Asthma bronchiale Dr. med. Andreas Jung - Oberarzt Pneumologie Kinderspital Zürich Universitätskinderkliniken
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
Asthma bronchiale Dr. med. Andreas Jung Oberarzt Pneumologie Kinderspital Zürich Universitätskinderkliniken

Themen
– Lungenfunktion
– Asthmatherapie
– Schweres Asthma
– Inhalationstherapie
2
Erhalt einer normalen Lungenfunktion ist wichtig!
Baraldi et al. , NEJM 2007
Lungenfunktionstests – Spirometrie – Bodyplethysmographie – FeNO – Belastungslungenfunktion (EIA-Test) – Methacholinprovokation – Spezielle Tests (MBW/LCI, nasals NO, FOT, DLCO)
Wer misst, misst Mist! (und übersieht ggfs. Relevantes…)
Erfolgsfaktoren bei Kindern – Erklärung / Demonstration – Motivation / Anfeuerung – Incentives / visuelles Feedback – Übung / Wiederholung – Zeit / Geduld
NICE Guideline 2017

(normal

Und bei den Vorschulkindern? Anamnese, Symptome, FeNO, Nachweis der BHR
Messung der bronchialen Hyperreagibilität
Belastungslungenfunktion: Asthma-Beweis
100
80
-15%
FEV1
60
40
20
Belastung
5 10 15 20 25 30
MinutenMessung der bronchialen Hyperreagibilität Methacholinprovokation: Asthma-Ausschluss
Nachweis der Atemwegsentzündung
Exhaliertes NO (FeNO): Atopische Atemwegs-Inflammation
NIOX Vario
(Aerocrine)
CLD 88 sp analyzer
(EcoMedics)
NIOX MINO
(Aerocrine)Nachweis der Atemwegsentzündung Exhaliertes NO: Norm bis 20 ppb
Nachweis der Atemwegsentzündung Exhaliertes NO: “offline” (bag) Methode: Norm
Nachweis der Atemwegsentzündung
Exhaliertes NO: offline Methode (Kleinkinder)
Singer F. & Moeller A., Allergy 2013;68:531Asthmatherapie: Behandlungsziele - Reduzierung von Häufigkeit und Schwere akuter Exazerbationen - Erreichen und Erhalten einer kompletten Symptomkontrolle - Ermöglichen einer normalen Aktivität und körperlichen Belastbarkeit - Erreichen und Erhalt einer normalen Lungenfunktion - Prävention bleibender Schäden - Verhindern von Asthma-Todesfällen - Verhütung von Nebenwirkung der Asthma-Behandlung
Asthmatherapie
Ziel: Symptomkontrolle
NVL Asthma, AWMF 2018Therapie: Vorschulkinder ≤ 5 Jahre
Behandlungsplan n. GINA (2018)
STEP 4
PREFERRED STEP 3
STEP 1 STEP 2 Continue
CONTROLLER
CHOICE controller
Double & refer for
‘low dose’ specialist
Daily low dose ICS ICS assessment
Other Leukotriene receptor antagonist (LTRA) Low dose ICS + LTRA Add LTRA
controller Inc. ICS
Intermittent ICS frequency
options Add intermitt
ICS
RELIEVER As-needed short-acting beta2-agonist (all children)
CONSIDER Infrequent Symptom pattern consistent with asthma Asthma diagnosis, and Not well-
THIS STEP FOR viral wheezing and asthma symptoms not well-controlled, or not well-controlled on controlled
CHILDREN and no or ≥3 exacerbations per year low dose ICS on double
WITH: few interval ICS
Symptom pattern not consistent with asthma but
symptoms First check diagnosis, inhaler skills,
wheezing episodes occur frequently, e.g. every
6–8 weeks. adherence, exposures
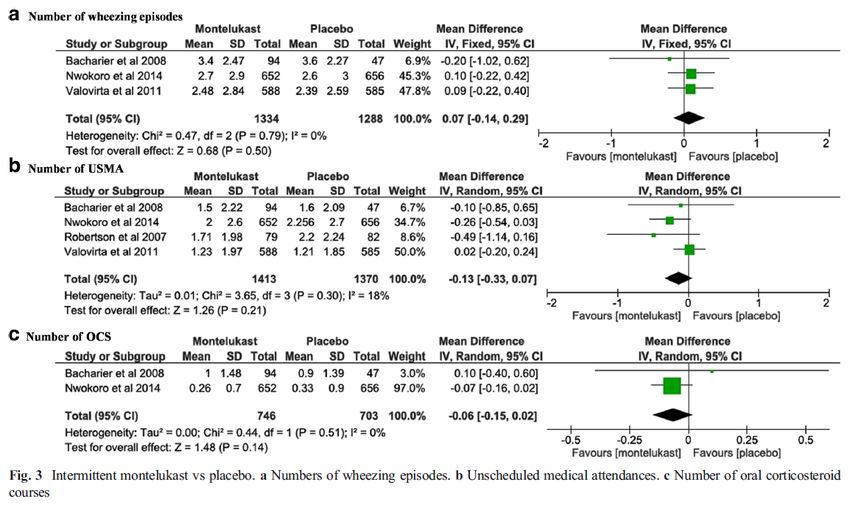
Give diagnostic trial for 3 months.Exazerbationsvermeidung: Montelukast: Time to say goodbye?
