Endometriosis research at the University Hospital in Bern - more than 10 years of Inter national Collaboration - SGGG
←
→
Transkription von Seiteninhalten
Wenn Ihr Browser die Seite nicht korrekt rendert, bitte, lesen Sie den Inhalt der Seite unten
u
fo m
3 2011
gynécologie suisse
Endometriosis
research at the University
Hospital in Bern – more
than 10 years of Inter
national Collaboration
Pratiques médicales et formation continue
La salpingectomie permet-elle d’éviter le cancer
de l’ovaire ?
Leben der Gesellschaft
Der Jahreskongress 2011 im Rückblick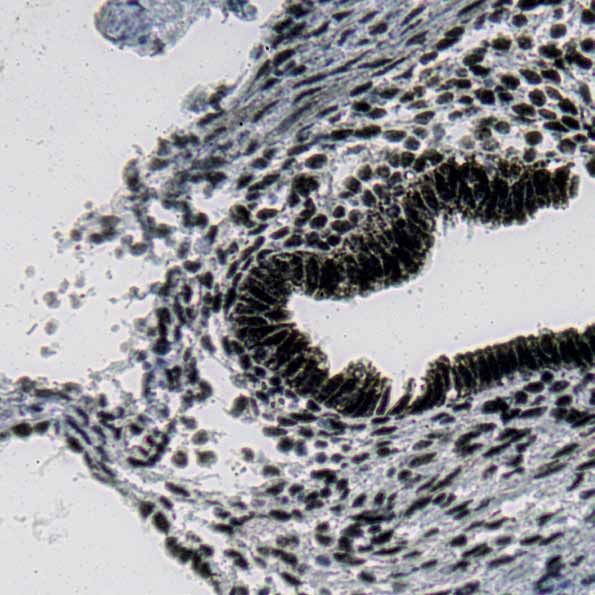
Körperidentische Hormone. Körperidentische Hormone gegen menopausale Beschwerden1. Die Kombination von transdermalem 17β-Estradiol und mikronisiertem Progesteron zeigt keine Evidenz für ein erhöhtes Brustkrebs- und Thrombose-Risiko2-5. 1. Arzneimittelkompendium der Schweiz; http://www.kompendium.ch 2. Fournier A et al. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int. J. Cancer 2005; 114: 448-454 3. Fournier A et al. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008; 107(1): 103-11 4. Espie M et al. Breast cancer incidence and hormone replacement therapy: results from the MISSION study, prospective phase. Gynecological Endocrinology, 2007; 23(7): 391-397 5. Canonico M et al. Hormone therapy and venous thromboembolism among postmenopausal women: Impact of the route of estrogen administration and progestogens: The ESTHER study. Circulation 2007; 115: 840-845 Estradot® 25/37,5/50/75/100® Z: Transdermales Pflaster (DOT), das 25, 37.5, 50, 75 oder 100 µg/24 h Estradiol abgibt. Excip. ad praep. I: Behandlung der Symptome des Estrogenmangels infolge der natürlichen od. künstlichen Menopause. Vorbeugung od. Verzögerung einer durch Estrogenmangel induzierten Osteoporose bei postmenopausalen Frauen mit hohem Frakturrisiko, für die eine Behandlung mit anderen zur Prävention der Osteoporose zugelassenen Arzneimitteln nicht in Frage kommt, od. bei Frauen die gleichzeitig an behand- lungsbedürftigen Symptomen des Estrogenmangels leiden. Bei Frauen mit intaktem Uterus muss die Estrogensubstitution stets mit einem Gestagen ergänzt werden. D: Applikation alle 3 – 4 Tage. Niedrigst wirksame Dosierung anwenden, so kurz wie möglich behandeln. Einzelheiten: s. Kompendium. KI: Bekannter od. vermuteter Brustkrebs, bekannter od. vermuteter Endometriumkarzinom od. andere estrogenabhängige Neoplasie, diagnostisch nicht abgeklärte abnormale Vaginalblutung. Schwere Lebererkrankung. Dubin-Johnson-Syndrom u. Rotor-Syndrom, frühere od. bestehende venöse thromboembolische Erkrankungen (z. B. tiefe Venenthrombose, Lungenembolie), bekannte Gerinnungsstörungen od. Thrombophlebitis, frühere od. bestehende arterielle thromboembolische Erkrankungen (z. B. Angina pect., Myokardinfarkt, Schlaganfall), Porphyrie, bekannte Überempfindlichkeit gegen Estrogene od. gegen andere Bestandteile von Estradot, bekannte od. vermutete Schwangerschaft, Stillzeit. VM: Nicht zur Prävention kardiovaskulärer Erkrankungen einsetzen; erhöhtes Risiko für venöse Thromboembolie (z. B. tiefe Venenthrombose od. Lungenembolie). Chirurg. Eingriffe, längere Immobilisation. Erhöhtes Brustkrebsrisiko. Monotherapie mit Estrogen: erhöhtes Endometriumkarzinom-Risiko bei Frauen mit intaktem Uterus. Restendometriosen. Diagnostisch nicht abgeklärte persistierende vaginale Blutungen od. Spotting. Langandauernde Estrogenmonotherapie erhöht das Risiko von Endometriumkarzinomen, wenn die Behandlung nicht durch sequenzielle Gestagentherapie ergänzt wird. Erhöhtes Risiko für die Entwicklung eines Ovarialkarzinoms. Demenz. Therapie sofort absetzen bei: Gelbsucht, Verschlechterung der Leberfunktion, signifikanter Blutdruckanstieg, Neuautreten von migräneartigen Kopfschmerzen, Schwangerschaft od. falls eine der unter »KI« genannten Bedingungen eintritt. Flüssigkeitsretention möglich. Hypertriglyzeridämie, Diabetes. Kontaktsensibilisierung, schwere Überempfindlichkeitsreaktion. Sorgfältige Nutzen/Risiko-Abwägung bei Einsatz von Osteoporoseprophylaxe. IA: Präparate, welche arzneistoffmetab. Enzyme induzieren, insb. Cytochrom P450 Enzyme. Antikonvulsiva, Meprobamat, Phenylbutazon, Antiinfektiva. Proteaseinhibitoren, Johanniskraut. UW: Sehr häufig: Spannungsgefühl in den Brüsten, Reaktionen an der Applikationsstelle nach Entfernen des Pflasters. Häufig: Depression, Kopfschmerzen, Migräne, Benommenheit, Nausea, Bauchschmerzen, Blähungen. Blutungsanomalien, Fluor vaginalis, Brustvergrösserung, Gewichtsveränderung, Oedem, Juckreiz und Ausschlag um die Applikationsstelle herum, Gelegentlich: Brust- krebs, Erbrechen, Alopezie, Hirsutismus, genitale Candidiasis, uterines Leiomyom, veränderte Libido. Selten und sehr selten: s. Arzneimittelkompendium. Liste B. Detaillierte Informationen: Arzneimittelkompendium der Schweiz oder www.documed.ch. Zulassungsinhaberin: Novartis Pharma Schweiz AG, Bern. Oestrogel® Z: 17β-Estradiol. I: Östrogenmangel-Symptome als Folge der Menopause. Prophylaxe der Osteoporose bei menopausalen Patientinnen. D: Niedrigste wirksame Dosierung anwenden, so kurz wie möglich behandeln. Täglich 1 Dosierungsmass oder 2 Hübe Oestrogel® (1.5 mg Oestradiol) auf Schultern und Arme applizieren. Die Dosierung muss individuell angepasst werden. Maximaldosierung: 5 g