Therapieintensivierung bei Typ-2-Diabetes Wie früh ist früh genug? - Februar 2021 Christian Schelkshorn I. Medizinische Abteilung / LK ...
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Therapieintensivierung bei
Typ-2-Diabetes
Wie früh ist früh genug?
20. Februar 2021
Christian Schelkshorn
I. Medizinische Abteilung / LK Korneuburg-
Stockerau
SC-AT-02098
09.12.2020
Meine Disclosures 2021
Vorträge und Kongressunterstützung:
Boehringer Ingelheim
Lilly Pharma
Novo Nordisk
Sanofi Pharma
Novartis
AstraZeneca
MSD
GSK
Daiichi-Sankyo
Abbott Diabetes
Mylan
Advisory Board: Novo Nordisk
Boehringer Ingelheim/Eli Lilly
Sanofi Pharma
2
AstraZeneca/MSD/Abbott
Diabetes und Lebenserwartung
In Österreich
24.000 HHF/Jahr
27.000 MCI/Jahr
25.000
Strokes/Jahr
Emerging Risk Factor Collaboration, JAMA 2015
DIABETES mellitus Typ 2 –
polypragmatische Therapieansätze
gefordert
Zerebrovaskuläre
Adipositas Voranamnese
Bewegungsmangel
Niereninsuffizienz Alter Depression
Compliance/Adhärenz Kardiovaskuläre
Voranamnese
C. Schelkshorn 2021
Entscheidungskreis für patientenzentrierte
Blutzuckerkontrolle bei Typ-2-Diabetes
ERMITTLUNG ZENTRALER PATIENTENMERKMALE
• Ermittlung zentraler
Derzeitiger Lebensstil
Überarbeitung
Überarbeitung &
& Zustimmung zum
• Komorbiditäten, d. h. ASCVD, CKD, HF
Patientencharakteristika
• Klinische Merkmale, d. h. Alter, HbA1c, Gewicht
Zustimmung
Therapieplan zum • Probleme wie Motivation und Depression
• Kultureller und sozioökonomischer Hintergrund
Therapieplan
Berücksichtigung
Therapieziele spezifischer Faktoren mit
Laufende Überwachung und • Komplikationen vorbeugen
BERÜCKSICHTIGUNG SPEZIFISCHER FAKTOREN MIT AUSWIRKUNG AUF
Unterstützung • Lebensqualität optimieren Auswirkung auf die
DIE BEHANDLUNGSWAHL
• Behandlungswahl
Individualisierter HbA -Zielwert
1c
• Einfluss der Medikation auf Gewicht und Hypoglykämie
• Nebenwirkungsprofil der Medikamente
• Komplexität des Therapieplans, z. B. Häufigkeit und Art der Anwendung
• Therapiewahl mit Optimierung von Therapieadhärenz und -persistenz
• Zugang, Kosten und Verfügbarkeit von Medikamenten
Umsetzung des
Gemeinsame
Therapieplans
Entscheidungsfindung bei
der Erstellung des
Therapieplans
Zustimmung zum
Therapieplan
ASCVD, atherosclerotic cardiovascular disease, atherosklerotische kardiovaskuläre Erkrankung; CKD, chronic kidney disease, chronische Nierenerkrankung; HbA1c, glykiertes Hämoglobin; HF, heart
failure, Herzinsuffizienz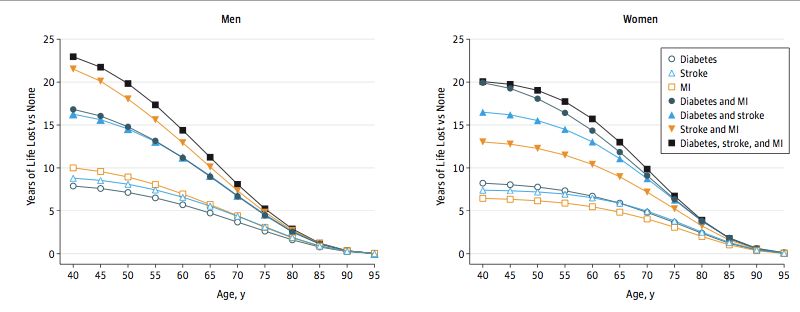
Entscheidungskreis für patientenzentrierte
Blutzuckerkontrolle bei Typ-2-Diabetes
Ermittlung zentraler
Überarbeitung
Überarbeitung &
& Zustimmung zum Patientencharakteristika
Zustimmung
Therapieplan zum
ERMITTLUNG ZENTRALER
Therapieplan
PATIENTENMERKMALE Berücksichtigung
Therapieziele spezifischer Faktoren mit
Laufende Überwachung und • Komplikationen vorbeugen
Unterstützung • Lebensqualität optimieren Auswirkung auf die
• Derzeitiger Lebensstil Behandlungswahl
• Komorbiditäten, d. h. ASCVD, CKD, HF
• Klinische
Umsetzung Merkmale,
des d. h. Alter, HbA 1c, Gewicht
Gemeinsame
Therapieplans
• Probleme wie Motivation und DepressionEntscheidungsfindung bei
der Erstellung des
• Kultureller undZustimmung
sozioökonomischer
zum
Hintergrund
Therapieplans
Therapieplan
