistenter Pilz © Dr. Ulrike Porsche First meeting of the WHO antifungal expert group on identifying priority fungal pathogens, Juni 2020
© Dr. Ulrike Porsche
First meeting of the WHO antifungal expert group on identifying priority fungal pathogens, Juni 2020A two-fold increase in the incidence of candidemia in COVID-19 ICUs.
MDR C. auris was the predominant species causing candidemia.
Duration of ICU stay, raised ferritin level, and tocilizumab
were independent predictors of candidemia. Highly related
strains among patients suggests nosocomial transmission.
© Dr. Ulrike Porsche
Rajni E. et al, Oxford University Press on behalf of Infectious Diseases Society of America, Sept. 2021C. auris in Europa © Dr. Ulrike Porsche Euro Surveill. 2018 Mar 29; 23(13): 18-00136
Therapieversagen – FUNGUS – PK/PD clinical breakpoints
On the clinical microbiology laboratory side:
Efforts should be pursued for more uniform practices and interpretive
criteria.
On the clinical side: Studies of MIC/outcome correlation should be
undertaken in large multicenter cohorts of relatively homogenous
patient populations, allowing for integration of potential
confounding factors in multivariate analyses.
Lamoth, F. et al, J. Fungi 2021, 7, 17.
© Dr. Ulrike PorscheTherapieversagen – FUNGUS/ ANTIFUNGAL – keine Korrelation MIC – clinical outcome © Dr. Ulrike Porsche Lamoth, F. et al, J. Fungi 2021, 7, 17.
Therapieversagen - ANTIFUNGAL – frühes versus spätes
Krankheitsstadium
Nach Hope WW et al, AAC 2010.
© Dr. Ulrike PorscheTherapieversagen – ANTIFUNGAL – pharmakogenetische
Variabilität
• 78 Patienten mit großer Voriconazol-Variabilität wurden eingeschlossen
• Nur 44.8% der Patienten erreichten Zielspiegel im Plasma von 1 und 5.5 µg/ml.
• Die Allele-Häufigkeit der *17 Variante war bei 29.5%.
• Rapid Metabolizer and Ultra rapid Metabolizer hatten niedrigere Plasmakonzentrationen
(RM/UM: 1.85 ± 0.24 µg/ml vs anderer Phenotypen: 2.36 ± 0.26 µg/ml).
• UAW waren häufig bei Patienten mit hohen Voriconazol-Spiegeln (p© Dr. Ulrike Porsche
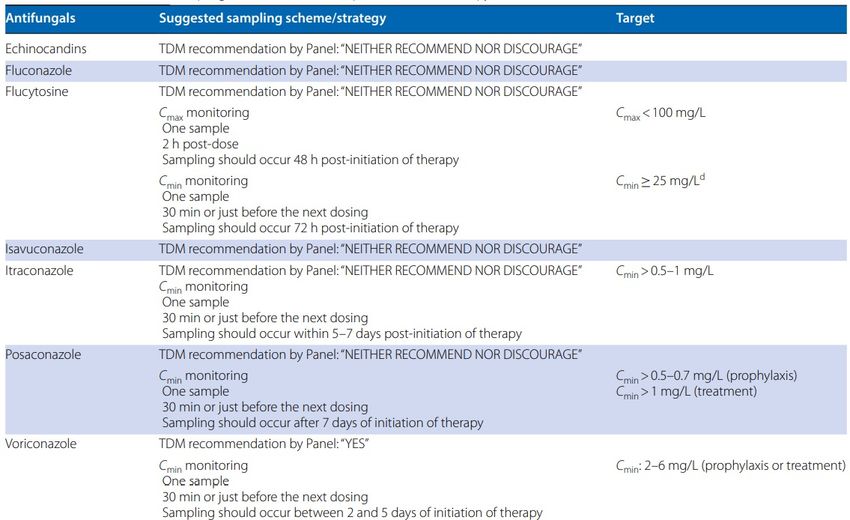
Antimykotika - TDM (1) © Dr. Ulrike Porsche Abdul-Aziz MH et al, Intensive Care Med. 2020
Antimykotika - TDM (2)
Azole - TDM in Patienten mit Covid-assoziierter pulmonaler
Aspergillose (sensibel gegenüber Voriconazol und
Posaconazol)
Wöchentliche Messung des Talspiegels (2x in der ersten Woche)
Azol-Antimykotikum Zielwerte Talspiegel
Zielwerte Talspiegel
Voriconazol 2 – 6 mg/L
Posaconazol 1 – 3,75* mg/L (*EMA-report 2014)
Isavuconazol n. a.
© Dr. Ulrike Porsche Koehler P et al, Lancet Infect Dis 2021; 21: e149–62Antimykotika - TDM (3) Azole - TDM in Patienten mit Covid-assoziierter pulmonaler Aspergillose Empfohlen bei • Eingeschränkte Nieren- oder Leberfunktion • Nierenersatzverfahren, ECMO • Übergewicht • Fragliche Arzneimittelinterkationen • Fragliche Resorption, Distribution, Metabolismus und Clearance • Hypoalbuminämie © Dr. Ulrike Porsche Koehler P et al, Lancet Infect Dis 2021; 21: e149–62
Therapieerfolg – unterstützende Maßnahmen • Adäquate diagnostische Maßnahmen + kompetente Interpretation – Glactomannan, ß-D-Glucan – Bildgebende Verfahren • Systematische Fokussuche, Suche nach Disseminationen • Cave Immunsuppression! • Adäquate antifungale Initialtherapie - Dosierung! • TDM-Einsatz, wenn sinnvoll © Dr. Ulrike Porsche Nach Lortholary, Antifungal workshop Innsbruck 2007
Sie können auch lesen