Dermatologica Helvetica 9 / 2011 - Elektronisches Epiderm
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten

Dermatologica
Helvetica
Elektronisches Epiderm Epiderme électronique
Vulvodynie Vulvodynie
Impfung gegen Gürtelrose Vaccin anti-zona
Fokus Wundheilung und Focus cicatrisation et
therapeutische Perlen perles thérapeutiques
9 / 2011
Volume 23
NEU
Excipial ®
U Lip
ohne Pa olotio
rfum
Emollientien, so individuell
wie der Hautzustand Ihres
Patienten
Kassenzulässig.
Excipial® Crème, Fettcrème, Fettsalbe, Mandelölsalbe
Z: Crème: Lipidgehalt 35.5%; Fettcrème: Lipidgehalt 54%; Fettsalbe: Lipidgehalt 100%; Mandelölsalbe: Mandelöl 751 mg/g, Zinkoxid 40 mg/g, Lipidgehalt 96%. I: Hautpflege,
Intervallbehandlung mit Kortikoidpräparaten, Grundlagen für magistrale Rezepturen. D: 2–3 × tgl. auftragen. KI: Überempfindlichkeit auf einen Inhaltsstoff. UAW: Unverträg-
lichkeitsreaktionen sind nicht auszuschliessen. SS/ST: Keine Einschränkungen. P: Crème, Fettcrème, Mandelölsalbe: Tuben à 30 g und 100 g. Fettsalbe: Tuben à 100 g. Liste D, SL.
Weiterführende Informationen entnehmen Sie dem Arzneimittel-Kompendium der Schweiz. 0710
Excipial® U Hydrolotio, Lipolotio
Z: U Hydrolotio: Ureum 20 mg/ml, Lipidgehalt 11%; U Lipolotio mit/ohne Parfum: Ureum 40 mg/ml, Lipidgehalt 36%. I: Schutz und Pflege von empfindlicher oder leicht entzün-
deter Haut vom normalen bis leicht trockenen Hauttyp (U Hydrolotio) und trockenen bis sehr trockenen Hauttyp (U Lipolotio), Intervallbehandlung mit Kortikoidpräparaten.
D: 2–3 × tgl. auftragen. KI: Nicht auf Wunden und offenen Hautpartien anwenden. P: Lotio, Flaschen à 200 ml (SL) und 500 ml (Grand-Frère Regelung). Liste D.
Weiterführende Informationen entnehmen Sie dem Arzneimittel-Kompendium der Schweiz. 0711/180711
Spirig Pharma AG, CH-4622 Egerkingen, www.spirig.ch
SOMMAIRE
4 Journal Club
RUBRIKEN DER DERMATOLOGICA HELVETICA 8 Fokus – Focus
RUBRIQUES DE DERMATOLOGICA HELVETICA
12 SGDV - SSDV
Weiterbildung
Formation continue 24 Report
Redaktionsbüro / Bureau éditorial 26 Terminologie
J.-H. Saurat Chefredaktor 28-36 Peer-reviewed original work
Editeur en chef
39 Quiz
M. Harms Stv. Chefredaktorin
Editeur en chef adjointe 42 Industrie
A.A. Navarini Assoziierter Redaktor
Editeur associé
A.M. Skaria Redaktor Westschweiz
Editeur député pour la Suisse
romande Authors instructions (peer reviews) Warnung / Avertissement
T. Hofer Redaktor Deutschschweiz Size: Papers should comprise approximately 700-2000 words Für den Inhalt ausserhalb des redaktionellen Teils
Editeur député pour la Suisse including figures, tables and references. (insbesondere Anzeigen, Industrieinformationen,
alémanique Pressezitate und Kongressinformationen) über-
Title page: The first page of each paper should indicate the nehmen Redaktion und Verlag keine Gewähr. Eine
title, the authors’ names, the institute where the work was Markenbezeichnung kann warenzeichenrechtlich
C. Mainetti Redaktoren Tessin
F. Pelloni Editeurs députés pour le Tessin conducted, and a short title for use as running head. geschützt sein, auch wenn bei ihrer Verwendung
Full address: The exact postal address of the corresponding in dieser Zeitschrift das Zeichen® oder ein anderer
e-mail : derm.helv@bluewin.ch author complete with postal code must be given. Hinweis auf etwa bestehende Schutzrechte fehlen
Key words: For indexing purposes, a list of 3–5 key words in sollten.
English is essential for all papers.
L’éditeur et la rédaction déclinent toute responsa-
Journal-Klub / Journal-Club Abstract: Normally each paper needs an abstract of not more bilité concernant le contenu non rédactionel du
Fokus / Focus than 150 words. It should contain the following information: périodique (en particulier les annonces, les infor-
J.-H. Saurat Redaktionsbüro / Bureau éditorial purpose of the study, procedures, results, conclusions and mations émanant de l’industrie, les citations tirées
derm.helv@bluewin.ch message of the paper. Abstracts submitted for publication de la presse et les informations issues de congrès).
in the section Original Papers should be structured as follows: Une marque déposée peut jouir d’une protection
Klinische Fälle / Cas cliniques / Report Background: What is the major problem that prompted the légale même si elle est mentionée dans le pério-
Universitätskliniken und praktizierende Ärzte study dique sans le symbole ® ou toute autre marque
Les cliniques universitaires et les praticiens signalant, le cas échéant, une telle protection ju-
• Objective: What is the purpose of the study? ridique.
• Methods: How was the study performed?
Peer-reviewed original work / FMH preparation
A.A. Navarini • Results: Most important findings? Dosierungsangaben von Medikamenten:
alexander.navarini@usz.ch • Conclusion: Most important conclusion?
Footnotes: Avoid footnotes. When essential, they are num- Autoren und Verlag haben alle Anstrengungen
bered consecutively and typed at the foot of the appropriate unternommen, um sicherzustellen, dass Auswahl
page. und Dosierungsangaben von Medikamenten im
Neues aus dem Fachgebiet vorliegenden Text mit den aktuellen Vorschriften
Nouvelles professionnelles Formatting rules: und der Praxis übereinstimmen. Trotzdem muss
• Do not use any special page layout. If you would like to der Leser im Hinblick auf den Stand der Forschung,
see what your manuscript looks like with embedded ta- Änderungen staatlicher Gesetzgebungen und den
Forum des Präsidenten der SGDV / bles and illustrations, remember that we need text and unterbrochenen Fluss neuer Forschungsergeenisse
Tribune du Président de la SSDV illustrations as separate files! bezüglich Medikamentenwirkung und -nebenwir-
J.-P. Grillet • Enter your text continuously flush left. Do not use hard re- kungen darauf aufmerksam gemacht werden, dass
jeanpierre.grillet@hin.ch turns ("enter") within a paragraph, only at its end. unbedingt bei jedem Medikament der Packungs-
prospekt konsultiert werden muss, um mögliche
• Do not use footer and header functions. Änderungen im Hinblick auf Indikation und Dosis
Neues aus der SGDV / Nouvelles de la SSDV • Use boldface and italics as well as sub- and superscript
M. Pongratz nicht zu übersehen. Gleiches gilt für spezielle War-
where appropriate. nungen und Vorsichtsmassnahmen. Ganz beson-
e-mail: sgdv-ssdv@hin.ch
• Use your word-processing program to insert Greek letters, ders gilt dieser Hinweis für empfohlene neue und/
mathematical symbols, etc. oder nur selten gebrauchte Wirkstoffe.