ASCVD, atherosclerotic cardiovascular disease, atherosklerotische kardiovaskuläre Erkrankung; CKD, chronic kidney disease, chronische Nierenerkrankung; HbA1c, glykiertes Hämoglobin; HF, heart
failure, Herzinsuffizienz
Entscheidungskreis für patientenzentrierte
Blutzuckerkontrolle bei Typ-2-Diabetes
Ermittlung zentraler
Überarbeitung &
BERÜCKSICHTIGUNG
Überarbeitung & Zustimmung SPEZIFISCHER
Zustimmung zum
zum FAKTOREN MIT
Patientencharakteristika
Therapieplan
AUSWIRKUNG
TherapieplanAUF DIE BEHANDLUNGSWAHL
Berücksichtigung
• Individualisierter
Laufende Überwachung HbA
und 1c-Zielwert
• Komplikationen vorbeugen
Therapieziele spezifischer Faktoren mit
Auswirkung auf die
• Unterstützung
Einfluss der Medikation auf • Lebensqualität optimieren
Gewicht und Hypoglykämie
Behandlungswahl
• Nebenwirkungsprofil der Medikamente
• Komplexität des Therapieplans, z. B. Häufigkeit und Art der
Umsetzung des
Anwendung
Therapieplans
Gemeinsame
Entscheidungsfindung bei
• Therapiewahl mit Optimierung von Therapieadhärenz und
der Erstellung des
-persistenz Zustimmung zum
Therapieplans
• Zugang, Kosten undTherapieplan
Verfügbarkeit von Medikamenten
ASCVD, atherosclerotic cardiovascular disease, atherosklerotische kardiovaskuläre Erkrankung; CKD, chronic kidney disease, chronische Nierenerkrankung; HbA1c, glykiertes Hämoglobin; HF,
heart failure, Herzinsuffizienz
8
EASD, 17. September 2015, Stockholm Wie alles begann 1
ADA, Montag 13. Juni 2016, New Orleans Wie alles begann 2
Blutzuckersenkende Therapie
bei Diabetes mellitus Typ 2
Blutzuckersenkende Therapie bei Diabetes mellitus Typ 2
Lebensstilmodifizierende Therapie – Gewichtsmanagement, körperliche Aktivität
Metformin als Basistherapie (wenn keine Kontraindikationen)
Anamnestisch bekannte kardiovaskuläre Erkrankung oder
chronische Niereninsuffizienz
Kardiovaskuläre Erkrankung im Vordergrund Herzinsuffizienz oder chronische
Niereninsuffizienz im Vordergrund
GLP-1-Analogon mit SGLT2-Hemmer mit SGLT2-Hemmer mit Evidenz zur
kardiovaskulärem kardiovaskulärem Reduktion von Herzinsuffizienz und/oder
Benefit und/oder renalem Benefit Progression einer chronischen
Niereninsuffizienz
HbA1c über dem Zielbereich
HbA1c über dem Zielbereich
Medikament mit dokumentierter kardiovaskulärer
Sicherheit Medikament mit dokumentierter
kardiovaskulärer Sicherheit
GLP-1-Analogon, SGLT2-Hemmer
DPP-4-Hemmer falls kein GLP-1-Analogon GLP-1-Analogon
Basalinsulin DPP-4-Hemmer (nicht Saxagliptin) falls
Pioglitazon kein GLP-1-Analogon
Sulfonylharnstoff Basalinsulin, Sulfonylharnstoff
ÖDG 2019Blutzuckersenkende Therapie
bei Diabetes mellitus Typ 2
Blutzuckersenkende Therapie bei Diabetes mellitus Typ 2
Lebensstilmodifizierende Therapie – Gewichtsmanagement, körperliche Aktivität
Metformin als Basistherapie (wenn keine Kontraindikationen)
Anamnestisch bekannte kardiovaskuläre Erkrankung oder
chronische Niereninsuffizienz
Kardiovaskuläre Erkrankung im Vordergrund Herzinsuffizienz oder chronische
Niereninsuffizienz im Vordergrund
GLP-1-Analogon mit SGLT2-Hemmer mit SGLT2-Hemmer mit Evidenz zur
kardiovaskulärem kardiovaskulärem Reduktion von Herzinsuffizienz und/oder
Benefit und/oder renalem Benefit Progression einer chronischen
Niereninsuffizienz
HbA1c über dem Zielbereich
HbA1c über dem Zielbereich
Medikament mit dokumentierter kardiovaskulärer
Sicherheit Medikament mit dokumentierter
kardiovaskulärer Sicherheit
GLP-1-Analogon, SGLT2-Hemmer