Gel/Tag. Bei Frauen mit intaktem Uterus durch eine Gestagentherapie ergänzen. Kl: Mamma- oder Endometriumkarzinom, nicht behandelte Endometriumhyperplasie, nicht abgeklärte Vaginalblutungen, schwere Leberschäden, thromboembolische Störungen, Porphyrie, Überempfindlichkeit gegen Bestandteile, Schwangerschaft und Stillzeit. VM: Überwachung von Patientinnen mit einem Risiko von östrogenabhängigen Tumoren oder thromboembolischen Erkrankungen, Leiomyomen, Hypertonie, Lebererkrankungen, Epilepsie, Migräne, Diabetes, Endometriose, generalisierter Lupus erythematodes, Asthma, Otosklerose, Sichelzellanämie, Herz- oder Nieren- insuffizienz, Ödemen, andauernde Blutungen, Tetanie und multipler Sklerose. Therapie sofort absetzen bei: Verschlechterung der Leberfunktion, Blutdruckanstieg, Wiederauftreten von Migräne, Schwangerschaft, venöse Entzündungen, grösserer Gewichtszunahme, Augen -oder Ohrenerkrankungen, koronareren Herzkrankheiten und Schlaganfall. IA: Antikonvulsiva, Antiinfektiva, Protease-Hemmer, Johanniskraut. UW: Gelegentlich: Hautververänderungen, Vaginalfloraveränderung, Metrorrhagie, Endometriumhyperplasie, Spannungsgefühl in den Brüsten, Kopfschmerzen, Migräne, Oedeme und/oder Gewichtsveränderungen. Selten: Mastopathie, Brechreiz, Bauchkrämpfe, Blähung, Gallenlithiasis, Schwindel. Erhöhtes Risiko für Brustkrebs, Endometriumskarzinom und thromboembolische Störungen. Liste B. Detaillierte Informationen: Arzneimittelkompendium der Schweiz oder www.documed.ch. Zulassungsinhaberin: Vifor AG, CH-1752 Villars-sur-Glâne. Utrogestan® Z: Progesteron. I: Orale Verabreichung: prämenstruelles Syndrom, Menstruationsstörungen, Prämenopause, Menopause. D: Prämenstruelles Syndrom, unregelmässige Menstruation: 200 mg bis 300 mg/Tag während 10 Tagen. Menopause: 200 mg/Tag in Kombination mit einem Östrogen während 12 bis 14 Tagen des Zyklus. Kl: Lebertumor, Leberleiden, Rotor- oder Dubin-Johnson-Syndrom, Genitalblutungen ungeklärter Ursache, Porphyrie, arteriell oder venösen thromboembolischen Störungen, Hirnblutungen, Neoplasien der Brust oder der Geschlechtsorgane, Herpes gestationis, Überempfindlichkeit auf Inhaltsstoffe der Kapseln oder Erdnussallergie. VM: Jährliche gynäkologische Untersuchung, Mammographie. Abklärung der ausgiebigen oder unregelmässigen genitalen Blutungen. Sofortige Einstellung der Behandlung: thrombo-embolische oder thrombo-phlebitischer Prozesse, cerebrale Apoplexie, Ikterus, Blutdruckerhöhung, generalisierten Pruritus, abnormale Leberparameter, Hepatomegalie, Lebertumor, Myom, schwere depressive Zustände. IA: Barbiturate, Antiepileptika, Rifampicin, Phenylbutazon, Spironolakton, Griseofulvin, Ampicillin, Tetrazykline, Antidiabetika, übermässiger Tabakkonsum, Alkoholmissbrauch. UW: Orale Verabreichung: Häufig: Amenorrhöe, Verminderung des menstruales Zyklus, unregelmässige Blutungen, Kopfschmerzen. Gelegentlich: Mastodynie, Schläfrigkeit, Schwindel, cholestatische Ikterus, Hautstörungen, gastrointestinale Störungen. Selten: Gewichtsschwankungen, Veränderung der Glukosetoleranz, anaphylaktischer Schock. Depression. Liste B. Detaillierte Informationen: Arzneimittelkompendium der Schweiz oder www.documed.ch. Zulassungsinhaberin: Vifor AG, CH-1752 Villars-sur-Glâne. Vifor SA, Route de Moncor 10, 1752 Villars-sur-Glâne 1, Telefon 058 851 61 11, www.viforpharma.com Novartis Pharma Schweiz AG, 3001 Bern, Telefon 031 377 31 11, www.novartispharma.ch

I N H A LT _ S O M M A I R E
Editorial
02 Le Röstigraben : une opportunité à saisir !
03 Der Röstigraben als Chance!
Wissenschaft _ Sciences
04
Endometriosis Research at the University Hospital in Bern –
a Report on more than 10 years of International Collaboration
Praxis und Fortbildung _ Pratiques médicales et
formation continue
10 L a salpingectomie permet-elle d’éviter le cancer de l’ovaire ?
14 Als Ärztin und Hebamme in der Republik Moldawien
18 Le réseau romand de formation post-graduée en gynécologie et
obstétrique (RRFGO)
20 Roma 2011: 13th World Congress on Menopause
Leben der Gesellschaft _ Société
22
Mi hanno detto che sembro una mamma vera …
26
Rückblick auf den Jahreskongress 2011 in Lugano
Impressum
Herausgeberin _ Editeur Schweizerische Gesellschaft für Gynäkologie und Geburtshilfe, gynécologie suisse
Redaktionskommission _ Commission de la rédaction Felix Adank, forum pr Bern, adank@forumpr.ch;
Fadhil Belhia, Lausanne, fbelhia@bluemail.ch; Regula Bürki, Bern, regula.buerki@hirslanden.ch; Claudia Canonica,
Zürich, claudia.canonica@usz.ch; Stefan Gerber, Fribourg, gerberstefan@bluewin.ch; Irene Hösli, Basel, ihoesli@uhbs.ch;
Patrick Petignat, Genève, patrick.petignat@hcuge.ch; David Stucki, Fribourg, dstucki@cliniquegenerale.ch; Edi Vlajkovic,
Zürich, eduard.vlajkovic@spitalzollikerberg.ch | Vorsitz und Koordination _ Présidence et coordination Christiane
Roth, Gockhausen, info@christiane-roth.ch | Redaktion der französischen Artikel _ Edition des articles en français
Sylvie Logean, Lausanne | Gestaltung _ Mise en page atelierrichner.ch | Druck _ Impression Stämpfli Publikationen AG,
Bern | Papier weiss halbmatt gestrichen 115 g/m2, holzhaltig _ couché blanc demi-matt 115 g/m2 | Auflage _ Tirage 1800
Titelbild _ Page de couverture Forschungslabor Universitätsfrauenklinik Bern
EDITORIAL
Le Röstigraben : une opportunité à saisir !