Neues aus den Kliniken / Nouvelles des cliniques Alle Rechte vorbehalten. Ohne schriftliche Geneh-
Klinikdirektoren / Les directeurs des cliniques Legends: The legends to your figures are part of the text and
should be listed at the end of your text file. migung des Verlags dürfen diese Publikation oder
Teile daraus nicht in andere Sprachen übersetzt
Neues aus den kantonalen Fachgesellschaften / Line Drawings oder in irgendeiner Form mit mechanischen oder
Nouvelles des Sociétés cantonales de la spécialité Black and White Half-Tone Images, Color Illustrations elektronischen Mitteln (einschliesslich Fotokopie,
Präsidenten der Gesellschaften / Les présidents des sociétés Scans Tonaufnahme und Mikrokopie) reproduziert oder
• For processing and retouching scanned half-tone images, auf einem Datenträger oder einem Computersys-
Ankündigungen (Kongresse/Kolloquien) und Berichte / Photoshop is recommended. Please save the original scan tem gespeichert werden.
Annonces (congrès/colloques) et Bureau éditorial as well as your processed version.
derm.helv@bluewin.ch • Export black and white half-tones and color illustrations as Posologie des médicaments:
TIF or EPS format, as close as possible to their anticipated Les auteurs et l’éditeur ont tout mis en œuvre pour
Freies Forum / Tribune libre size in print.
Redaktionsbüro / Bureau éditorial s’assurer que le choix des médicaments et la po-
• Save them as separate files, not embedded in the text. sologie préconisés dans ce texte soient conformes
derm.helv@bluewin.ch
• Scanned line drawings must be digitalized with a resolu- aux recommandations et à la pratique au moment
tion of at least 800, better 1000 dpi (dots per inch) after de la publication. Cependant, compte tenu des re-
Humor / Billet d’humour et d’humeur cherches en cours, des changements dans les légis-
J.P. Grillet scaling.
• Scanned half-tone images should be digitalized with a fi- lations et de l’afflux constant de données nouvelles
derm.helv@bluewin.ch concernant la thérapie médicamenteuse et l’effet
nal resolution of 300 dpi, a 12 bit grayscale accuracy and des médicaments, il est vivement recommandé
Neues aus der Industrie / Nouvelles de l’industrie a density range of 2.8. Screen values must lie between 5% au lecteur de vérifier sur la notice jointe à chaque
Redaktionsbüro / Bureau éditorial and 95%. emballage si aucune modification n’est intervenue
derm.helv@bluewin.ch • Scanned color illustrations must be digitalized in RGB dans la posologie et si aucune nouvelle contre-in-
mode with a resolution of at least 300 dpi, a 32 bit accura- dication ou précaution à prendre n’a été signalée.
Druck / Impression cy and a density range of 2.8. Cela est particulièrement important lorsque l’agent
Atar Roto Presse SA, Vernier • Summary. recommandé est nouveau ou peu employé. Tous
droits de reproduction, même partielle, sous n’im-
Make sure that your original has the resolution values in this porte quelle forme, strictement réservés.
table after scaling, otherwise the printing quality may be in-
ISSN : 1420-2360 adequate.
Detailled authors instruction will soon be avaible on our
ANZEIGENREGIE / RÉGIE DES ANNONCES upcoming website.
Carine HERRERAS
Tél : +41 79 667 32 48
3
Fax: +41 22 372 94 95
E-mail : derm.helv@bluewin.ch
Epidermal Electronics
KIM D-H, LU N, MA R, KIM Y-S, KIM R-H,
WANG S, WU J, WON SM, TAO H, ISLAM A,
YU KJ, KIM T-I, CHOWDHURY R, YING M,XU L,
LI M, CHUNG H-J, KEUM H, MCCORMICK M,
LIU P, ZHANG Y-W, OMENETTO FG, HUANG Y,
COLEMAN T, ROGERS JA
University of Illinois at Urbana-Cham-
paign, Urbana, USA
Science 2011, 333 : 838-42
We report classes of electronic systems
that achieve thicknesses, effective elas-
tic moduli, bending stiffnesses, and ar-
eal mass densities matched to the epi-
dermis. Unlike traditional wafer-based
technologies, laminating such devices
onto the skin leads to conformal contact
and adequate adhesion based on van
der Waals interactions alone, in a man-
ner that is mechanicallyinvisible to the Fig. 1. Information caught by film. A flexible electronic device attaches to the skin
user. We describe systems incorporat- like a bandage tape and can be used to acquire physiological information without
ing electrophysiological, temperature, bulky electrodes. Kim et al. developed an electronic skin in the form of a highly
and strain sensors, as well as transistors, stretchable net, consisting of various sensors and electronics of serpentine shapes,
light-emitting diodes, photodetectors, that is sandwiched between two protection layers of equal thickness. The device
radio frequency inductors, capacitors, layer sits on a polyester layer that was engineered with mechnical properties to
oscillators, and rectifying diodes. Solar match those of natural skin. Reprinted with permission from AAAS.
cells and wireless coils provideoptions
for power supply. We used this type of
technology to measure electrical activity
J O U R N A L C LU B
producedby the heart, brain, and skel-
etal muscles and show that the resulting
data contain sufficient information for an
unusual type of computer game control-
ler. See also Fig 1 & 2.
Fig. 2. (A) Image of a demonstration platform for multifunctional electronics with physical
properties matched to the epidermis. Mounting this device on a sacrificial, water-soluble film
of PVA, placing the entire structure against the skin, with electronics facing down, and then
dissolving the PVA leaves the device conformally attached to the skin through van der Waals
forces alone, in a format that imposes negligible mass or mechanical loading effects on the
skin. (B) EES partially (top) and fully (bottom) peeled away from the skin. (Inset) A represen-
tative cross-sectional illustration of the structure, with the neutral mechanical plane (NMP)
defined by a red dashed line. (C) Multifunctional EES on skin: undeformed (left), compressed
(middle), and stretched (right). (D) A commercial temporary transfer tattoo provides an al-
ternative to polyester/PVA for the substrate; in this case, the system includes an adhesive to
improve bonding to the skin. Images are of the backside of a tattoo (far left), electronics in-
tegrated onto this surface (middle left), and attached to skin with electronics facing down in
undeformed (middle right) and compressed (far right) states. Reprinted with permission from
AAAS.
4 Dermatologica Helvetica - Volume 23(9) - Novembre 2011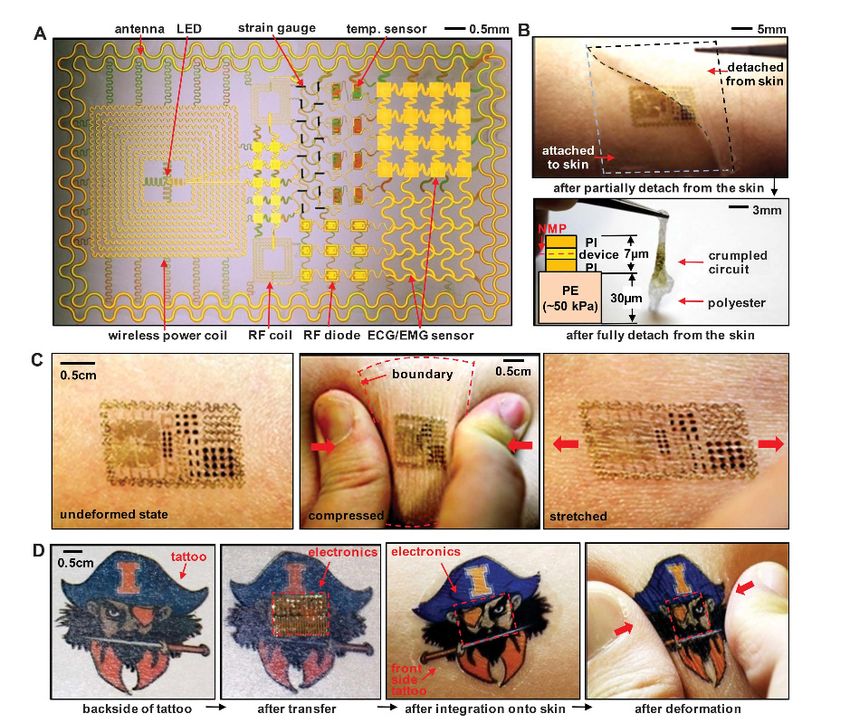
Xéroses cutanées*
L‘essentiel
DEXERYL
Glycérol, vaseline, paraffine liquide
®
NOUVEAU
L‘émollient le plus
prescrit en France1) arf
s p um
san
•
•
ne
an i
s la n ol
s
• efficacité médicale 2) 3)
• excellente tolérance 4)
• galénique optimisée
• nombreuses applications:
de l‘ichtyose aux dermatoses professionelles
et de la xérose sénile au pied diabétique
• prix économique et
admis aux caisses maladies
Liste D
Crème (50 g/250 g)
Remboursé
NOUVEAU: www.pierre-fabre-dermatologie.ch
1) Données IMS France 2010 2) L.Vaillant, G.Georgesco, C.Rivollier. Etude comparative, randomisée, en double aveugle des propriétés de V0034CR (véhicule + glycérol + vaseline) versus véhicule, versus véhicule + glycérol, versus véhicule
+ vaseline, chez des sujets présentant une peau sèche non pathologique. Rapport d’étude V00034 CR 202, 2003. 3) C. Blanchet-Bardon, H. Buckova, H. Raudsepp, H.Traupe. Efficacité et tolérance de DEXERYL dans le traitement
symptomatique des ichtyoses infantiles. Réalités Thérapeutiques en Dermato-Vénérologie n°190 Octobre 2009. 4) Données de pharmacovigilance, Pierre Fabre France 1999–2010.