DPP-4-Hemmer falls kein GLP-1-Analogon GLP-1-Analogon
Basalinsulin DPP-4-Hemmer (nicht Saxagliptin) falls
Pioglitazon kein GLP-1-Analogon
Sulfonylharnstoff Basalinsulin, Sulfonylharnstoff
ÖDG 2019Blutzuckersenkende Therapie
bei Diabetes mellitus Typ 2
Blutzuckersenkende Therapie bei Diabetes mellitus Typ 2
Lebensstilmodifizierende Therapie – Gewichtsmanagement, körperliche Aktivität
Metformin als Basistherapie (wenn keine Kontraindikationen)
Anamnestisch bekannte kardiovaskuläre Erkrankung oder
chronische Niereninsuffizienz
Kardiovaskuläre Erkrankung im Vordergrund Herzinsuffizienz oder chronische
Niereninsuffizienz im Vordergrund
GLP-1-Analogon mit SGLT2-Hemmer mit SGLT2-Hemmer mit Evidenz zur
kardiovaskulärem kardiovaskulärem Reduktion von Herzinsuffizienz und/oder
Benefit und/oder renalem Benefit Progression einer chronischen
Niereninsuffizienz
HbA1c über dem Zielbereich
HbA1c über dem Zielbereich
Medikament mit dokumentierter kardiovaskulärer
Sicherheit Medikament mit dokumentierter
kardiovaskulärer Sicherheit
GLP-1-Analogon, SGLT2-Hemmer
DPP-4-Hemmer falls kein GLP-1-Analogon GLP-1-Analogon
Basalinsulin DPP-4-Hemmer (nicht Saxagliptin) falls
Pioglitazon kein GLP-1-Analogon
Sulfonylharnstoff Basalinsulin, Sulfonylharnstoff
ÖDG 201918
19
20
21
SGLT2-I und Herzinsuffizienz Empagliflozin ist derzeit nicht zugelassen zur Therapie der Herzinsuffizienz außerhalb der Behandlung von Typ-2-Diabetes. Die behördliche Prüfung ist noch ausständig. Die Daten dienen 22 lediglich der fachlich-wissenschaftlichen Information.
Significant reduction with empagliflozin in clinically
relevant renal outcomes
39% 39% 38% 44%
p < 0.001 p < 0.001 p < 0.001 p < 0.001
New or worsening New or worsening Progression to Doubling of serum
nephropathy or nephropathy macro-albuminuria creatinine
CV death
55% 46% 0.5%
p = 0.04 p < 0.001 p = 0.25
Initiation of renal Doubling of serum New onset of albuminuria
replacement therapy creatinine, initiation of in patients with
renal replacement therapy or normo-albuminuria
death due to renal disease at baseline
Cox regression analyses in patients treated with ≥1 dose of study drug. Analyses were pre-specified except for the composite of doubling of serum
creatinine, initiation of renal replacement therapy, or death due to renal disease.
CV, cardiovascular
Christoph Wanner et al. N Engl J Med June 14, 2016, DOI: 10.1056/NEJMoa1515920McGuire DK et al. Lancet Diabetes Endocrinol 2020 Dec; 8(12): 949-959
Percentage increase in recurrent versus first events
McGuire DK et al. Lancet Diabetes Endocrinol 2020; 8: 949Overview: total (first plus recurrent) events from
EMPA-REG OUTCOME (1/2)
Empagliflozin Placebo Adjusted event
(n=4687) (n=2333) rate ratio p-value
No. of events (95% CI)
MACE outcomes
3P-MACE (primary) 585 351 0.78 (0.67, 0.91) 0.0020
4P-MACE (key secondary) 741 425 0.82 (0.71, 0.95) 0.0081
Coronary outcomes
MI 265 156 0.79 (0.62, 0.998) 0.049
Main coronary outcome 637 369 0.80 (0.67, 0.95) 0.012
Expanded coronary outcome 793 443 0.83 (0.70, 0.99) 0.033
Coronary revascularisation 372 213 0.85 (0.71, 1.03) 0.093
Admission to hospital for UA 156 74 1.03 (0.76, 1.41) 0.83
0,25 0,5 1 2
Favours empagliflozin Favours placebo
Based on post-hoc analysis. Total events were analysed by the negative binomial model. Patients were treated with ≥1 dose of study drug.