Der Röstigraben als Chance!
L’expression Röstigraben (barrière de Rösti) est très souvent employée dans les médias
pour exprimer l’opposition de la Suisse francophone par rapport à la Suisse germano-
phone, concernant différents thèmes, aussi bien culturels, économiques, que politiques.
Cette expression signifie qu’il y a une profonde incompréhension entre les deux parties
principales de la Suisse et que la recherche de solutions communes semble impos-
sible. Est-ce bien le cas ?
Ayant vécu toute ma jeunesse à Fribourg, ville bilingue, je pense que cette cohabitation
de différentes cultures, de différentes mentalités, de différentes sensibilités, complé
mentaires, est une richesse qui permet à la Suisse de trouver des solutions originales,
dans le respect de chaque citoyen-ne suisse.
La Suisse s’est construite lentement. Tout au long de notre histoire, les politiciens ont
toujours tenté, sur le plan fédéral, de trouver des solutions dans un esprit de compro-
mis : le fameux consensus suisse. Cela prenait du temps, mais chacun y trouvait son
compte et la Suisse est ainsi devenue, progressivement, dans de nombreux domaines,
un pays fort, respecté, sur le plan international.
La Société suisse de gynécologie et obstétrique est une société dynamique, moderne
et performante, qui a montré l’exemple aux autres sociétés de spécialistes suisses
dans de nombreux domaines.
Parmi ses membres, on retrouve les différences linguistiques, culturelles, de formation,
qui font que chacun-e de nous a ses références. La confrontation d’idées qui résulte
de cette diversité doit être considérée comme une opportunité pour trouver des solu-
tions efficaces, qui nous permettent de progresser et de nous adapter aux nouvelles
exigences de la société moderne. Pour cela, il faut discuter, comparer nos thèses,
élaborer des compromis, dans un esprit de tolérance. Durant les dernières années,
le Comité central a opéré des modifications radicales dans les structures de la société,
pour les moderniser. Sous l’influence de notre nouvelle Secrétaire générale, nous
avons centralisé à Berne le secrétariat de la société suisse, ainsi que différentes séances
de comité. Cela renforce l’équilibre entre les régions.
Actuellement, chacun-e parle sa langue, mais nous pourrions aussi opter pour l’an-
glais, puisque la Suisse s’internationalise. Dans les prochaines années, la Société suisse
de gynécologie et obstétrique sera confrontée à de nombreux défis: le Tarmed, les DRG,
le monitorage de la qualité en ambulatoire, la formation continue, la relève, la struc-
ture de notre société, l’avenir de notre profession, les relations avec la FMH et la fmCh.
Le Comité central s’y prépare, avec vous et pour vous.
Nous avons un métier formidable, celui de promouvoir et de veiller à la santé de
la femme. Pour continuer à le pratiquer dans de bonnes conditions et être en mesure
d’accomplir notre mission, nous devons travailler ensemble à trouver des solutions
pragmatiques, équilibrées et solidaires, dans un esprit de tolérance et dans le respect
de nos différences.
Je suis persuadé que, tous ensemble, nous réussirons !
Dr Jacques Seydoux
Président SSGO
02 forum gynécologie suisse 3 | 11
Der Begriff Röstigraben wird in den Medien modernisiert, die Gesellschaft hat sich neue
oft verwendet, um kulturelle, ökonomische Strukturen gegeben. So hat die neue General
und politische Gegensätze zwischen Deutsch sekretärin dem Vorstand vorgeschlagen, das
schweiz und Westschweiz zum Ausdruck zu Sekretariat nach Bern zu verlegen, wo heute
bringen. Der Begriff deutet auf ein tiefgreifen auch die meisten Sitzungen stattfinden. Dies
des Unverständnis zwischen den beiden ermöglicht ein neues Gleichgewicht zwischen
wichtigsten Sprachregionen der Schweiz – den Regionen, weil die Erreichbarkeit für alle
der Röstigraben hindert uns angeblich daran, etwa gleich ist. Heute spricht noch jede und
gemeinsam nach Lösungen zu suchen. Ist das jeder in seiner Sprache. Mit der zunehmenden
wirklich so? Globalisierung könnten Deutsch und Fran
Ich habe meine Jugend im zweisprachigen zösisch durch die englische Sprache abgelöst
Freiburg verbracht. Das Zusammenleben von werden.
Menschen unterschiedlicher Kulturen, Menta In den kommenden Jahren wird sich gynéco
litäten und Sensibilitäten hat mich geprägt logie suisse zahlreichen Herausforderungen
und mir bewusst gemacht, dass diese Unter stellen müssen: TARMED; SwissDRG, Qualitäts
schiede einen Reichtum darstellen, der es uns monitoring in der ambulanten Medizin, die
Schweizern ermöglicht, unter Wahrung des ärztliche Fortbildung, der Nachwuchs, die
gegenseitigen Respekts eigenständige Lösun Struktur der Gesellschaft, die Zukunft unseres
gen zu finden. Berufs sowie die Beziehungen zur FMH und
Die Schweiz ist langsam entstanden. Die Ge zur fmCh werden uns weiterhin beschäftigen.
schichte zeigt, dass die eidgenössischen Poli Der Vorstand bereitet die Zukunft vor, für Sie
tiker schon immer versucht haben, konsens und zusammen mit Ihnen.
fähige Lösungen zu finden, nach dem Prinzip Die Gesundheit der Frau zu fördern und für
des guteidgenössischen Kompromisses. Das sie zu sorgen ist eine wundervolle Aufgabe.
brauchte Zeit, aber alle kamen auf ihre Rech Damit wir unseren Beruf auch in Zukunft unter
nung. Die Schweiz ist so in vielen Bereichen guten Bedingungen ausüben können, müssen
nach und nach zu einem starken, auch inter wir zusammen nach pragmatischen, ausge
national anerkannten und respektierten Land wogenen und solidarischen Lösungen suchen.
geworden. Dies in einem Geist von Toleranz und gegen
Gynécologie suisse ist eine dynamische, mo seitigem Respekt. Gemeinsam werden wir es
derne und leistungsfähige Fachgesellschaft, die schaffen!