Strategien der Exazerbationsvermeidung: ad-hoc LTRA
Vorschulkinder ≤6 Jahren: recurrent wheeze
Hussein et al., Eur J Pediatr 2017Strategien der Exazerbationsvermeidung: ad-hoc ICS
Vorschulkinder ≤6 Jahren: recurrent wheeze
Kaiser et al., Pediatrics 2016Strategien der Exazerbationsvermeidung: ICS vs LTRA
Vorschulkinder ≤6 Jahren: recurrent wheeze
Kaiser et al., Pediatrics 2016Montelukast
Neuropsychiatrische Nebenwirkungen
– Auftreten innerhalb von 2 Wochen nach Therapiebeginn
k as t
n t e lu
– Irritabilität, Aggressivität, Schlafstörung
n M o
rt vo l t e r ?
n we h u l a
e c
Stell im Vors
– Relatives Risiko vs ICS = 12 (2-90)
Benard et al., ERJ 2017Präventive Dauertherapie: ICS/LABA endlich auch bei Vorschulkindern?
Wirksamkeit und Sicherheit von ICS/LABA bei
Vorschulkindern
Fluticason-proprionat/Salmeterol
< 5 Jahre, n= 796
Retrospektive Datenauswertung
Hatziagorou et al.., J Asthma 2018Wirksamkeit und Sicherheit von ICS/LABA bei
Vorschulkindern
Die Häufigkeit von Wheezing war ein Jahr nach ICS/LABA-Start
signifikant reduziert (3% vs. 40%).
Hatziagorou et al.., J Asthma 2018Wirksamkeit und Sicherheit von ICS/LABA bei
Vorschulkindern
Keine SAEs
Irritabilität 2%
Heiserkeit 0.2%
Hatziagorou et al.., J Asthma 2018Therapie: Schulkinder von 6 bis 12 Jahren
Behandlungsplan n. GINA (2018)
Diagnosis
Symptom control & risk factors
(including lung function)
E
Inhaler technique & adherence
NS
O
Patient preference
SP
AS
RE
Symptoms NT
TME
S
EA
ES
W
Exacerbations TT R
S
E
ADJU
S
Side-effects VI
RE
Asthma medications
Patient satisfaction Non-pharmacological strategies
Lung function Treat modifiable risk factors
STEP 5
STEP 4
Refer for
add-on *Not for childrenPräventive Dauertherapie: Neues von GINA!
Therapie: Jugendliche und Erwachsene ab 12 Jahre
Behandlungsplan n. GINA (2019)
Box 3-5A Confirmation of diagnosis if necessary
Adults & adolescents 12+ years Symptom control & modifiable
risk factors (including lung function)
Comorbidities
Inhaler technique & adherence
Personalized asthma management: Patient goals
Assess, Adjust, Review response
Symptoms
Exacerbations
Side-effects
Lung function
Patient Treatment of modifiable risk
satisfaction factors & comorbidities STEP 5
Non-pharmacological strategies
Education & skills training High dose
Asthma medication options: ICS-
Asthma medications STEP 4
Adjust treatment up and down for LABA
individual patient needs STEP 3 Medium dose Refer for
phenotypic
STEP 2 ICS-LABA
assessment
PREFERRED STEP 1 Low dose
± add-on
CONTROLLER Daily low dose inhaled corticosteroid (ICS), ICS-LABA therapy,
to prevent As-needed or as-needed low dose ICS-formoterol * High dose e.g.tiotropium,
exacerbations and low dose ICS, add-on anti-IgE,
control symptoms ICS- anti-IL5/5R,
tiotropium, or
formoterol anti-IL4R
Other Leukotriene receptor antagonist (LTRA), or Medium dose add-on LTRA Add low dose
controller Low dose ICS OCS, but
low dose ICS taken whenever SABA taken † ICS, or low #
options taken whenever consider
dose
SABA is taken side-effects
ICS+LTRA #
†
PREFERRED As-needed low dose ICS-formoterol * As-needed low dose ICS-formoterol ‡
RELIEVER
Other As-needed short-acting β2 -agonist (SABA)
reliever
option * Off-label; data only with budesonide-formoterol (bud-form) ‡ Low-dose ICS-form is the reliever for patients prescribed
† Off-label; separate or combination ICS and SABA inhalers bud-form or BDP-form maintenance and reliever therapy
# Consider adding HDM SLIT for sensitized patients with
allergic rhinitis and1 FEV >70% predicted
© Global Initiative for Asthma, www.ginasthma.orgWas noch?