3P-MACE is composite of CV death, MI or stroke; 4P-MACE is composite of CV death, MI, stroke or admission to hospital for UA. Main coronary
outcome is MI or coronary revascularisation. Expanded coronary outcome is MI, coronary revascularisation, or unstable angina. Coronary
revascularisation is defined as coronary artery bypass graft or percutaneous coronary intervention
MACE, major adverse cardiovascular events; CV, cardiovascular; MI, myocardial infarction; UA, unstable angina.
McGuire DK et al. Lancet Diabetes Endocrinol 2020;8:949Overview: total (first plus recurrent) events from
EMPA-REG OUTCOME (2/2)
Empagliflozin Placebo Adjusted event
(n=4687) (n=2333) rate ratio p-value
No. of events (95% CI)
Cerebrovascular outcomes
Stroke 179 80 1.10 (0.82, 1.49) 0.52
TIA 44 26 0.84 (0.49, 1.44) 0.52
Stroke or TIA 223 106 1.04 (0.80, 1.36) 0.77
HF outcomes
Hospitalisation for HF 177 144 0.58 (0.42, 0.81) 0.0012
Hospitalisation for HF/CV death
333 270 0.56 (0.45, 0.69)Real World Evidence EMPRISE
EMPRISE - Objectives
Initiated and led by academic partners in collaboration with Boehringer Ingelheim
MarketScan Optum Medicare
150 million 65 million 55 million
3 large US databases people people people
Older population (65+ years)
More events expected
What will be assessed? How long is the study? How many patients?
Effectiveness, safety, healthcare First 5 years of empagliflozin 232,000 patients projected to be
resource utilisation and costs of care of use: 2014−2019 included by study completion — 116,000
empagliflozin versus DPP-4 inhibitors each in the empagliflozin and DPP-4
in patients with T2D inhibitor study arms
DPP-4, dipeptidyl peptidase-4; T2D, type 2 diabetes.
1. ClinicalTrials.gov [NCT03363464, accessed Aug 2020]. 2. Boehringer Ingelheim. Data on file, 2018.EMPRISE® study design
New users of empagliflozin
Patients with T2D
1:1 Propensity score
matching between
= patients on
empagliflozin and DPP-
4 inhibitors
New users of DPP-4 inhibitors
Key inclusion criteria*1 Key exclusion criteria*1,2
• Adults aged ≥18 years • Concomitant SGLT2 inhibitor or DPP-4 inhibitor at
• Initiation of empagliflozin or a DPP-4 inhibitor treatment initiation
between • Use of either SGLT2 inhibitor or DPP-4 inhibitor class in
August 2014 and August 2019 the 12 months preceding cohort entry (switchers)
• Patients with T2D (claims in the 12 months prior to • Patients withComprehensive clinical picture of empagliflozin
Primary outcomes Secondary outcomes
Hospital admission for MI* All-cause mortality* ESRD
Hospital admission for stroke* HHF* Treatment for retinopathy
Effectiveness1 Coronary revascularisation
CV mortality 3P-MACE
procedure
Secondary outcomes
Bone fracture Lower-limb amputation Diabetic ketoacidosis
Safety1 Urinary tract cancers† Severe hypoglycaemia‡ Acute kidney injury requiring dialysis
Inpatients HCRU Outpatients Costs
All-cause and CV hospitalisation Total cost of
All-cause ED visits Inpatient costs
care
Length of hospital stay
Office visits Outpatient costs Pharmacy costs
Healthcare
Pharmacy
resource utilisation
Medications filled Other outpatient services Emergency care costs
and costs2
* Sensitivity analyses: SGLT2i versus DPP-4i; †Bladder cancers; kidney cancers; other urinary tract, non-kidney or non-bladder cancers;
‡ Hypoglycaemia events requiring hospitalisation. 3P-MACE, 3-point major adverse cardiovascular events; CV, cardiovascular; DPP-4i,
dipeptidyl peptidase-4 inhibitor; ED, emergency department;
ESRD, end-stage renal disease; HHF, hospitalisation for heart failure; MI, myocardial infarction; SGLT2i, sodium-glucose co-transporter-2
inhibitor.