anderen Fachgesellschaften in vielen Bereichen
beispielhaft vorangegangen ist. Ihre Mitglieder
sind sprachlich, kulturell und in der fachlichen
Ausrichtung unterschiedlich. Entsprechend ist
auch das Bezugssystem verschieden. Dies müs
sen wir als Chance nutzen für die Suche nach
Lösungen, die uns weiter bringen und helfen,
uns an die Anforderungen der modernen Gesell Dr. Jacques Seydoux
schaft anzupassen. Um Kompromisse zu finden, Präsident
braucht es das Gespräch und eine konstruktive
Diskussion, die von Toleranz geprägt ist. In den
vergangenen Jahren wurde gynécologie suisse
03 forum gynécologie suisse 3 | 11
SCIENCES
Endometriosis Research at the University
Hospital in Bern – a Report on more than
10 years of International Collaboration
Endometriosis is a common gynecological disorder defined by the presence, growth
and invasion of endometrial tissue outside the uterine cavity. Despite growing numbers
of hypotheses, the etiology of the disease remains an enigma. Our laboratory and others
have demonstrated that environmental factors might play an important role (1). Endo-
metriosis is a fascinating disease, as it is benign but behaves like a cancer. More than ten
years ago our laboratory started to look at different, histopathological (2, 3) as well as
clinical (4, 5) aspects of the disease and different international collaborations took place
in these years. Data suggest that an aberrant immunologic response is involved in the
pathophysiology of endometriosis (3) and that endometriosis may be seen as a local pel-
vic inflammatory process. In recent years, different studies have stressed the importance
of the peritoneal environment in the implantation, leukocytic infiltration and proliferation
of ectopic endometrial implants (3, 6, 7, 8) Although pelvic fluid is a complex medium
containing and influenced by multiple cell types, we among others have found this to be
a useful biological fluid to define intercellular mediators of the local reactions associated
with endometriosis. In recent years, part of our research focussed on the etiology of pain
in patients with endometriosis.
Prof. Nick A. Bersinger, Ph. D., Brett McKinnon, Ph. D., Alessandro Santi, M. D., Prof. Michel Mueller
Endometriosis, inflammation and pain against IGF binding proteins which, as a consequence,
Correlations between the morphologically assessed could result in higher levels of available growth fac-
severity of the disease and the peritoneal fluid (PF) tors (IGF) and thus explain the result.
concentration of pro-inflammatory cytokines and
other potentially immunoregulatory substances or
growth factors have been demonstrated by several No correlation between
groups as well as by ourselves (3, 6, 7, 8). These mol-
ecules include the key cytokines TNF-α and IL-8, but severity of pain and disease
Prof. Nick A. Bersinger
also Regulated on activation, normal T-cell expressed stage or known
and secreted (RANTES), epithelial neutrophil activat-
ing peptide-78 (ENA-78), midkine (a newly described inflammatory markers.
multifunctional growth factor), monocyte chemot-
actic protein-1 (MCP-1), and osteoprotegerin (OPG). As said above, pain is a major issue in endometriosis
Due to the often small numbers of women involved and its treatment. Unfortunately, however, a clear re-
in the different reports and the clinical heterogeneity lationship between the extent of pain experienced
(menstrual cycle, medication, etc.) of the study by the patients and either the severity of the disease
groups, it is not surprising that the results in the lit- or the concentration of a given cytokine, in the se-
erature remain largely inconsistent. Pregnancy-asso- rum or peritoneal fluid, could not be clearly demon-
ciated plasma protein A (PAPP-A) deserves a special strated to date. Major reports describe the associa-
note. It has entered routine application as a first tri- tion between the pain level and the morphological
mester maternal serum screening marker for fetal score (rAFS) of the disease as either absent or very
chromosomal abnormalities, but has never been weak, and this although intraneural and perineural
Prof. Michel Mueller
studied in the context of endometriosis. We have invasion by nodules of endometriosis is clearly asso-
found increased PF concentrations for PAPP-A in ciated with severe pain. The same is the case for the
women with the disease (8). Its biological role is still correlation between pain and the measured concen-
unclear, but it has a proteolytic activity directed trations of the currently known substances (cytokines,
04 forum gynécologie suisse 3 | 11
growth factors or others) – the «miracle» marker has – Identification of new peritoneal fluid and serum
not been identified yet. In a recent project with a markers using novel technology such as low-den-
comparatively small number of cases, however, we sity protein arrays (dot blots, Luminex® multiplex
have observed a trend towards increased PF concen- ELISA) and in defined patient groups as a function
trations of the above mentioned TNF-α, RANTES, and of menstrual cycle stage, endocrinology and
OPG (8). A much more pronounced association with medication (Collaboration with the Universities
menstrual pain (dysmenorrhoea) was found for gly- of Montpellier, France and Ljubljana, Slovenia);
codelin (or PP14; the abbreviation is still in use) (9), a – Investigation of neurogenic (in the end pain pro-
gestagen-dependent endometrial protein produced moting) effects in endometriosis, using in vitro
by the glandular epithelium and which has also been models (culture of neuronal cells in presence and
shown to be angiogenic. Endometrial glycodelin absence of PF from case and control women)
production is upregulated by dioxin (1). and assessment of neuronal tissue induction and
proliferation (11). Determination of promoting
In addition to the heterogeneity of the patient groups, factors by molecular biological (RNA extraction
the measurement of pain, as it is performed in our and RT-QPCR) at the transcriptional and by immu-
own as well in many other clinics and for different nohistochemical (protein expression at the trans-
applications, is subjective. We are using the Visual lational level) methods in collaboration with the
Analogue Scale (VAS) with a range between 0 (no University of Sydney, Australia. The main objective
pain) and 10 (strong, unbearable pain). The result is is the identification of the missing link. between
not a mathematical one like it would be in an electro- endometriosis and the pain generation, and thus
physiological measurement, but it is reflecting what the development of treatment lines targeting
the patient actually feels and can still be parametrised. specific cells or molecules.
Moreover, it can be divided into different types of
pain, such as menstrual (cycle dependent, dysmenor- A better understanding of the pathophysiology of en-
rhoea), generalized lower abdominal pain, dyspareu- dometriosis will help to identify new possible thera-
nia (pain limited to sexual activity), and others. peutical pathways for a more targeted therapy of en-
dometriosis (12). This is another focus of our laboratory,
In a close collaboration with the Anesthesiology the latest findings are summarized hereafter.
Department of the University of Berne, we recently
demonstrated evidence for widespread expansion New research objectives in endometriosis
of reflex receptive fields in endometriosis patients. Endometriosis is essentially estrogen dependent and
It thereby identifies a mechanism involved in central the induction of a hypo-estrogenic state is currently
hypersensitivity in chronic pain associated with en- the standard treatment for the control of symptoms.
dometriosis (10). Reverting the expansion of nocice- Unfortunately, side effects and adverse reactions to
ptive receptive fields and exploring the prognostic such treatment are common. Moreover, as endome-
meaning of this phenomenon may become future triosis is a disease of reproductive age women, the
targets of clinical research. treatment is often required to specifically target either
the occurrence or the development of the disease
Our research efforts towards a better characterisation without unduly affecting fertility. New medical treat-
of endometriosis-dependent pain and its treatment ments are thus required.
involve several sub-projects and collaborations:
– Comparison between subjective (VAS) and objec-
tive (electrophysiological) pain assessment and
the association of these results with the severity Diabetes drugs show promise
of endometriosis and the cytokine concentrations in treatment of endometriosis.