Jugendliche sind SMART
n e n,
b a t i o
a z e r I C S
r E x a ti v e
e l
Zusatzhübe
e nig u m u
W ge r k
i
4x
wen
4x
2x
3x
2x
2x
1x
1x
1x
Fix 1x tgl: Formoterol / Budesonid (Symbicort®)
SMART: Symbicort Maintainance and Reliever Therapy
(alternative Vannair, Flutiform)Exazerbationsvermeidung: Bringt`s eine ICS Super-Eskalation?
Verdoppelung der ICS-Dosis Exazerbationsvermeidung?
r I CS
ng de
p e lu m
d o p ks a
Ver icht wir
n
Primary Outcome:
Therapieversagen (Bedarf an OCS)
Kew KM et al., Chochrane 2016Verfünffachung der ICS-Dosis bei Exazerbationen
Kinder 5-11 Jahre mildes bis moderates Asthma
n=254 Fluticason 2x 88 mcg vs 2x 440 mcg / Tag
(«schwere Exazerbation»)
h ie d
t er sc
Un
Kein
Jackson et al. , NEJM 2018I CS
g d er
ch u n k sa m
n ffa n wir
ü u
Verf indern
bei K
- Aber: höhere kumulative Steroid-Dosis (+16%)
- Erhöhtes Risiko einer Wachstumsverminderung (-0.23 cm, p=0.06)36
Akute Asthma-Exazerbation: Bronchienerweiterer
– Nur auf der Notfallstation
um Hospitalisationen zu
vermeiden
– Nur Kinder >2 Jahre mit
schwerer Exazerbation
Alternativ Salbutamol 0.5% via Vernebler:
20 Tropfen (=1 ml = 5 mg) in 2 ml NaCl 0.9%
Augsburger et al., Paediatrica 2018; 17:285-263Akute Asthma-Exazerbation:
Systemische Kortikosteroide (Beginn innerhalb 1 Stunde)
Augsburger et al., Paediatrica 2018; 17:285-263Exazerbationstherapie: OCS schon zu Hause?
OCS-Gebrauch zu Hause bei Asthma-Exazerbation
2-18 Jahre, n=132
Moderates bis schweres Asthma
Outcome: «Healthcare utilization"
Notfallbesuche
Sarzynski et al., Paed Pulmonol 2017OCS-Gebrauch zu Hause bei Asthma-Exazerbation
2-18 Jahre, n=132
Moderates bis schweres Asthma
Outcome: «Healthcare utilization"
Stat. Aufnahmen
Sarzynski et al., Paed Pulmonol 2017OCS-Gebrauch zu Hause bei Asthma-Exazerbation
2-18 Jahre, n=132
Moderates bis schweres Asthma
Outcome: «Healthcare utilization"
Intensivstation
Sarzynski et al., Paed Pulmonol 2017Schweres Asthma Neue medikamentöse Strategien: Was macht denn da Sinn?
Was noch?