Information professionnelle abrégée DEXERYL® Crème :
C : Principe actif : Glycerolum, Vaselinum album, Paraffinum liquidum. Excipients : Conserv.: Propylis parahydroxybenzoas (E 216), Macrogolum 600, excipiens ad emulsionem. *I: Traitement des états de sécheresse
cutanés de certaines dermatoses, p.ex. états ichtyosiques. P: appliquer deux fois par jour ou plus souvent si nécessaire. CI : Hypersensibilité à l’un des composants. PE : Ne pas avaler. Ne pas appliquer sur des plaies
infectées. Réactions allergiques (éventuellement retardées) possibles au parahydroxybenzoate de propyle et au macrogol 600. IA : Aucune étude n’a été réalisée. GA : On ne dispose d’aucune information. DEXERYL®
10/2011
peut cependant être utilisé pendant la grossesse et l’allaitement (durant lequel il est recommandé de ne pas appliquer la crème sur la poitrine). EI : occasionnellement : urticaire, érythème, prurit. Cas isolés : eczéma.
S : Aucun cas de surdosage n’a été rapporté. Catégorie de vente : Liste D. Admission aux caisses maladies. Pour des informations complètes et détaillées, veuillez consulter le Compendium Suisse des Médicaments.
Pierre Fabre (Suisse) SA, 4123 Allschwil. 01/2011.
Hegenheimermattweg 183 • 4123 Allschwil
061 487 89 00 • dermatologie.ch@pierre-fabre.com
Mutual Antagonism of T Cells Causing Psoriasis tic in a range of inflammatory skin disorders such
and Atopic Eczema as psoriasis and AD. Clinical evaluation of topical
INCB018424 is ongoing.
EYERICH S, ONKEN AT, WEIDINGER S, FRANKE A, NA-
SORRI F, PENNINO D, GROSBER M, PFAB F, SCHMIDT-
WEBER, CB MEMPEL M, HEIN R, RING J, CAVANI A, EYE-
RICH K
Technische Universität Munich, Munich, Germany Topical Treatment of Basal Cell Carcinomas in
Nevoid Basal Cell Carcinoma Syndrome with a
New England Journal of Medicine 2011, 365:231-8 Smoothened Inhibitor
The simultaneous occurrence of psoriasis driven SKVARA H, KALTHOFF F, MEINGASSNER JG, WOLFF-
by type 1 helper T (Th1) cells and type 17 helper WINISKI B, ASCHAUER H, KELLEHER JF, WU XPAN S,
T (Th17) cells and atopic eczema dominated by MICKEL L, SCHUSTER C, STARY G, JALILI A, DAVID OJ,
type 2 helper T (Th2) cells is rare. Here, we describe EMOTTE C, COSTA ANTUNES AM, ROSE K, DECKER J,
three patients with co-occurring psoriasis and CARLSON I, GARDNER H, STUETZ A, BERTOLINO AP,
atopic eczema with an antagonistic course and STING G, DE RIE MA
distinct T-cell infiltrates in lesions from psoriasis Medical University of Vienna, Vienna, Austria
and those from atopic eczema. Sensitized patients
with psoriasis had a reaction to epicutaneous al- Journal of Investigative Dermatology 2011, 131:1735-
lergen challenge, with clinically and histologically 44
verified eczema lesions containing a large number
of allergen-reactive T cells. These findings support Basal cell carcinoma (BCC) is a distinctive manifes-
a causative role for T cells triggered by specific an- tation in nevoid basal cell carcinoma syndrome
tigens in both psoriasis and atopic eczema. (NBCCS) patients. Both inherited and acquired
mutations of patched 1 (PTCH1), a tumor-suppres-
sor gene controlling the activity of Smoothened
(SMO), are the primary cause of the constitutive
activation of the Hedgehog (HH)
Preclinical Evaluation of Local JAK1 and JAK2 In- pathway, leading to the emergence of BCCs in
hibition in Cutaneous Inflammation NBCCS. LDE225, a distinct, selective antagonist of
SMO, showed potent inhibition of basaloid tumor
FRIDMAN JS, SCHERLE PA, COLLINS R, BURN T, NEILAN nest formation and mediated regression of pre-
CL, HERTEL D, CONTEL N, HALEY P, THOMAS B, SHI J, formed basaloid tumors in organ cultures of skin
COLLIER P, RODGERS JD, SHEPARD S, METCALF B, HOL- derived from Ptch1 heterozygous knockout mice.
LIS G, NEWTON RC, YELESWARAM S, FRIEDMAN SM, In a double-blind, randomized, vehiclecontrolled,
VADDI C intraindividual study, a total of 8 NBCCS patients
Incyte Corporation, Wilmington, USA presenting 27 BCCs were treated twice daily with
0.75% LDE225 cream or vehicle for 4 weeks. Ap-
Journal of Investigative Dermatology 2011, 131:1838– plication of 0.75% LDE225 cream was well toler-
44 ated and showed no skin irritation. Of 13 LDE225-
treated BCCs, 3 showed a complete, 9 a partial,
JAKs are required for signaling initiated by several and only 1 no clinical response. Except for one
cytokines (e.g., IL-4, IL-12, IL-23, thymic stromal partial response, the vehicle produced no clinical
lymphopoietin (TSLP), and IFNg) implicated in response in any of the 14 treated BCCs. Treatment
the pathogenesis of inflammatory skin diseases with 0.75% LDE225 cream in NBCCS patients was
such as psoriasis and atopic dermatitis (AD). Di- very well tolerated and caused BCC regression,
rect antagonism of cytokines, such as IL-12 and thus potentially offering an attractive therapeutic
IL-23 using ustekinumab, has proven effective in alternative to currently available therapies for this
randomized studies in psoriasis patients.We hy- indication.