in the peritoneal fluid (Collaboration: Anesthesiol-
ogy and Pain Therapy, University of Berne);
05 forum gynécologie suisse 3 | 11
SCIENCES
A class of drugs known as Thiazolidinediones (TZD) we found no correlation with the expression of cy-
currently used to treat Type II diabetes (Glustin/Actos tokines, but we did find that the higher the number
and Avandia) has recently shown promise in treating of cells in the endometriotic lesion that express
pain, as well as reducing the lesion size itself. In a PPAR-γ, the more severe pain in the abdominal re-
clinical trial Rosiglitazone reduced the pain experi- gion and dyspareunia was reported by the patients
enced by women with endometriosis whereas both (Fig. 1C) (14). The relationship between PPAR-γ and
Rosiglitazone and Ciglitazone reduced the size of the pain is intriguing. Several studies have shown that
endometriotic lesion in animal models (13). Although PPAR-γ agonists were neuroprotective, most po-
already on the market for type II diabetes treatment, tently in ischemic injury, by reducing inflammation
the mechanism of action of these drugs is still con- and the generation of free radicals. It is therefore
troversial, with some analogues being withdrawn possible that the relationship between pain and
due to potential side effects. To assess the utility of PPAR-γ expression in endometriotic lesions is related
these drugs for endometriosis treatment while main- to its ability to facilitate an environment that can sus-
taining fertility, we performed studies on both the tain new innervations
ectopic endometriotic lesions and in vitro eutopic
endometrial cell models. Increasing evidence is beginning to show that neu-
rogenic factors are present in endometriosis. In mac-
Classically, it is thought TZDs target a nuclear tran- rophages, research has shown a cross talk exists
scription factor known as peroxisome proliferator- between PPAR-γ and the neurogenic receptor neu-
activated receptor gamma (PPAR-γ). PPAR-γ is known rokinin 1 (NK1), which is involved in the regulation of
to regulate the expression of inflammatory cytokines,
and this inhibition of inflammatory cytokine produc-
tion may be responsible for the reduction in lesion Bernese team finds that
size. We examined endometriotic lesions for PPAR-γ
expression by immunostaining (Fig. 1) and compared
neurogenic factor NK1 may
it to the clinico-pathological data we obtained from play a modulatory role.
patients. Interestingly in ectopic endometrial lesions
Fig. 1
Immunoexpression of PPAR-γ in ectopic endometrium (endometriotic lesions)
Dysmenorrhea
10 r = 0.6588
p = 0.0198
8
6
4
2
0 20 40 60 80 100
% of PPAR-γ positive cells
A Patient reporting no pain. B Patient reporting strong C Positive correlation between the percentage of
menstrual and generalised endometriotic cells staining positively for PPAR-γ and
lower abdominal pain. the menstrual pain level reported by the patients.
06 forum gynécologie suisse 3 | 11
Fig. 2
Epithelial Cells Stromal Cells
The high purity of endo-
Cytokeratin
metrial cell preparations
is shown by specific
staining of epithelial cells
for cytokeratin (A) and of
stromal cells for CD10 (F).
The commonly used
Vimentin
stromal marker vimentin
is less specific (C, D).
neurogenic inflammation and pain as well as being
upregulated at many sites of inflammation. Its most
CD10
potent ligand, substance P (SP), has been confirmed
in endometriotic tissue although the expression of
NK1 has not yet been examined in either eutopic or
ectopic endometrium. We therefore assessed NK1
expression in endometriotic lesions, and found that
87.5% of these were positive. Moreover, the NK1 ex- Fig. 3
pression level was related to the menstrual pain
Application of the endometrial stromal cell culture model
reported by women with endometriosis. A direct re-
lationship between PPAR-γ and NK1 in endometrial A Immunofluorescence
tissue has not yet been investigated, however this staining of cultured stromal
cells. Green staining is a
data suggests PPAR-γ agonists may, via NK1 protec- stromal cell marker (CD44v7),
tion, reflect a potential target for the modulation of where blue is a nuclear DAPI
pain in endometriosis. stain. Bar = 100μm.
The ablation of the ectopic endometrial tissue, the
lesion, and its accompanying reduction in pain is a
significant goal. On the other hand, the maintenance
or restoration of fertility is desired, requiring an in-
tact cyclic function of the endocrine environment B Treatment of endometrial
and the eutopic (intra-uterine) endometrium. To ex- stromal cells treatment with
Ciglitazone. Red staining
amine the effect TZD drugs had on endometrium, shows GLUT1 transporters.
and potentially fertility, an in vitro eutopic endome- Blue = nuclear DAPI stain.
trial stromal cell model was developed. The glucose
metabolism of endometrial tissue is an important
factor in fertility. Energy requirements increase, glu-
cose regulation in stromal cell decidualisation and
blastocyst implantation is tightly controlled. Glucose
metabolism and the altered expression of glucose
membrane transporters (GLUT1 and 3) have been
implicated in idiopathic infertility. Given the ability
of TZD drugs to regulate glucose homeostasis in receptor blocking agent. We found that TZDs do not
type II diabetes patients we examined their effect on in fact affect the intracellular production of inflamma-
the endometrium using the in vitro model described. tory cytokines, but rather modulated their secretion
We found that some TZD drugs affect glucose uptake from the cell. Significantly, the reduction in cytokine
and homeostasis in endometrial stromal cells through secretion also occurred when PPAR-γ receptors were
what is likely an increased expression in GLUT1 mem- blocked, suggesting that modulation of the PPAR-γ
brane transporter expression. The mechanism of this receptor was not responsible for the decrease in cy-
regulation and whether it impacts on fertility de- tokine secretion.
serves further attention.
It is not yet clear how this reduction in cytokine se-
The primary endometrial stromal cell culture model cretion occurs, however one possibility that we have
was also used to test the role of PPAR-γ activation in been investigating is that TZD analogues induce
the reduction of the inflammatory response; for this stress on the endoplasmic reticulum. The endoplas-
both the production and the secretion of cytokines mic reticulum is responsible not only for assembling
under TZD influence was studied with and without proteins from amino acid precursors according to
pre-treatment of the culture with a specific PPAR-γ the RNA template, but also to ensure tertiary modi
07 forum gynécologie suisse 3 | 11
SCIENCES
fication, such as protein folding or glycosylation, in marker, human epididymis (specific) protein-4 (HE-4).
an efficient and organized manner. Stress on the en- In a small project supported by Fujirebio (Sweden) we
doplasmic reticulum induces the unfolded protein are planning to compare these two molecules for
response, which results in proteins being sent to- their potential to assess hormonal treatment prog-
wards degradation pathways rather than secreted nosis in endometriosis patients and to identify their
from the cell. The unfolded protein response results subgroup of women who are at an increased risk to
in an initial reduction in protein secretion and if left develop ovarian cancer.
unchecked, the initiation of apoptosis. We have
found that some TZD’s have the ability to initiate en- The exact mechanism through which inflammation
doplasmic reticulum stress and consequently cell stimulates tumor development is not yet clear, but
death. More importantly we have found that this re- it is known to affect several hallmarks of cancer,
sponse is analogue specific. We postulate therefore such as angiogenesis. Angiogenesis is an early step
that some TZD’s actually stimulate a reduction in en- in malignant transformation as new vasculature is
dometriotic lesions via an induction of cell death needed to provide tumors with nutrients and growth
through endoplasmic reticulum stress, rather than factors. The «angiogenic switch»; the progression
activation of the PPAR-γ receptor. A better under- from an avascular to vascular tumor phenotype is
standing of the mechanism of action of the TZD’s essential for tumor growth beyond 1– 2 mm2 and is
may be useful in designing analogues that are spe- thought to begin in the pre-malignant stage of most
cifically designed for endometriotic lesion ablation. cancers.