Metaanalyse 40 Studien
Spezifische Immuntherapie Efficacy: n=17 SCIT, n=11 SLIT
Saftey: n=8 SCIT, n=4 SLIT
≤ 18 Jahre
Asthma-Outcome
• SCIT reduziert Asthma-Medikamentenverbrauch
• SCIT verbessert QoL und FEV1
• SLIT reduziert Medikamentenverbrauch
• SLIT verbessert FEV1
• Ungenügende Evidenz, dass SIT Asthma-Symptome verbessert
oder Notfallbesuche reduziert
Rice et al., Pediatrics 2018Was noch? Tiotropium (ein LAMA) • Tiotropium als Add-on in der Dauertherapie bei Asthma • EMA ab 6 für Asthma, Swissmedic KEINE Zulassung für Asthma • (CH: Zulassung für COPD ab 18 Jahre) • Voraussetzung: Asthma mit hochdosiert ICS plus LABA nicht ausreichend kontrolliert • Ohne Vorschaltkammer • Sehr gutes Sicherheitsprofil
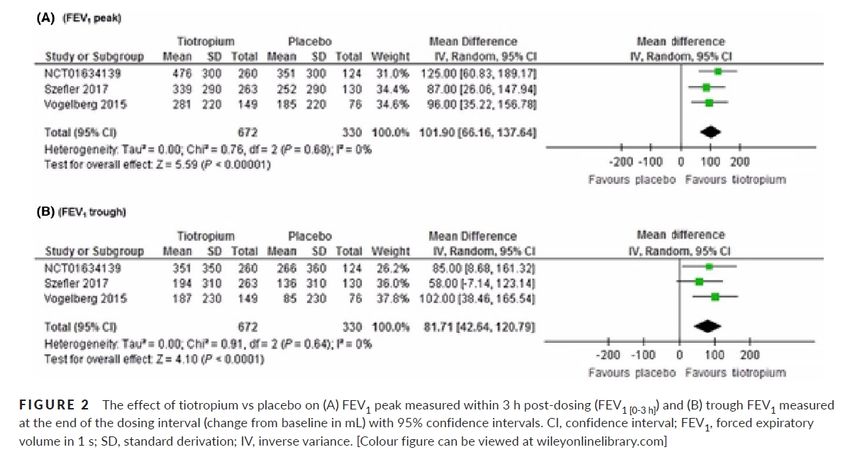
Was noch? Metaanalyse 3 Studien
Tiotropium bei Schulkindern 6-11 Jahre (n>900)
Tiotropium ad-on ICS±LABA
Rodrigo et al., PAI 2017Was noch? Metaanalyse 3 Studien
Tiotropium bei Schulkindern 6-11 Jahre (n>900)
Tiotropium ad-on ICS±LABA
Rodrigo et al., PAI 2017Was noch?
Tiotropium bei Vorschulkindern
Vrijlandt et al., Lancet 2018Was noch?
Biologika
Bel et al., Chest 2017
E. Bel et al. Chest 2017Zugelassene Biologika
• Omalizumab (Anti-IgE) Xolair® Allergisches Asthma
(ab 6 Jahren)
• Mepolizumab (Anti-IL-5), Nucala® (ab 12 Jahren)
• Reslizumab (Anti-IL-5), Cinqair® / Cinquero ® Eosinophiles Asthma
• Benralizumab (Anti-IL-5R), Fasenra® (ab 18 Jahren)Omalizumab (anti-IgE, Xolair®)
• Zulassung Schweiz
• 2006 schweres allergisches Asthma ab 6 Jahren
• 2014 chronische Urticaria ab 12 Jahren
• Indikationen
• Schweres persistierendes allergisches Asthma mit FEV1Omalizumab (anti-IgE, Xolair®)
• Humanisierter monoklonaler Antikörper gegen IgE
• Bindung von freiem IgE, Hemmung der Histaminausschüttung
• Keine Bindung von an den hochaffinen IgE-Rezeptor (FcεRI)
gebundenes IgE von Mastzellen, Basophilen undDCs
• Downregulation der
IgE-Rezeptoren
auf BasophilenOmalizumab (anti-IgE, Xolair®): allergisches Asthma
• Reduktion der Exazerbationsrate: alle (ca. 20%), schwere (ca.
50%)
Busse WW, NEJM 2011, 364(11):1005-15Omalizumab (anti-IgE, Xolair®): allergisches Asthma
• Reduktion der inhalativen Steroid-Dosis (ICS)
Busse WW, NEJM 2011, 364(11):1005-15Omalizumab: Real-life data
Global Evaluation of Treatment Effectiveness
Humbert et al., ERJ 20187-18 Jahre, n=19
Omalizumab: QoL Kinder & Eltern
2 Jahre nach Start
Pediatric Asthma Quality of Life Questionnaire (PAQLQ)
Pediatric Asthma Caregiver’s Quality of Life Questionnaire (PACQLQ)
Sztafińska et al., Advanc Dermatol Allergol 2017Mepolizumab (anti-IL-5, Nucala®, Cinqair®)
• Humanisierter monoklonaler IL-5-Antikörper