1. ClinicalTrials.gov. NCT03363464 (accessed Aug 2020); 2. EU PAS Register. EUPAS20677.
www.encepp.eu/encepp/viewResource.htm?id=21657 (accessed Oct 2018)EMPRISE year 3: interim analysis overview1
Data pooled from three Interim study population: patients aged ≥18 years
US databases11 with T2D who are new users of:1
Optum Empagliflozin DPP-4i
Cohort 1 (n=39,169)
or (n=39,169)
Clinformatics
1:1 PS-matched patients
Aug
IBM Mean follow-up: 5.8 months
MarketScan
2014–Sep
2017
Empagliflozin GLP-1 RA
Medicare Cohort 2 (n=55,860) or (n=55,860)
fee-for-service
1:1 PS-matched patients
Mean follow-up: 6.7 months
Primary and • HHF-specific*; HHF-broad†2
secondary • HHF-broad with a subsequent worsening HF event2
study • HHF-specific and HHF-broad with a 30-day readmission for any cause3
outcomes • HHF-specific and HHF-broad with a 30-day readmission for any cause or death2,3
• HHF-broad with a 90-day readmission for any cause or death2
• Atherosclerotic CV event (MI, stroke, hospitalisation for unstable angina or coronary revascularisation
procedure)1
• All-cause mortality‡4
• Safety: AKI that required dialysis, bone fracture, LLA, and hospitalisation for DKA4
Of the outcomes, only HHF-specific, HHF-broad and atherosclerotic CV event are available for the empagliflozin vs GLP-1 RA cohort
*Defined as a discharge diagnosis of HF in the primary position (positive predictive value = 84–100%); †Defined as a discharge diagnosis of HF in any
position (positive predictive value = 79–96%); ‡Medicare only
CV, cardiovascular; DKA, diabetic ketoacidosis; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist;
HF, heart failure; HHF, hospitalisation for heart failure; MI, myocardial infarction; LLA, lower limb amputation; PS, propensity score; T2D, type 2 diabetes
1. Patorno E et al. AHA 2019; oral presentation 17 Nov 2019 ; 2. Patorno E et al. HFA Discoveries 2020 abstract 1761;
3. Najafzadeh M et al. AMCP 2020, poster; 4. Patorno E et al. ADA 2020; abstract 134-LB:Selected patient characteristics in the propensity
score-matched population
Cohort 1 Cohort 2
DPP-4i Empagliflozin GLP-1-RA Empagliflozin
(n=39,169) (n=39,169) (n=55,860) (n=55,860)
Age, years, mean ± SD 60.28 ± 9.19 60.25 ± 9.06 60.66 ± 9.24 60.82 ± 8.99
Gender, male 21,407 (54.7) 21,416 (54.7) 30,622 (54.8) 30,574 (54.7)
Cardiovascular disease history 10,895 (27.8) 10,968 (28.0) 15,649 (28.0) 15,687 (28.1)
Ischaemic heart disease 8259 (21.1) 8241 (21.0) 11,593 (20.8) 11,664 (20.9)
Stroke 2396 (6.1) 2428 (6.2) 3556 (6.4) 3538 (6.3)
Heart failure 2482 (6.3) 2461 (6.3) 3353 (6.0) 3381 (6.1)
Peripheral arterial disease 2295 (5.9) 2316 (5.9) 3539 (6.3) 3517 (6.3)
Chronic kidney disease 3394 (8.7) 3321 (8.5) 5074 (9.1) 4887 (8.7)
No. of diabetes medications, mean ± SD 2.23 ± 0.84 2.24 ± 0.90 2.48 ± 1.00 2.46 ± 0.98
Current use of metformin 23,998 (61.3) 24,244 (61.9) 34,750 (62.2) 34,682 (62.1)
Current use of insulin 6794 (17.3) 6933 (17.7) 8762 (15.7) 8603 (15.4)
HbA1c,* %, mean ± SD 8.52 ± 1.82 8.46 (1.76) 8.57 (1.82) 8.51 (1.73)
Creatinine,* mg/dl, mean ± SD 0.92 ± 0.30 0.89 ± 0.23 0.92 ± 0.28 0.89 ± 0.23
Data are n (%) unless specified otherwise. *Values available in approximately 20% of the population
Patient characteristics were measured during the 12 months (365 days) preceding (and including) date of dispensing
DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycated haemoglobin;
33
1. Patorno E et al. AHA 2019; oral presentation 17 Nov 2019; 2. Patorno E et al. ADA 2020; abstract 134-LBEmpagliflozin is associated with a decreased risk of HHF and