A better knowledge of the biology of endometriosis Inflammation stimulates angiogenesis through the
might also help to recognize certain similarities be- cytokine induced activation of both the NFκB and
tween endometriosis and cancer and understanding mTOR signal transduction pathways that stimulate
the relationship between endometriosis and ovarian transcription and translation of VEGF. As endome
cancer may provide an insight to early triggers of ma- triosis diagnosis occurs on average 3 to 11 years after
lignant transformation and thus potential markers onset the peritoneal environment is exposed to
for early diagnosis. This is another focus of our re- inflammatory mediators during extended periods.
search area. Therefore it is possible that the long-term inflamma-
tory environment created by endometriosis increases
Endometriosis and ovarian cancer the risk of women, who may already have an aber-
An association between endometriosis and cancer rant immune response, being subjected to extended
has been demonstrated; for the epithelial endometri- cytokine exposure. We wish to study the link be-
oid this has been suspected as early as 1925. Several tween inflammatory cytokines and angiogenesis in
risk factors for ovarian carcinogenesis, such as pelvic both endometriosis and ovarian cancer. Although
inflammatory disease and incessant ovulation sup-
port a role for inflammation in ovarian cancer pathol-
ogy, whereas conditions that suppress ovulation and
the inflammatory reaction that accompanies it, such Studies on relationship
as pregnancy, lactation and the use of oral contra-
ceptives are associated with a reduced risk of ovarian between inflammation,
cancer. angiogenesis and ovarian
CA (cancer antigen)-125 is routinely used as a serum
tumor marker for the detection and more importantly cancer are initiated.
for the monitoring of ovarian cancer progress and re-
mission. The peritoneal fluid contains high concentra-
tion of this carbohydrate antigen, and the same is the
case for another, less well studied ovarian cancer
08 forum gynécologie suisse 3 | 11this project is still only in its infancy we have already
found that the expression of VEGF, the most potent
angiogenic factor, is expressed in significantly higher
concentrations in endometriotic lesions excised from
the ovary compared to lesions from either the recto-
vaginal septum or the peritoneal wall. High expres-
sion of VEGF in ovarian endometriotic lesions sug-
gests a predisposition towards angiogenesis for
these lesions, which may be related to the increased
risk of developing ovarian cancer if endometriotic
lesions are found growing on the ovary.
Finally, our research also focuses on the clinical as-
pects of endometriosis and endometriosis related
infertility. In a recent paper, we demonstrated that
patients with endometriosis have a poorer endome-
trium when hysteroscopy is performed (15).
Literature
1 2,3,7,8-Tetrachlorodibenzo-p-dioxin increases glycodelin 9 Correlation between symptoms of pain and peritoneal
gene and protein expression in human endometrium. fluid inflammatory cytokine concentrations in endome-
Mueller MD, Vigne JL, Streich M, Tee MK, Raio L, Dreher E, triosis. Scholl B, Bersinger NA, Kuhn A, Mueller MD.
Bersinger NA, Taylor RN. J Clin Endocrinol Metab (2005); Gynecol Endocrinol (2009); 25(11):701-6
90(8): 4809-15
10 Generalized expansion of nociceptive reflex receptive
2 Neutrophils infiltrating the endometrium express vascular fields in chronic pain patients. Neziri AY, Haesler S,
endothelial growth factor: potential role in endometrial Petersen-Felix S, Müller M, Arendt-Nielsen L, Manresa JB,
angiogenesis. Mueller MD, Lebovic DI, Garrett E, Taylor RN. Andersen OK, Curatolo M. Pain. (2010);151(3):798-805
Fertil Steril (2000) 74(1): 107-12
11 Effect of peritoneal fluid from endometriosis patients
3 Immunobiology of endometriosis. Lebovic DI, Mueller MD, on neuroblastoma cells in culture. Bersinger NA, Brod-
Taylor RN. Fertil Steril (2001) 75(1): 1-10 beck MH, Jahns B, Mueller MD. Gynecol Endocrinol (2009);
25(11): 707-12
4 Outcome of laparoscopic ureterolysis for ureteral endome-
triosis. Ghezzi F, Cromi A, Bergamini V, Serati M, 12 Anti-angiogenic treatment of endometriosis: biochemical
Sacco A, Mueller MD. Fertil Steril (2006) 86 (2): 418-22 aspects. Taylor RN, Mueller MD Gynecol Obstet Invest.
(2004); 57(1): 54-6
5 Steroids and protein markers in the follicular fluid as indi-
cators of oocyte quality in patients with and without 13 PPAR-gamma receptor ligand induces regression of endo-
endometriosis. Wunder DM, Mueller MD, Birkhäuser MH, metrial explants in baboons: a prospective, randomized,
Bersinger NA. J Assist Reprod Genet (2005) 22(6): 257-64 placebo- and drug-controlled study. Lebovic DI, Mwenda
JM, Chai DC, Mueller MD, Santi A, Fisseha S, D’Hooghe T.
6 Angiogenic factors in endometriosis. Taylor RN, Lebovic Fertil Steril. (2007); 88(4 Suppl): 1108-19
DI, Mueller MD. Ann N Y Acad Sci. (2002); 955: 89-100
14 PPAR-gamma expression in peritoneal endometriotic
7 Epithelial neutrophil-activating peptide 78 concentrations lesions correlates with pain experienced by patients.
are elevated in the peritoneal fluid of women with endo- McKinnon B, Bersinger NA, Huber AW, Kuhn A,
metriosis. Mueller MD, Mazzucchelli L, Buri C, Lebovic DI, Mueller MD. Fertil Steril (2010); 93(1): 293-6
Dreher E, Taylor RN. Fertil Steril (2003); 79 Suppl1: 815-20
15 The hysteroscopic view of infertility: the mid-secretory
8 PAPP-A and osteoprotegerin, together with interleukin-8 endometrium and treatment success towards pregnancy.
and RANTES, are elevated in the peritoneal fluid of women Santi A, Bersinger NA, Felser R, Wunder DM, McKinnon B,
with endometriosis. Bersinger NA, Von Roten S, Wunder Mueller MD. Gynecol Surg (2011): in press
DM, Raio L, Dreher E, Mueller MD. Am J Obstet Gynecol
(2006); 195(1):103-8
09 forum gynécologie suisse 3 | 11P ratiques m E dicales et formation continue
La salpingectomie permet-elle d’éviter
le cancer de l’ovaire ?