pothesized that local inhibition of cytokine signal-
ing using topical administration of INCB018424, a
small molecule inhibitor of JAK1 and JAK2, would
provide benefit similar to systemic cytokine neu-
tralization. In cellular assays, INCB018424 inhibits Interleukin-36–Receptor Antagonist Deficiency
cytokine-induced JAK/signal transducers and ac- and Generalized Pustular Psoriasis
tivators of transcription (STAT) signaling and the
resultant production of inflammatory proteins MARRAKCHI S, GUIGUE P, RENSHAW BR, PUEL A, X-Y,
(e.g., IL-17, monocyte chemotactic protein-1, and FRAITAG S, ZRIBI J, BAL E, CLUZEAU C, CHRABIE M,
J O U R N A L C LU B
IL-22) in lymphocytes and monocytes, with half- TOWNE JE, DOUANGPANYA J, PONS C, MANSOUR S,
maximal inhibitory concentration values o100 nM. SERRE V, HAFEDH MAKNI H, MAHFOUDH N, FAKHFAKH
In vivo, topical application of INCB018424 resulted F, BODEMER C, FEINGOLD J,HADJ-RABIA S, FAVRE M,
in suppression of STAT3 phosphorylation, edema, GENIN E, SAHBATOU M, MUNNICH A, CASANOVA J-L,
lymphocyte infiltration, and keratinocyte prolifer- SIMS JE, TURKI H, BACHELEZ H, SMAHI A
ation in a murine contact hypersensitivity model Sfax University, Sfax, Tunisia
and inhibited tissue inflammation induced by ei-
ther intradermal IL-23 or TSLP. Topical INCB018424 New England Journal of Medicine 2011, 365:620-8
was also well tolerated in a 28-day safety study
in Gottingen minipigs. These results suggest that Background: Generalized pustular psoriasis is a
localized JAK1/JAK2 inhibition may be therapeu- life-threatening disease of unknown cause. It is
characterized by sudden, repeated episodes of
6 Dermatologica Helvetica - Volume 23(9) - Novembre 2011
high-grade fever, generalized rash, and dissemi- position 27 (L27P). Homology-based structural
nated pustules, with hyperleukocytosis and el- modeling of human interleukin-36Ra suggests
evated serum levels of C-reactive protein, which that the proline at position 27 affects both the sta-
may be associated with plaque-type psoriasis. bility of interleukin-36Ra and its interaction with
Methods: We performed homozygosity mapping its receptor, interleukin-1 receptor–like 2 (inter-
and direct sequencing in nine Tunisian multiplex leukin-1 receptor–related protein 2). Biochemical
families with autosomal recessive generalized analyses showed that the L27P variant was poorly
pustular psoriasis. We assessed the effect of mu- expressed and less potent than the nonvariant
tations on protein expression and conformation, interleukin-36Ra in inhibiting a cytokine-induced
stability, and function. response in an interleukin-8 reporter assay, lead-
Results: We identified significant linkage to an ing to enhanced production
interval of 1.2 megabases on chromosome 2q1- of inflammatory cytokines (interleukin-8 in par-
3-q14.1 and a homozygous missense mutation ticular) by keratinocytes from the patients.
in IL36RN, encoding an interleukin-36–receptor Conclusions: Aberrant interleukin-36Ra structure
antagonist (interleukin-36Ra), an antiinflamma- and function lead to unregulated secretion of in-
tory cytokine. This mutation predicts the substitu- flammatory cytokines and generalized pustular
tion of a proline residue for leucine at amino acid psoriasis.
Repeated Vulvovaginal Fungal Infections Editor’s Summary
Cause Persistent Pain in a Mouse Model of Vul-
vodynia Science Translational Medicine 2011, 3(101):
101ra91
FARMER MA, TAYLOR AM, BAILEY AL, TUTTLE AH,
MACINTYRE LC, MILAGROSA ZE, CRISSMAN HP, BEN- The causes of some chronic pain syndromes have
NETT GJ, RIBEIRO-DA-SILVA A, BINIK YM, MOGIL JS been mysterious. One of these is vulvodynia, in
University of Illinois at Urbana-Champaign, Ur- which the vulva becomes excruciatingly sensi-
bana, USA tive to touch. Now, Farmer and her colleagues re-
inforce one hypothesis as to its origins by show-
Science Translational Medicine 2011, 3(101): ing that a vulvodynia-like state can be induced in
101ra91 mice by repeated yeast infections.
The authors showed that two rounds of vulvar
Provoked vestibulodynia, the most common yeast infection had no effect on the response
form of vulvodynia (unexplained pain of the of mice to touch in the vulvar area, but after a
vulva), is a prevalent, idiopathic pain disorder as- third infection, 6 of 15 mice became hypersensi-
sociated with a history of recurrent candidiasis tive. The vulvar tissue of hypersensitive mice was
(yeast infections). It is characterized by vulvar not inflamed or otherwise abnormal after mi-
allodynia (painful hypersensitivity to touch) and croscopic inspection, but the affected mice did
hyperinnervation. We tested whether repeated, have particularly dense sympathetic and pepti-
localized exposure of the vulva to a common dergic vulvar innervations. A single, long infec-
fungal pathogen can lead to the development tion could have the same effect and, as long as
of chronic pain. A subset of female mice sub- 70 days after the infection cleared up, the mice
jected to recurrent Candida albicans infection were hypersensitive to touch. Live yeast were
developed mechanical allodynia localized to the not required, because injections of the yeast cell
vulva. The mice with allodynia also exhibited hy- wall glucan zymosan produced the same chronic
perinnervation with peptidergic nociceptor and pain syndrome, as measured by hypersensitivity
sympathetic fibers (as indicated by increased to touch.
protein gene product 9.5, calcitonin gene–relat- The re-creation of a vulvodynia-like state in
ed peptide, and vesicular monoamine transport- mice by repeated infection with yeast raises key
er 2 immunoreactivity in the vaginal epithelium). questions that need to be asked in further ex-
Long-lasting behavioral allodynia in a subset of
J O U R N A L C LU B
periments. Does repeated exposure to infection
mice was also observed after a single, extended induce hyperinnervation in some individuals? If
Candida infection, as well as after repeated vul- so, what is the mechanistic basis of this effect?
var (but not hind paw) inflammation induced Is this innervation the cause of the chronic pain
with zymosan, a mixture of fungal antigens. The of vulvodynia? Some of these questions may be
hypersensitivity and hyperinnervation were both best asked in mice, but the ultimate goal is to un-
present at least 3 weeks after the resolution of derstand this process in women well enough to
infection and inflammation. Our data show that effectively interfere with it.
infection can cause persistent pain long after its
resolution and that recurrent yeast infection rep-
licates important features of human provoked
vulvodynia in the mouse.