similar risk of atherosclerotic CV events compared with DPP-4i
Empagliflozin DPP-4i
(n=39,169) (n=39,169)
n IR/ n IR/
event 1000 PY event 1000 PY HR (95% CI)
HHF-specific* 56 2.92 131 7.43 0.42 (0.31, 0.58)
HHF-broad† 272 14.24 447 25.48 0.59 (0.51, 0.69)
Atherosclerotic CV event‡ 278 14.56 305 17.6 0.88 (0.74, 1.03)
0,25 0,5 1 2
Favours Favours
empagliflozin DPP-4i
Year 3 data. Estimated HR and 95% CI adjusting for >140 baseline covariates
*Defined as a discharge diagnosis of HF in the primary position (positive predictive value = 84–100%);
†Defined as a discharge diagnosis of HF in any position (positive predictive value = 79–96%);
‡Defined as a composite of myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation procedure
CV, cardiovascular; DPP-4i, dipeptidyl peptidase-4 inhibitor; HF, heart failure; HHF, hospitalisation for heart failure; IR, incidence rate; PY, patient-
year
1. Patorno E et al. AHA 2019; oral presentation. 17 Nov 2019; 2. Patorno E et al. ADA 2020; abstract 134-LB
34Empagliflozin is associated with a decreased risk of ACM and a similar
risk of atherosclerotic CV events compared with DPP-4i
Empagliflozin DPP-4i
(n=39,169) (n=39,169)
n IR/ n IR/
HR (95% CI)
event 1000 PY event 1000 PY
All-cause mortality*2 42 8.3 83 15.9 0.52 (0.36, 0.76)
Atherosclerotic CV event†1 278 14.56 305 17.6 0.88 (0.74, 1.03)
MI1 128 6.69 133 7.54 0.93 (0.73, 1.19)
Stroke1 83 4.33 95 5.39 0.84 (0.63, 1.14)
MI or stroke2 192 10.0 209 11.9 0.89 (0.73, 1.09)
Unstable angina1 27 1.41 36 2.04 0.71 (0.41, 1.20)
Coronary revascularisation1 145 7.59 157 8.91 0.87 (0.69, 1.09)
0,25 0,5 1 2
Favours Favours
empagliflozin DPP-4i
Year 3 data. Estimated HR and 95% CI adjusting for >140 baseline covariates
*Medicare only; †Defined as a composite of myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation
procedure; ACM, all-cause mortality; CV, cardiovascular; DPP-4i, dipeptidyl peptidase-4 inhibitor; IR, incidence rate; MI, myocardial infarction;
PY, patient-year
1. Patorno E et al. AHA 2019; oral presentation 17 Nov 2019 ; 2. Patorno E et al. ADA 2020; abstract 134-LBEmpagliflozin is associated with a decreased risk of ACM and a similar
risk of atherosclerotic CV events compared with DPP-4i
Empagliflozin DPP-4i
(n=39,169) (n=39,169)
n IR/ n IR/
HR (95% CI)
event 1000 PY event 1000 PY
All-cause mortality*2 42 8.3 83 15.9 0.52 (0.36, 0.76)
Atherosclerotic CV event†1 278 14.56 305 17.6 0.88 (0.74, 1.03)
MI1 128 6.69 133 7.54 0.93 (0.73, 1.19)
Stroke1 83 4.33 95 5.39 0.84 (0.63, 1.14)
MI or stroke2 192 10.0 209 11.9 0.89 (0.73, 1.09)
Unstable angina1 27 1.41 36 2.04 0.71 (0.41, 1.20)
Coronary revascularisation1 145 7.59 157 8.91 0.87 (0.69, 1.09)
0,25 0,5 1 2
Favours Favours
empagliflozin DPP-4i
Year 3 data. Estimated HR and 95% CI adjusting for >140 baseline covariates
*Medicare only; †Defined as a composite of myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation
procedure; ACM, all-cause mortality; CV, cardiovascular; DPP-4i, dipeptidyl peptidase-4 inhibitor; IR, incidence rate; MI, myocardial infarction;
PY, patient-year
1. Patorno E et al. AHA 2019; oral presentation 17 Nov 2019 ; 2. Patorno E et al. ADA 2020; abstract 134-LBEmpagliflozin is associated with a decreased risk of HHF and
similar risk of atherosclerotic CV events compared with GLP-1 RA
Empagliflozin GLP-1 RA
(n=55,860) (n=55,860)
n IR/ n IR/
HR (95% CI)
event 1000 PY event 1000 PY
HHF-specific* 113 3.49 160 5.70 0.63 (0.49, 0.80)