L’épithélium de surface de l’ovaire est considéré comme le site d’où prennent
naissance les cancers épithéliaux de l’ovaire. Plusieurs travaux montrent toutefois
que l’origine du carcinome séreux ovarien serait l’épithélium des franges tubaires.
Ces informations sont essentielles car elles nous conduisent à nous focaliser sur
la compréhension de nouveaux mécanismes de carcinogenèse qui pourrait aboutir
à la prévention potentielle du cancer gynécologique le plus meurtrier.
D r Cesar Jaton Médecin-assistant, Hôpital de Nyon, GHOL
Le cancer de l’ovaire représente la quatrième cause Connaissances actuelles du carcinome tubaire :
de décès par cancer chez la femme dans les pays une pathologie qui devra être révisée.
industrialisés. En Suisse, on compte environs 700 Le cancer primitif de la trompe est considéré comme
nouveaux cas par année, dont plus des deux tiers le plus rare des cancers du tractus génital féminin.
découverts à un stade avancé. Le pronostic n’a été Son incidence annuelle aux États-Unis est estimée
que peu amélioré ces dernières années. à 0.41 pour 100 000 femmes. Le diagnostic repose sur
des critères histologiques rarement remplis, qui in-
Le carcinome séreux papillaire de haut grade, cou- cluent la présence de la tumeur principale dans la
ramment associé à un stade avancé au moment trompe et provenant de l’endosalpinx ; une morpho-
du diagnostic, est la forme la plus fréquente et repré- logie reproduisant un phénotype similaire à la mu-
sente approximativement 70 % des tumeurs épithé- queuse tubaire ; la mise en évidence d’une transition
liales de l’ovaire. entre l’épithélium tubaire normal et pathologique
(en particulier si la paroi tubaire est envahie) ; ainsi
Le carcinome séreux de haut grade : qu’une proportion moindre de tumeur sur l’ovaire ou
est-il une entité distincte ? l’endomètre que sur la trompe. (1, 2)
Parmi les tumeurs épithéliales de l’ovaire, on distingue
les tumeurs de bas grade (type endométrioïde, muci- Dans les cas de tumeurs séreuses pelviennes, il est
neux, à cellules claires, séreux de bas grade et border- souvent impossible d’identifier, macroscopiquement
line) et les tumeurs de haut grade (principalement de autant qu’histologiquement, le site primaire de la
type séreux ou indifférencié). Ces dernières sont plus néoplasie en raison de l’étendue des lésions au mo-
agressives et responsables d’une majeure partie des ment du diagnostic.
décès liés au cancer de l’ovaire. Les altérations géné-
tiques de ces deux groupes sont différentes, les car- Quelles sont les leçons tirées des patientes
cinomes de bas grade étant associés à une certaine présentant une prédisposition BRCA ?
stabilité génétique ainsi qu’à des mutations des La salpingo-ovariectomie prophylactique chez les
gènes KRAS et BRAF. Ils ne présentent que rarement patientes porteuses des gènes BRCA1 et BRCA2
des altérations du gène p53, mutation principale- a contribué à améliorer notre compréhension des
ment retrouvée dans le carcinome de haut grade. lésions précurseurs du cancer de l’ovaire. L’examen
de ces pièces à permis de mettre à jour des lésions
Contrairement à la majorité des tumeurs épithéliales, tubaires de type séreuses et non invasives appelées
où les différents stades de la séquence épithélium carcinomes tubaires intra-épithéliaux (TIC). Ces « pré-
normal-cancer se retrouvent au niveau de modifica- cancers » partagent l’altération génétique prédo
tions génétiques menant à la formation d’une cellule minante dans les carcinomes séreux de haut grade
tumorale, aucune lésion précancéreuse ovarienne (p53), indiquant donc la possibilité d’une relation
menant au carcinome ovarien de haut grade n’a en-
core été mise en évidence. (1)
10 forum gynécologie suisse 3 | 11Carcinome séreux primaire de la trompe
de Fallope. Développée dans la muqueuse,
la tumeur prolifère dans la lumière et in-
filtre la musculeuse tubaire.
entre ces deux entités. (3) De plus, l’étude histolo-
gique des trompes dans le cas de carcinomes pel-
viens a montré que ces lésions sont fréquentes, étant
détectées dans plus de la moitié des cas de carci-
nomes pelviens de haut grade classés selon les cri- Zusammenfassung
tères standards comme étant d’origine ovarienne ou
péritonéale. On les retrouve exclusivement en asso- Das Ovarialkarzinom liegt als Todesursache bei der Frau
ciation avec le sous-type séreux de haut grade et an vierter Stelle. Ca. 700 neue Fälle werden jährlich diag-
avec une fréquence élevée de localisation au niveau nostiziert, über zwei Drittel in einem fortgeschrittenen
des franges tubaires. (4) Ces conclusions sont super- Stadium. Die Prognose hat sich in den vergangenen Jahren
posables dans des groupes de patientes non por- nicht wesentlich verbessert. Bisher wurde angenommen,
teuses des mutations BRCA. dass das Oberflächenepithel des Ovars Ausgangspunkt ist
für die Entstehung eines Karzinoms. Neuere Untersuchun-
Récemment, l’étude oncomoléculaire de l’épithé- gen lassen vermuten, das Epithel der Tubenzotten könnte
lium tubaire non néoplasique a permis d’isoler une der Ursprungsort des serösen Ovarialkarzinoms sein. Es
altération précoce, dénommé p53 signature. Cette stellt sich deshalb die Frage, ob anlässlich einer konservati-
dernière partage certaines caractéristiques com- ven Hysterektomie eine prophylaktische Salpingektomie
munes avec le carcinome séreux de haut grade, à durchgeführt werden soll. Da bisher keine Beweise vor
savoir le type de cellules impliquées (cellules sé liegen, wird am Universitätsspital in Genf den Patientinnen
crétoires) et l’évidence d’altération de l’ADN. (5) Elle die Sachlage erklärt und auf ihren Wunsch, anlässlich einer
pourrait constituer une étape clé du modèle onco- Hysterektomie oder einer Tubenligatur eine Salpingek
génétique des carcinomes séreux de haut grade. tomie vorgenommen. Prospektive Studien werden zeigen
Paradoxalement, elle est retrouvée avec la même müssen, ob eine Tubenablation als Prophylaxe des Ovarial-
fréquence dans les cas BRCA que dans les cas karzinoms geeignet ist und welche Folgen dies hat. Ferner
contrôles, mais plus fréquemment et de manière wird die Frage zu klären sein, ob eine Ovarektomie bei
multifocale dans les trompes contenants un carci- BRCA-positiven Frauen notwendig ist oder ob die Salping-
nome tubaire intra-épithélial. Par la même séquence ektomie genügt.