Dermatologica Helvetica - Volume 23(9) - Novembre 2011 7
Early Results from a Randomized Trial of Saphen- Success Rate of Split-thickness Skin Grafting of
ous Surgery with or without Subfascial Endoscopic Chronic Venous Leg Ulcers Depends on the Presence
Perforator Surgery in Patients with a Venous Ulcer of Pseudomonas Aeruginosa: a Retrospective Study
Background: The aim was to clarify the role of in- The last years of research have proposed that bacte-
F O C U S - C h r o n i c Wo u n d s - Tr e a t m e n t P e a r l s
competent perforators (IPs) in venous leg ulcers. This ria might be involved in and contribute to the lack of
short-term report focused on safety, patient satisfac- healing of chronic wounds. Especially it seems that
tion and the fate of IPs after subfascial endoscopic Pseudomonas aeruginosa play a crucial role in the heal-
perforator surgery (SEPS), or saphenous surgery ing. At Copenhagen Wound Healing Centre it was for
alone. many years clinical suspected that once chronic venous
Methods: Patients aged 30-78 years with an open leg ulcers were colonized (weeks or months preopera-
or recently healed venous ulcer, and with an incom- tively) by P. aeruginosa, the success rate of skin grafting
petent saphenous vein and IPs, were allocated ran- deteriorated despite aggressive treatment. To investi-
domly to saphenous surgery alone, or in combina- gate this, a retrospective study was performed on the
tion with SEPS. A control duplex scan was performed clinical outcome of 82 consecutive patients with chron-
6-9 months after surgery, and clinical follow-up was ic venous leg ulcers on 91 extremities, from the 1(st) of
scheduled after 1 week, 3 and 12 months. A standard March 2005 until the 31(st) of August 2006. This was
questionnaire was completed at each clinical visit. achieved by analysing the microbiology, demographic
Results: Seventy-five patients were enrolled; 37 had data, smoking and drinking habits, diabetes, renal im-
SEPS and 38 had saphenous surgery alone. SEPS pairment, co-morbidities, approximated size and age
prolonged the operation by a median of 15 min (P of the wounds, immunosuppressive treatment and
= 0.003). Duplex imaging revealed significantly more complicating factors on the clinical outcome of each
remaining IPs in the no-SEPS group (P < 0.001). Com- patient. The results were evaluated using a Student
pared with the preoperative scan, significantly more T-test for continuous parameters, chi-square test
legs were free from IPs in the SEPS group compared for categorical parameters and a logistic regression
with the no-SEPS group (21 of 36 versus 7 of 37 re- analysis to predict healing after 12 weeks. The analy-
spectively; P < 0.001). There were no other major out- sis revealed that only 33,3% of ulcers with P. aerugi-
come differences between the groups. nosa, isolated at least once from 12 weeks prior, to or
Conclusion: There was no short-term clinical benefit during surgery, were healed (98% or more) by week
from adding SEPS to saphenous surgery in patients 12 follow-up, while 73,1% of ulcers without P. aerugi-
with varicose ulcers and IPs, although SEPS reduced nosa were so by the same time (p = 0.001). Smoking
the number of perforators remaining after 1 year. also significantly suppressed the outcome at the 12-
week follow-up. Subsequently, a logistic regression
British Journal of Surgery 2011, 98(4):495-500 analysis was carried out leaving P. aeruginosa as the
only predictor left in the model (p = 0.001). This study
supports our hypothesis that P. aeruginosa in chronic
venous leg ulcers, despite treatment, has consider-
mTOR inhibitors slow skin carcinogenesis, but im- able impact on partial take or rejection of split-thick-
pair wound healing ness skin grafts.
Background: Recent studies suggest that patients on
mTOR inhibitors have a reduction in cutaneous car-
cinogenesis by an estimated 50% or more compared PLoS ONE 6(5): e20492
to calcineurin inhibitors. While randomized trials are
running, organ transplant recipients are frequently
switched from calcineurin inhibitors to mTOR inhibi-
tors when cutaneous carcinogenesis increases. Herpes Zoster Vaccine in Older Adults and the Risk
Case report: A heart transplant recipient with a neu- of Subsequent Herpes Zoster Disease
ropathic diabetic foot syndrome developed cutane-
ous carcinogenesis at more than 20 squamous cell Context: Approximately 1 million episodes of herpes
carcinomas (SCC) annually. To slow carcinogenesis, zoster occur annually in the United States. Although
his immunosuppression was switched from the cal- prelicensure data provided evidence that herpes
cineurin inhibitor ciclosporin to the mTOR inhibitor zoster vaccine works in a select study population un-
everolimus. Carcinogenesis slowed to 6 SCC annu- der idealized circumstances, the vaccine needs to be
ally; however, he developed recalcitrant diabetic foot evaluated in field conditions.
ulcers which were purely neuropathic and non-an- Objective: To evaluate risk of herpes zoster after re-
giopathic, and a limb-threatening fistulating necrotic ceipt of herpes zoster vaccine among individuals in
erysipelas of the right leg. Both sites responded poor- general practice settings.
ly to antibiotic therapy, offloading and debridement. Design, Setting, and Participants: A retrospective
This skin fistula became chronic and some toes were cohort study from January 1, 2007, through Decem-
at risk for minor amputation. In view of the propen- ber 31, 2009, of individuals enrolled in the Kaiser
sity for mTOR inhibitors to impair would healing, im- Permanente Southern California health plan. Partici-
munosuppression was switched back to ciclosporin. pants were immunocompetent community-dwelling
All wounds healed rapidly, but skin carcinogenesis adults aged 60 years or older. The 75 761 members
rose to former levels. in the vaccinated cohort were age matched (1:3) to
Conclusions: This case impressively illustrates the 227 283 unvaccinated members.
clinical dilemma for mTOR inhibitor use where benefit Main Outcome Measure: Incidence of herpes zoster.
in carcinogenesis is counterbalanced by impairment Results: Herpes zoster vaccine recipients were more
in wound healing. Changes in immunosuppressive likely to be white, women, with more outpatient vis-
regimes should thus be made on an individual basis its, and fewer chronic diseases. The number of herpes
with careful consideration of the relative risks. zoster cases among vaccinated individuals was 828
in 130 415 person-years (6.4 per 1000 person-years;
British Journal of Dermatology 2011, Epub ahead of print 95% confidence interval [CI], 5.9-6.8), and for unvac-
8 Dermatologica Helvetica - Volume 23(9) - Novembre 2011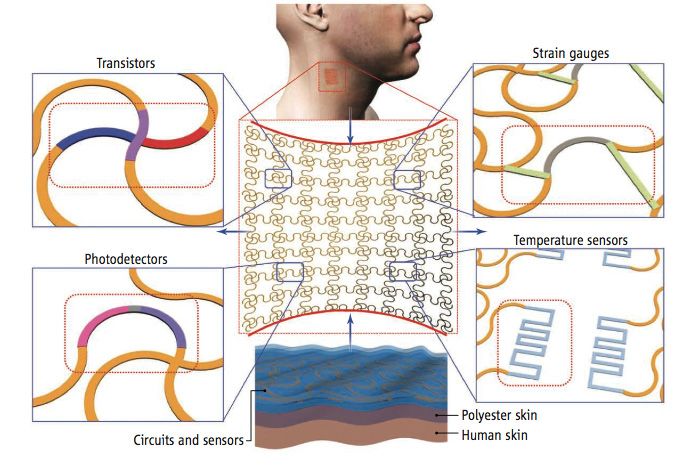
Behandlung der aktinischen Keratose
Wirkt lang anhaltend
und punktgenau*
Stimuliert bei Bedarf das körper-
eigene Immunsystem der Haut
* Krawtchenko N et al. A randomised study of topical 5% imiquimod vs. topical 5-fl uorouracil vs. cryosurgery in immunocompetent patients with actinic keratoses: a comparison of clinical and histological outcomes including
1-year follow-up. BJD 2007; 157(Suppl.2):34–40.
Aldara® 5% Creme (Imiquimod): Immunmodulator. Indikationen: Topische Behandlung des Erwachsenen. 1. Äusserliche spitze Kondylome der Genital- u. Perianalregion. 2. Multiple oberfl ächliche Basalzellkarzinome (Biopsie-
bestätigt; max. 2 cm Tumordurchmesser) am Rumpf (mit Ausschluss der Anal- und Genitalregion), an der Halsregion oder den Extremitäten (ohne Hand und Fuss), wenn chirurgische Entfernung nicht angezeigt und Nachkontrolle
gewährleistet ist. 3. Klinisch typische, nicht-hyperkeratotische, nicht-hypertrophische aktinische Keratosen im Gesicht und auf dem Kopf. Dosierung: Jeweils vor dem Zubettgehen auftragen. Äusserl. spitze Kondylome: 3x
wöchentlich dünn auftragen (max. 16 Wochen) und 6–10 Std. auf der Haut belassen. Oberfl. Basalzellkarzinom: Während 6 Wochen 5x wöchentlich und 8 Std. auf der Haut belassen. Aktinische Keratosen: Während 16 Wochen
3x wöchentlich und 8 Std. auf der Haut belassen. Kontraindikationen: Überempfi ndlichkeit auf Wirkstoff oder einen Hilfsstoff. Behandlung von Kindern und Jugendlichen. Vorsichtsmassnahmen: Offene Geschwüre, Wunden,
chirurgische Eingriffe: erst nach vollständiger Abheilung. Kein Okklusivverband, kein Kontakt mit Augen, Lippen und Nasenschleimhaut, keine Sonneneinwirkung auf die behandelte Haut. Verschlechterung entzündlicher
Hauterscheinungen möglich. Vorsicht bei Patienten mit Autoimmunerkrankungen oder Organtransplantaten. Heftige lokale Entzündungsreaktionen der Haut möglich. Vorsicht bei Vorhautbehandlung unbeschnittener Männer. Nicht
empfohlen bei inneren spitzen Kondylomen der Genitalregion. Während Schwangerschaft und Stillzeit: nur bei absoluter Notwendigkeit. Empfehlungen bzgl. Geschlechtsverkehr und Empfängnisverhütung bei spitzen Kondylomen
sowie weitere indikationsspezifi sche Warnhinweise und Vorsichtsmassnahmen: s. Kompendium. Interaktionen: Nicht untersucht. Interaktionen mit systemisch applizierten Wirkstoffen
sind nur in sehr geringem Masse zu erwarten. Vorsicht bei Patienten mit immunsupressiver Behandlung. Unerwünschte Wirkungen: Sehr häufi g: Reaktionen am Applikationsort (bis 40%).