HHF-broad† 510 15.79 557 19.92 0.83 (0.74, 0.93)
Atherosclerotic CV event‡ 458 14.19 413 14.76 0.99 (0.87, 1.13)
Myocardial infarction 224 6.92 193 6.88 1.03 (0.85, 1.25)
Stroke 131 4.04 100 3.56 1.18 (0.90, 1.53)
Unstable angina 45 1.39 51 1.81 0.77 (0.52, 1.16)
Coronary
225 6.96 215 7.67 0.92 (0.76, 1.11)
revascularisation
0,25 0,5 1 2
Favours Favours
empagliflozin GLP-1 RA
Year 3 data. Estimated HR and 95% CI adjusting for >140 baseline covariates
* Defined as a discharge diagnosis of HF in the primary position (positive predictive value = 84–100%);
† Defined as a discharge diagnosis of HF in any position (positive predictive value = 79–96%);
‡ Defined as a composite of myocardial infarction, stroke, hospitalisation for unstable angina, or coronary revascularisation procedure
CV, cardiovascular; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HF, heart failure; HHF, hospitalisation for heart failure; IR, incidence rate;
PY, patient-year
Patorno E et al. AHA 2019, oral presentation 17 Nov 2019Empagliflozin is associated with a decreased risk of HHF and MACE
compared with DPP-4i in older adults*
Empagliflozin DPP-4i
(n=11,579) (n=11,579)
n IR/ n IR/
event 1000 PY event 1000 PY HR (95% CI)
HHF-specific† 38 7.57 91 17.53 0.43 (0.30, 0.63)
HHF-broad‡ 165 33.03 296 57.59 0.57 (0.47, 0.69)
Modified MACE§ 122 24.32 199 38.38 0.63 (0.50, 0.79)
Myocardial infarction 48 9.56 70 13.46 0.71 (0.49, 1.03)
Stroke 37 7.36 60 11.53 0.64 (0.42, 0.96)
ACM 42 8.34 83 15.91 0.52 (0.36, 0.76)
Sensitivity analyses for competing risks
HHF-specific† or ACM 80 15.95 143 27.15 0.59 (0.45, 0.77)
HHF-broad‡ or ACM 201 40.28 334 64.14 0.63 (0.53, 0.75)
Myocardial infarction or ACM 87 17.35 128 24.24 0.71 (0.54, 0.94)
Stroke or ACM 79 15.73 111 21.03 0.75 (0.56, 1.00)
0,25 0,5 1 2
Favours Favours
empagliflozin DPP-4i
Year 3 data. Estimated HR and 95% CI adjusting for >140 baseline covariates
* Patients ≥66 years, Medicare only; †Defined as a discharge diagnosis of HF in the primary position (positive predictive value = 84–100%);
‡ Defined as a discharge diagnosis of HF in any position (positive predictive value = 79–96%); §Defined as a composite of myocardial infarction,
stroke or ACM
ACM, all-cause mortality; CV, cardiovascular; DPP-4i, dipeptidyl peptidase-4 inhibitor; HF, heart failure; HHF, hospitalisation for heart failure;
IR, incidence rate; MACE, major adverse cardiovascular events; PY, patient-year
Patorno E et al. ADA 2020, abstract 133-LBEmpagliflozin is associated with a decreased risk of AKI, an increased
risk of DKA and a similar risk of LLA and fractures compared with DPP-4i
Empagliflozin DPP-4i
(n=39,169) (n=39,169) HR (95% CI)
n events (IR/1000 PY)
AKI that required dialysis 170 (8.9) 271 (15.5) 0.64 (0.53, 0.77)
LLA 55 (2.9) 53 (3.0) 0.97 (0.67, 1.42)
Bone fracture 55 (2.9) 43 (2.4) 1.21 (0.81, 1.81)
Hospitalisation for DKA 52 (2.7) 31 (1.8) 1.56 (1.00, 2.44)
0,25 0,5 1 2 4
Favours empagliflozin Favours DPP-4i
Year 3 data
AKI, acute kidney injury; DKA, diabetic ketoacidosis; DPP-4i, dipeptidyl peptidase-4 inhibitor; IR, incidence rate; LLA, lower limb amputation;
PY, patient-years
Patorno E et al. ADA 2020, abstract 134-LBEMPRISE: interim analysis overview
Data pooled from Overall population of patients aged
two US databases ≥18 years with T2D who are new users of:
Empagliflozin or DPP-4i
Optum (n=22,811) (n=22,811)
Clinformatics
1:1 PS-matched patients
Aug 2014–
Sep 2017
IBM
MarketScan Patients with CVD Patients without CVD
• 3413 1:1 PS-matched pairs • 19,277 1:1 PS-matched pairs