d’événements, le carcinome séreux pourrait égale-
ment se développer à partir de lésions ovariennes
d’endosalpingiose. (4)
Les facteurs de risque du cancer de l’ovaire
revisités
L’incessant ovulation hypothesis de Fathalla et la
gonadotrophin hypothesis de Cramer placent l’épi-
thélium ovarien de surface au centre de la formation
des cancers ovariens épithéliaux. Shannon et al (6),
quant à eux, affirment que le carcinome séreux de
11 forum gynécologie suisse 3 | 11P ratiques m E dicales et formation continue
Tab. 1
Facteurs protecteurs contre le cancer de l’ovaire (exception : première grossesse tardive)
Intervention Théorie de l’ovulation Théorie inflammatoire
incessante
Pilule (inhibiteur de l’ovulation) Diminution des microtraumatismes Diminution des infections
épithéliaux ovariens ascendantes par épaississement
(anovulation) de la glaire cervicale
Diminution du flux menstruel rétro-
grade par atrophie endométriale
Grossesse Diminution des microtraumatismes Diminution des infections
épithéliaux ovariens (anovulation) ascendantes
Diminution de l’exposition tubaire
aux médiateurs inflammatoires
menstruels
Stérilisation tubaire Diminution des microtraumatismes Interruption de l’exposition
épithéliaux ovariens par diminu- tubaire aux médiateurs inflamma-
tion de la vascularisation anne- toires menstruels
xielle (anovulation relative)
Hystérectomie Diminution des microtraumatismes Interruption de l’exposition tubaire
épithéliaux ovariens par diminution aux médiateurs inflammatoires
de la vascularisation annexielle menstruels
(anovulation relative)
Première grossesse tardive Facteur de risque : Microtraumatis- Facteur protecteur : Diminution de
mes épithéliaux ovariens fréquents l’exposition aux médiateurs inflamm-
(ovulations) atoires par affaiblissement tardif
du col utérin
haut grade proviendrait non pas de l’ovaire mais de contre le cancer ovarien tel que l’utilisation prolon-
la trompe et proposent un modèle basé sur l’associa- gée (plus de 5 ans) d’un contraceptif oestro-proges-
tion entre inflammation et cancer pour expliquer tatif, la grossesse, la stérilisation tubaire ainsi que
son développement. l’hystérectomie peuvent également être expliqués
par ce modèle (Tableau 1).
D’une part, les macrophages, absents de l’épithélium
ovarien, rendent la muqueuse tubaire plus sensible Faut-il proposer une salpingectomie lors
aux phénomènes d’inflammation chronique. Leur d’hystérectomie conservatrice des annexes?
présence est prédominante au niveau du pavillon. Si l’origine du « cancer de l’ovaire » séreux de haut
D’autre part, outre les infections ascendantes, le flux grade est tubaire, il devient légitime de se poser la
menstruel rétrograde expose cette dernière à de question de prévention de ce cancer par une abla-
nombreux médiateurs de l’inflammation (IL-8, IL-12, tion des trompes.
TNF-α). La réaction inflammatoire peut être à l’ori-
gine de lésions qui peuvent endommager le matériel L’hystérectomie et la stérilisation tubaire sont des
génétique et favoriser la survenue de mutation cel- opérations gynécologiques courantes qui laissent
lulaire. Les franges tubaires, lieu privilégié du déve- dans la majorité des cas les trompes ou des frag-
loppement des carcinomes, présentent contraire- ments de ces dernières in situ (dans les pays indus-
ment à l’épithélium ovarien une importante étendue, trialisés, 15 à 20 % des femmes souffrant d’un cancer
rendant le phénomène plus fréquent. Leurs proximi- de l’ovaire ont un antécédent d’hystérectomie ou
tés avec le péritoine et la transition entre épithélium de stérilisation tubaire). En dépit du fait qu’il faille
Müllerian et mésothélium offrent également à cette probablement réaliser un grand nombre de salpin-
région jonctionnelle une certaine plasticité cellu- gectomies pour éviter un futur cancer, force est de
laire. Finalement, les facteurs protecteurs reconnus constater que ce geste ne représente qu’un faible
risque chirurgical, probablement grevé d’une morbi-
dité mineure.
12 forum gynécologie suisse 3 | 11L’état des connaissances actuelles ne permet pas de Bibliographie
statuer de manière définitive quant à l’origine tu- 1 Levanon K, Crum C, Drapkin R. New insight into the patho-
genesis of serous ovarian cancer and its clinical impact.
baire du cancer séreux de l’ovaire. L’attitude pragma- J Clin Oncol 2008; 26(32): 5284-93.
tique adoptée aux HUG et au GHOL est de présenter
les connaissances actuelles sur l’origine présumée 2 Benedet JL, Bender H, Jones H 3rd, Ngan HY, Pecorelli S.
FIGO staging classifications and clinical practice guidelines
du cancer ovarien ; si les patientes le souhaitent, une in the management of gynecologic cancers. FIGO Commit-
salpingectomie est effectuée lors d’hystérectomie tee on Gynecologic Oncology. Int J Gynecol Obstet 2000;
simple ou de stérilisation tubaire. 70(2): 209-62.
3 Medeiros F, Muto MG, Lee Y, Elvin JA, Callahan MJ et al.
Perspectives The tubal fimbria is a preferred site for early adenocarci-
Des études prospectives doivent encore êtres réa noma in women with familial ovarian cancer syndrome.
Am J Surg Pathol 2006; 30(2): 230-6.
lisées afin de confirmer que l’ablation des trompes
apporte un réel bénéfice en termes de prévention 4 Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A,
du cancer ovarien, et l’évidence doit statuer définiti- Lee Y. Lessons from BRCA: The tubal frimbria emerges as
an origin for pelvic serous cancer. Clin Med Res 2007; 5(1):
vement sur la place de la salpingectomie « de rou- 35-44.
tine » ainsi que sur l’impact d’une telle mesure.
5 Lee Y, Miron A, Drapkin R, Nucci MR, Medeiros F et al. A
candidate precursor to serous carcinoma that originates
De plus, l’ablation prophylactique des ovaires chez in the distal fallopian tube. J Pathol 2007; 211(1): 26-35.
les patientes porteuses de mutations BRCA est-elle
nécessaire ou peut-on se limiter à une simple sal 6 Salvador S, Gilks B, Köbel M, Huntsman D, Rosen B, Miller
D. The fallopian tube: primary site of most pelvic high-
pingectomie bilatérale ? Le syndrome du cancer du grade serous carcinomas. Int J Gynecol Cancer 2009; 19(1):
sein/ovaire héréditaire est sous-diagnostiqué en 58-64.
Suisse, et certains auteurs estiment qu’environs 3500
femmes âgées de 25 à 70 ans seraient concernées.
Différents modèles ont été développés afin d’évaluer
le risque d’une prédisposition génétique, et l’anam-
nèse oncologique reste l’outil principal de stratifica-
tion de ce risque. L’analyse systématique des pièces
d’annexectomie pourrait-elle permettre, de manière
complémentaire et par la mise en évidence de lésions
précurseurs, de démasquer ces patientes à risque, et
par ce biais de mettre en place des stratégies de sur-
veillance influant ainsi sur la mortalité d’autres can-
cers gynécologiques ?
Nous remercions le Pr P. Petignat et le Dr F. Dreher
pour leur lecture critique, leurs conseils et leur dispo-
nibilité.
13 forum gynécologie suisse 3 | 11Sie können auch lesen