Häufi g: Infektionen; Kopfschmerzen; Myalgie; Juckreiz, Schmerzen, Brennen am Applikationsort; Müdigkeit. (UW ≤ 1%: s. Kompendium). Packung: OP mit 12 Sachets zum Einmalgebrauch.
(A). Kassenzulässig. Ausführliche Informationen: Packungsbeilage, Arzneimittel-Kompendium oder MEDA Pharma GmbH, 8602 Wangen-Brüttisellen. Stand der Information: Mai 2009.
cinated individuals it was 4606 in 355 659 person- H1-Antihistamine Up-Dosing in Chronic Spontane-
years (13.0 per 1000 person-years; 95% CI, 12.6-13.3). ous Urticaria: Patients’ Perspective of Effectiveness
In adjusted analysis, vaccination was associated with and Side Effects – A Retrospective Survey Study
a reduced risk of herpes zoster (hazard ratio [HR],
0.45; 95% CI, 0.42-0.48); this reduction occurred in all Background: The guidelines recommend that first line
age strata and among individuals with chronic dis- treatment of chronic spontaneous urticaria should
eases. Risk of herpes zoster differed by vaccination be second generation non-sedating H1-antihista-
status to a greater magnitude than the risk of unre- mines with a positive recommendation against the
lated acute medical conditions, suggesting results use of old sedating first generation antihistamines. If
for herpes zoster were not due to bias. Ophthalmic standard dosing is not effective, increasing the dos-
herpes zoster (HR, 0.37; 95% CI, 0.23-0.61) and hospi- age up to four-fold is recommended. The objective
talizations coded as herpes zoster (HR, 0.35; 95% CI, of this study was to obtain the chronic spontaneous
0.24-0.51) were less likely among vaccine recipients. urticaria-patient perspective on the effectiveness
Conclusions: Among immunocompetent communi- and unwanted effects of H1-antihistamines in stan-
ty-dwelling adults aged 60 years or older, receipt of dard and higher doses.
the herpes zoster vaccine was associated with a low- Methodology/Principal Findings: This was a ques-
er incidence of herpes zoster. The risk was reduced tionnaire based survey, initially completed by 368
among all age strata and among individuals with individuals. 319 (248 female, 71 male, median age 42
chronic diseases. years) had a physician-confirmed diagnosis of chron-
ic spontaneous urticaria and were included in the
The Journal of the American Medical Association results. Participants believed standard doses (manu-
2011, 305(2):160-166 facturers recommended dose) of second generation
antihistamines to be significantly (Pof 12 (8.3%) patients found no benefit with the treat-
ment but had also failed multiple other treatments
modalities.
"The young physicians start life with
Limitations: Limitations include the small number of twenty drugs for each disease, and
patients treated and the retrospective nature of the the old physicians ends life with one
study.
Conclusions: Topical nitroglycerin demonstrated ef-
drug for twenty diseases."
ficacy in treating both the symptoms and lesional
appearance of CNH in a noninvasive manner, with William Osler
an overall success rate that is comparable with other
published methods.
Journal of the American Academy of Dermatology
65(3):531-536
Fo c u s
COMESTIBLE…
e pinceau quotidien pour des ongles sains
Le coup d
• Infections fongiques
des ongles, légères à
NON COMESTIBLE… modérément importantes
(sans contamination de la
matrice unguéale)
• Sans limer
• Application facile le soir admis par
les caisses-
• Pratiquement invisible maladie
TRAITABLE!
Information professionnelle abrégée de Ciclopoli® vernis à ongles
Comp: Vernis à ongles avec 80 mg/g de ciclopirox. I: Infections fongiques des ongles, légères à modérément importantes, provoquées par des dermatophytes
et/ou d’autres champignons sensibles au ciclopirox, dans lesquelles la matrice unguéale n’est pas touchée. P/ME: Pour application topique sur les ongles
des doigts, les ongles des pieds et les zones de peau voisines (périonyx, hyponychium). Appliquer une fois par jour en une couche mince. CI: Hypersensibilité
au ciclopirox ou à un des autres composants du médicament. Enfants de moins de 6 ans. Préc: En cas de survenue d’une réaction d’hypersensibilité le
médicament doit être arrêté. L’alcool cétylstéarylique peut provoquer des réactions cutanées locales telles que par exemple une dermite de contact irri-
tative. Grossesse et allaitement: l'utilisation n'est pas conseillée, à moins que cela ne soit absolument indispensable. EI: Très rarement: rougeur, desqua-
mation, brûlures et démangeaisons de la zone traitée. Prés: 3,3 ml et 6,6 ml. Liste: B, admis par les caisses-maladie. Avant la prescription, consulter le
Compendium Suisse des Médicaments. Astellas Pharma SA, Grindelstrasse 6, 8304 Wallisellen. Mise à jour de l'information: mai 2009. APCHCICIN0311fReferendum zur KVG-Revision über die integrierte
Gesundheitsversorgung (Managed Care) – Position der SGDV
Am 30.09.2011 hat das Schweizer Parlament die KVG- stellter Erwerbsfähigkeit, die allerdings schwer
Revision 04.062 über die integrierte Gesundheits- messbar und auswertbar ist
versorgung beschlossen, welches am 11.10.2011 • soll weiterhin liberalen Prinzipien gehorchend in
publiziert wurde. Ab diesem Moment läuft die Refe- einem regulierten Wettbewerb stattfinden kön-
rendumsfrist von 100 Tagen, die bis zum 19.01.2012 nen
dauert.
Zwei Antworten auf die Anliegen des "Managed Care-
Die Gesetzesrevision ist im Kontext von zwei grossen Gesetzes":
Themen zu sehen: • Die Kostensteigerung im Gesundheitswesen
• die gegenüber dem Bruttoinlandprodukt über- ist im Fundament unvermeidbar, aber sie kann
proportionale Zunahme der Gesundheitskosten modifiziert werden: In erster Linie muss der
• als Antwort auf die vom Parlament diskutierte Leistungskatalog der Grundversicherung regel-
Aufhebung des Kontrahierungszwangs gedacht mässig überprüft und gestrafft werden. Diese
Aufgabe müssen die Fachgesellschaften lösen.
Diese Gesetzesrevision beinhaltet im Wesentlichen: Es sind auch die Fachgesellschaften, welche die
• die Budget-Mitverantwortung der im Ärztenetz- "schwarzen Schafe" unter den Ärztinnen und
werk zusammengeschlossenen Ärztinnen und Ärzten zur Rechenschaft ziehen müssen.