• Mean follow-up: 6.1 months • Mean follow-up: 6.2 months
Utilisation • Risk of first all-cause hospitalisation • Number of office visits
outcomes • Number of all-cause hospital admissions • In-hospital days
• Risk of first emergency department visit
• Number of emergency department visits
Year 3 data
CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; PS, propensity score; T2D, type 2 diabetes
Najafzadeh M et al. AHA 2019, poster 13655The effect of empagliflozin vs DPP-4i on HHF was consistent in patients
with and without CVD
Empagliflozin Comparator
n event/ n event/
N analysed Rate/ N analysed Rate/ HR (95%
Study (%) 1000 PY (%) 1000 PY CI)
EMPA-REG OUTCOME® 1 126/4687 95/2333 0.65
9.4 14.5
Empagliflozin vs placebo (2.7) (4.1) (0.50, 0.85)
EMPRISE2
Empagliflozin vs DPP-4i
82/17,551 146/17,551 0.56
Broad HHF 10.3 19.6
(N/R) (N/R) (0.43, 0.73)
17/13,238 36/13,238 0.46
Without CVD 2.8 6.3
(N/R) (N/R) (0.26, 0.83)
64/4245 115/4245 0.56
With CVD 35.4 65.0
(N/R) (N/R) (0.41, 0.76)
0,25 Favours
1 Favours
4
empagliflozin comparator
Year 2 data
Comparison of studies should be interpreted with caution due to differences in study design, populations and methodology. Definitions of
HHF vary between studies.
CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; HHF, hospitalisation for heart failure; N/R, not reported; PY, patient-
years
1. Zinman B et al. N Engl J Med 2015; 373: 2117; 2. Patorno E et al. Circulation 2019; 139: 2822-2830Empagliflozin is associated with a lower risk of all-cause hospitalisations
versus DPP-4i
Empagliflozin DPP-4i
First event n IR/1000 n IR/1000
events PY events PY HR (95% CI)
Risk of first all-cause 0.80
805 68.0 906 85.7
hospitalisation (0.73, 0.88)
0.78
With baseline CVD 227 131.8 267 170.6
(0.66, 0.94)
0.83
Without baseline CVD 570 56.6 623 69.2
(0.74, 0.93)
0,5 1 2
Favours empagliflozin Favours DPP-4i
Empagliflozin DPP-4i
Recurrent events Incidence rate
PMPY ratio (95% CI)
Risk of all-cause
0.08 0.10 0.80 (0.73, 0.87)
hospital admissions
With baseline CVD 0.16 0.20 0.82 (0.70, 0.96)
Without baseline CVD 0.06 0.08 0.81 (0.73, 0.90)
0,5 1 2
Favours empagliflozin Favours DPP-4i
Year 3 data
CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; IR, incidence rate;
PMPY, per member per year; PY, patient-years
Najafzadeh M et al. AHA 2019, poster 13655CV death over time
Cumulative incidence.
Cox regression analyses in patients treated with ≥1 dose of study drug
Fitchett D et al. J Am Coll Cardiol. DOI: 10.1016/j.jacc.2017.11.022
43Diabetes-related complications in the USA, 1990-2010 Acute myocardial infarction Adapted from Gregg EW, et al. N Engl J Med 2014;370:1514–1523. Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.
Take-Home-Message
Herausforderungen
▪ Renale und CV Thematik muss früh in die Therapieentscheidung
eingebunden werden. AKTIVES UMSTELLEN bei Auftreten von
RISIKOFAKTOREN – auch bei guter BZ Stoffwechsellage
▪ Das NW Profil und die Hypoglykämiereduktion werden die
Therapieadhärenz unserer Patienten entscheidend mitbeeinflussen und
somit den Therapieerfolg, daher ist Schulung von elementarer Bedeutung.
▪ Zeitgerechte Therapie-Intensivierung – bessere Langzeitergebnisse –
„metabolic memory“
▪ Überwindung der Hemmschwelle zur „injektable“ Therapie
▪ Die Begleitung/Betreuung der Diabetespatienten muss polypragmatisch
erfolgen.
▪ Nur einen Aspekt (z. B. BZ) im Fokus zu haben, führt zu keiner
ausreichenden Verbesserung des Outcomes. Christian Schelkshorn 2021Sie können auch lesen