• verhindert Bindung von IL-5 an Eosinophile
• Blockade des Singalweg und Reduktion der Eosinophilen-
Differenzierung, -Rekrutierung, -Aktivierung und -Überleben
• 2019 Zulassung Schweiz ab 12 Jahren (Nucala), bzw. ab 18 Jahren
• Indikationen
• schweres eosinophiles Asthma
• und mind. 2 Exazerbationen in den letzten 12 Monaten unter
aktueller Standardtherapie
• und/oder Notwendigkeit zur Therpie mit sytemischen CS
• und Blut-Eosinophile ≥150/µl bei Therpiebeginn oder ≥300/µl
während der letzten 12 MonateMepolizumab (anti-IL-5, Nucala®) • Reduktion der Exazerbationsrate (DREAM-Studie) • Reduktion der Exazerbationsrate bei 100mg (MENSA): 53% • Reduktion des oralen Steroidbedarfs (SIRIUS): 64% (Placebo 44%)
Schweres Asthma: unser Baukasten
Hochdosiert ICS/LABA
+ LAMA + spezifische +
(Tiotropium) Immuntherapie Rehabilitation
/Schulung
+ Biologicals
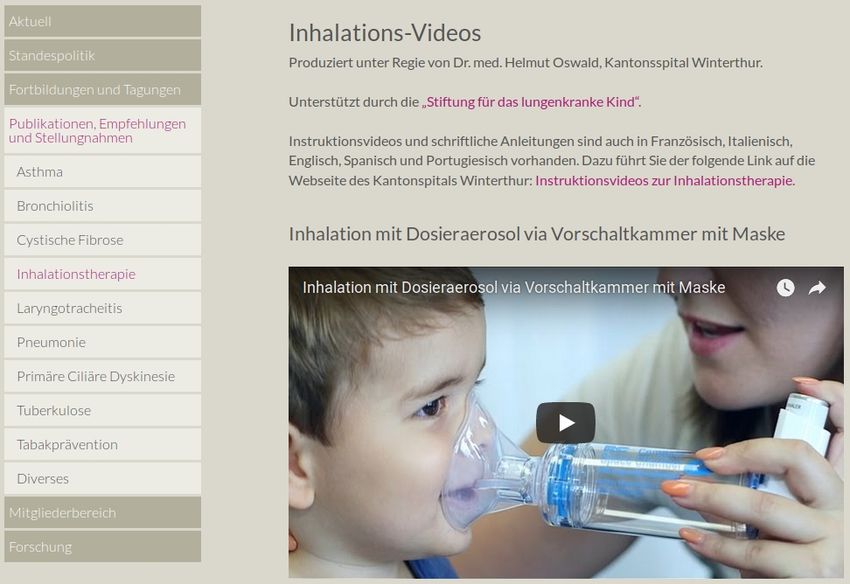
(Omalizumab)Inhalationstherapie
Feucht oder Trocken? Pulver, Spray: – Wirkstoffinhalation (z.B. Ventolin, Axotide, Symbicort, Relvar, Spiriva) Düsenvernebler, Membranvernebler: - Sekretolytische Therapie (Mucoclear, Pulmozyme) - Antibiotika (TOBI/Bramitop, Colistin/Colifin, Cayston) - Atrovent - In Ausnahmesituationen: Ventolin (z.B. auf dem Notfall) Besondere Devices: - z.B. Respimat, Podhaler, Easyhaler, Aerolizer, Handyhaler u.a.
Trockeninhalation: Dosieraerosol und Pulverinhalatoren
Korrekte Inhalationstechnik durch
u n g : s i g e
medizinisches Personal? Lös gelmäs
n d r e
at e u ng !
äq u h u l u
Ad S c
Plaza et al., JACI Pract 2018Wirkstoffdeposition bei der Inhalationstherapie:
Anspruch und Realität
© R. JohannsenDosieraerosol
– Immer mit Vorschaltkammer
– Ab 2 Jahren ohne Maske
– Bis ca. 7 Jahre, danach Pulver
– Technik:
a. Langsame tiefe Ruheatmung
b. Tiefe Inspiration mit Luft anhalten
(analog zum Pulverinhalator)
Die korrekte Inhalationstechnik
muss IMMER geschult werden!Pulverinhalatoren
Turbuhaler Diskus Ellipta
PIF 60 l/min 30 l/min 40 l/min
Alter ca. ab 8-9 J. ca. ab 6-7 J. ca. ab 7-8 J.
Vor Verordnung IMMER PIF prüfen und Technik schulen (z.B. Turbutester)!Hygiene, Reinigung, Wartung Vorschaltkammer: – Nach jeder Inhalation: Mundstück abnehmen, mit heissem Wasser ggfs. mit Spülmittel abspülen und trocknen lassen – Nicht von innen ausreiben (Antistatik geht verloren) – 1x/Woche: Spülmaschine (50°C) oder Auskochen oder Vaporisator – Wenn Lamellen oder Plastik porös oder undicht werden: austauschen Pulverinhalatoren: – Nach jedem Gebrauch abwischen – Keine Desinfektion – Nicht in Inhalator blasen oder atmen (Feuchtigkeit)
68
www.sgpp-sspp.ch
69Sie können auch lesen