Ärzte • Als Nachfolgekonzept des Kontrahierungszwangs
• den differenzierten Selbstbehalt für die Patien- bestehen mehrere valable Lösungen, welche die
tinnen und Patienten (finanzieller Anreiz, sich in Prinzipien des regulierten Wettbewerbs in einer
einem Ärztenetzwerk versichern zu lassen) liberalen Wirtschaftsordnung respektieren mit
• ein Verbot für die Krankenkassen, selber Ärzte- folgender Zielsetzung ; ÄrztInnen mit einer pro-
netzwerke zu betreiben funden Weiterbildung sollten bevorzugt werden,
und eine Überarztung der grossen Städte und
Die SGDV hat das Projekt von Anfang an bekämpft: «attraktiven» Grenzkantone vermieden werden.
• im Argumentarium während dessen Entstehung
• indem sie zusammen mit zwei weiteren Fachge- Praktische Aspekte der Unterschriften-Sammlung:
sellschaften und vier kantonalen Gesellschaften • die Unterschriften müssen bis zum 30.11.2011
die Urabstimmung zur "Motion Chaudhry" her- gesammelt sein. Die Gemeinden müssen jede
beiführte einzelne Unterschrift beglaubigen, was 2-3 Wo-
und sie wird sie weiter entschieden bekämpfen, in- chen beansprucht. Danach kommen die Festta-
dem sie : ge.
• die Unterschriften-Sammlung für das Zustande- • Wenn Ihre Praxis im Einzugsgebiet mehrerer
kommen des Referendums vorbehaltlos unter- Wohngemeinden liegt, müssen Sie darauf achten,
stützt dass pro Wohngemeinde ein Unterschriftenbo-
SGDV - SSDV
• den Abstimmungskampf aktiv mitgestalten wird gen verwendet wird. Es sollen nicht Personen
aus verschiedenen Wohngemeinden auf dem
Aus folgenden Gründen ist die Gesetzesrevision falsch gleichen Unterschriftenbogen unterzeichnen
konzipiert und daher zu bekämpfen: (wegen der Beglaubigung auf den Gemeinden).
• die Budget-"Mit"verantwortung wird im Laufe Wegen des Arztgeheimnisses empfiehlt es sich,
der Zeit in eine Budget-Vollverantwortung über- in der Praxis pro Person ein Blatt auszufüllen. Das
gehen Formular kann auch mit nur einer Unterschrift
• sie setzt einen starken Anreiz zur finanziellen eingereich werden !
Steuerung, anstelle einer Steuerung über die • Wir bitten Sie daher, bis zum 30.11.2011 wenn
Qualität irgend-möglich pro Dermatologische Praxis 100
• sie setzt einen starken Anreiz zur Rationierung Unterschriften zu sammeln, und einmal pro Wo-
der Medizin che die bislang gesammelten Bögen an folgende
• der differenzierte Selbstbehalt entspricht einer Adresse zu schicken:
Wettbewerbsverzerrung: Wenn Ärztenetzwerke • "Rererendums-Komitee freie Arztwahl für alle",
kosten-wirksamer arbeiten, werden sie sich von c/o fmCh-Generalsekretariat, Theodor Kocher-
selber durchsetzen Strasse 12, 2502 Biel/Bienne
• alle Ärztinnen und Ärzte arbeiten ohnehin in
Netzwerken Mehr Informationen: www.fmch.ch
• es ist eine anmassende Behauptung, dass sich
Ärztinnen und Ärzte im Gesundheitswesen wie in Herzlichen Dank für Ihre Unterstützung!
einem Selbstbedienungsladen bedienen würden. Freundliche kollegiale Grüsse
Die Medizin der Zukunft:
• wird wegen der Demographie und des medizini- Prof. Jürg Hafner, Präsident SGDV
schen Fortschritts nicht billiger werden Dr. Jean-Pierre Grillet, Past-Präsident
• schafft für die Gesellschaft einen grossen Mehr-
wert in Form von gewonnenen Lebensjahren,
gewonnener Lebensqualität und wiederherge-
12 Dermatologica Helvetica - Volume 23(9) - Novembre 2011Z: 1 g Pruri-med Lipolotion enthält: Ureum 50 mg, polidocanolum 600 30 mg. I: Hauterkrankungen mit trockener und/oder juckender Haut wie z.B. atopische Dermatitis und
Pruritus senilis. D: 2-3 mal täglich auftragen. UW: auf entzündeter Haut gelegentlich Brennen, Rötung. P: 200 ml* + 500 ml*. Liste D. Z: 1 g Pruri-med enthält: Polidocanolum 600
50 mg, disodium undecylenamido MEA-sulfosuccinate 30 mg. I: Therapieunterstützende, antipruriginöse Hautreinigung bei atopischer Dermatitis, Urtikaria, Pruritus senilis oder
sine materia. D: wie flüssige Seife anwenden. P: 150 ml* + 500 ml*. Liste D. Ausführliche Informationen siehe Arzneimittel-Kompendium der Schweiz. Permamed AG, CH-4106
Therwil, Tel. 061 725 20 20, Fax 061 725 20 40, e-mail: permamed@permamed.ch, www.permamed.ch, Pru/ins/D/12-10
200 ml (SL)
• Pruritus senilis
• Atopische Dermatitis
• 200 ml + 500 ml kassenpflichtig
und juckende Haut
Pruri-med Lipolotion
®
auch 500 ml
Die Oase für sehr trockene
• 5% Ureum
• 40% Lipide
kassenpflichtig (SL)
• 3% Polidocanol 600Référendum contre la révision partielle de la LAMal
concernant l’approvisionnement de soins intégrés (managed
care) – Position de la SSDV
En date du 30 septembre 2011, le Parlement suisse a forme d'années de vie gagnées, d'accroissement
adopté la révision partielle de la LAMal (objet 04.062) de la qualité de vie et du rétablissement de la ca-
concernant les soins intégrés (managed care), texte qui pacité de gain, ce qui est en réalité difficilement
a été publié le 11 octobre 2011. Dès cette date court le mesurable et évaluable
délai de référendum de 100 jours, qui prendra donc fin • doit pouvoir continuer à évoluer, conformément
au 19 janvier 2012. aux principes libéraux, dans le cadre d'une concur-
rence régulée.
Il y a lieu de considérer ce nouveau texte légal dans le
contexte de deux problématiques importantes: Deux réponses aux soucis qui ont motivé la "révision
• l'augmentation disproportionnée des coûts de la managed care":
santé par rapport au produit intérieur brut • l'augmentation des coûts du domaine de la santé
• un texte conçu à titre de réponse à la suppression est en principe incontournable, mais elle peut être
de la liberté de contracter discutée par le Parle- modifiée: en premier lieu, le catalogue des presta-
ment. tions de l'assurance de base doit être réexaminé et
Voici les grands traits du contenu de la révision de la allégé régulièrement. Les sociétés de disciplines
loi: médicales doivent faire ce travail. Il faut également
• la co-responsabilité budgétaire des médecins affi- contraindre les sociétés de disciplines médicales
liés à un réseau qui sont des "moutons noirs" de rendre des comp-
• la franchise différenciée pour les patient-e-s (inci- tes.
tation financière à se faire assurer dans le modèle • Une régulation du nombre de médecins dans cer-
dun réseau de médecins) taines régions paraît incontournable. Plusieurs pos-
• une interdiction faite aux caisses-maladie dexploi- sibilités raisonnables pourraient être envisagées
ter elles-mêmes des réseaux de médecins. pour remplacer la clause du besoin. Idéalement,
il s’agit de solutions qui répondent aux principes
La SSDV a combattu dès le départ le projet de révision: d’une concurrence réglementée dans le respect
dans l'argumentaire pendant l'élaboration de ce projet d’un système économique libéral. Celui-ci devrait
• en organisant, en collaboration avec deux autres d’une part avantager les médecins avec une for-
sociétés de disciplines médicales et quatre socié- mation post-graduée approfondie et d’autre part
tés cantonales, la votation générale relative à la restreindre (ou éviter) une surdensité et une sur-
"Motion Chaudhry". médicalisation dans les grandes villes attractives et
• et elle continuera à se battre avec détermination leur périphérie.
contre le nouveau texte légal:
• en soutenant sans réserve la récolte de signatures Aspects pratiques de la récolte de signatures:
pour que le référendum aboutisse • les signatures doivent être collectées jusqu'au
• en participant activement à la campagne précé- 30.11.2011. Les communes doivent authentifier
dant le vote du peuple. chaque signature, ce qui prend 2 à 3 semaines. Puis
il faut y ajouter la période des fêtes.
La révision de la loi est mal conçue et doit donc être • Si votre cabinet se trouve dans la zone de desser-
combattue pour les motifs suivants: te de plusieurs communes, vous devez veiller à
• la "co"-responsabilité budgétaire deviendra au fil ce que soit utilisée une feuille de signatures par
du temps une pleine responsabilité budgétaire commune. Des personnes résidant dans des com-
• elle crée une forte incitation au pilotage financier munes différentes ne peuvent pas signer sur la
au lieu d'un pilotage de la qualité même feuille (en raison de l'authentification par
• elle incite fortement au rationnement de la méde- les communes). Pour des raisons de secret médical,
cine nous vous conseillons d’utiliser une feuille par per-
• la franchise différenciée équivaut à une distorsion sonne dans les cabinets. La feuille n’a pas besoin
de concurrence: si des réseaux de médecins tra- d’être pleine pour être renvoyée !
vaillent plus efficacement sous l'angle des coûts, • Nous vous prions donc de réunir, autant que faire
ils vont s'imposer d'eux-mêmes se peut, 100 signatures par cabinet de dermatolo-
• tous les médecins travaillent de toute façon en ré- gie d'ici le 30.11.2011 et d'adresser une fois par se-
seaux maine les feuilles récoltées à l'adresse suivante:
• il est présomptueux d'affirmer que les médecins se "Rererendums-Komitee freie Arztwahl für alle", c/o
servent, dans le domaine de la santé, comme dans fmCh-Generalsekretariat, Theodor Kocher-Strasse 12,
un magasin self-service. 2502 Biel/Bienne.
Plus d'information: www.fmch.ch
La médecine à l'avenir:
• ne sera pas moins chère en raison de l'évolution Un tout grand merci pour votre soutien !
SGDV - SSDV
démographique et des progrès de la médecine Avec nos salutations cordiales et collégiales,
• crée pour la société une forte valeur ajoutée sous
Prof. Jürg Hafner, Président SSDV Dr Jean-Pierre Grillet, Past-Président SSDV
14 Dermatologica Helvetica - Volume 23(9) - Novembre 2011PROCES-VERBAL
de la 93e Assemblée générale de la SSDV
Vendredi 2 septembre, de 17h30 à 19h00
Starling Hotel, Genève
Intervenants jusqu’en 2018. L’assemblée remercie par applaudis-
sements le Dr Bloch pour cette prestation.
Dr Jean-Pierre GRILLET Président Par ailleurs, le président a très à cœur de remettre
Prof. Jürg HAFNER Président elect la médecine en tant que telle au premier plan et
Dresse Rosmarie HOLZINGER Trésorière de ne pas laisser la bureaucratie prendre la main. "Il
n’y a pas une grande et une petite médecine – il y
Procès-verbal a LA médecine".
Le président s’exprime sur les thèmes brûlants sui-
Monica PONGRATZ Secrétaire vants de la politique de la santé:
générale SSDV
- Dr J. De Haller – candidat au Conseil national
Participants Le président considère que le président de la FMH
ne devrait pas se porter candidat au Conseil natio-
53 membres de la SSDV points 1 à 10 de nal. Il attend d’une association faîtière une position
l'ordre du jour apolitique et se demande si la FMH n’encourt pas
43 membres de la SSDV points 11 à 28 de le danger de devenir à l’avenir un sous-groupe du
l'ordre du jour PS.
1. Approbation de l’ordre du jour du 2 septembre - Réseaux de soins intégrés
2011 Les réseaux de soins intégrés prévus apparaissent
Le président salue les membres. L'ordre du jour est aux yeux du président comme une tentative de so-
approuvé. lution inadaptée à un problème mal posé. Vouloir
régler la question du financement par des influen-
2. Election des scrutateurs ces exercées sur les coûts lui semble être une ap-
La Dresse Françoise Balsiger et la Dresse Mouna proche totalement erronée. A son avis, les réseaux
Skaria sont désignées scrutatrices. 53 membres de de soins prévus liés par une co-responsabilité bud-
la SSDV sont présents. gétaire vont plutôt générer une limitation de l’ac-
tivité médicale que favoriser son épanouissement !
3. Approbation du procès-verbal de la 92e As- Ces réseaux seront totalement dépendants d’insti-
semblée générale de la SSDV du 27 août à Zurich tutions financières telles que les caisses-maladie et,
Le procès-verbal de la dernière Assemblée généra- comme on l’a vu très récemment, de Migros égale-
le est approuvé. Mme Pongratz est remerciée pour ment.
le procès-verbal. La FMH a soutenu de tout temps le projet Managed
care. En principe, il n’y a rien à objecter à celui-ci,
4. Présentation des nouveaux membres SSDV sauf que le Parlement l’a tellement modifié dans
2010/2011 ses points essentiels qu’il en devient insoutenable
Les nouveaux membres suivants 2010/2011 pren- pour les spécialistes. Concrètement, il s’agit: - de
nent part à l’AG et sont présentés à la société: la franchise différenciée et de la co-responsabilité
Membres ordinaires: Prof. Gilliet, Dr Donghi, Dr Du- budgétaire liée à ces réseaux de soins. Il est à crain-
chini, Dr Hauser, Dr Kristof, Dr Weibel dre qu’à l’avenir, la médecine ne se fonde plus que
Membres extraordinaires: Dr Bull, Dr Keller sur des critères économiques et ne prenne plus en
compte le bien des patients.
5. Mots d’introduction du président et politique Lors de la Chambre médicale (CM) du 26 mai, un
professionnelle vote a eu lieu pour déterminer si la FMH s’oppo-
Le président entame son introduction en remer- sait au projet du Parlement ou le soutenait. Dans
ciant les personnes et organes qui l’ont soutenu et son premier vote, la CM s’est clairement exprimée
accompagné tout au long de son mandat. En font à l’encontre du projet actuel. Mais dans l’après-
partie au niveau de la discipline spécifique: Prof. midi, un nouveau vote a été exigé, dont le résultat
SGDV - SSDV
Laugier et Prof. Saurat, et au plan de la politique a abouti à la position contraire. En conséquence,
professionnelle: Dr Aubert, Dr Chavaz, Dr Gabbud, un groupe composé des sociétés cantonales de
Dr Gueissaz, Dr Hofer, Dr Ramelet, Dr Tapernoux et, médecine et des sociétés de disciplines médicales
à l’échelon de la SSDV, les membres du Bureau du a été constitué, qui a exigé un scrutin général afin
Comité, les membres du Comité ainsi que la secré- de faire voter l’ensemble du corps médical sur ce
taire générale. Un merci spécial va également au thème important.
Dr Bloch. Il a très notablement contribué à l’élabo- Le président, soutenu par le comité de la SSDV,
ration de notre programme de formation postgra- recommande aux membres d’approuver le texte
duée pour la dermatologie et la vénérologie. Notre de la votation générale. Plus nombreuses seront
programme a été récemment réaccrédité par le DFI les voix qui rejetteront le projet de loi, plus la FMH
Dermatologica Helvetica - Volume 23(9) - Novembre 2011 15Sie können auch lesen

















































